Chapter 19 The Neurologic System






A. Mental Status Examination
5 What are the snouting, rooting, and sucking reflexes?



10 What are the most important levels of consciousness? How do they deteriorate?
There are four levels of consciousness. In increasing degree of deterioration they are:
 Alertness: An awake person with normal level of consciousness (alert patient)
Alertness: An awake person with normal level of consciousness (alert patient)
 Lethargy: A sleepy patient who needs continuous stimulation to remain awake
Lethargy: A sleepy patient who needs continuous stimulation to remain awake
 Stupor: An unarousable patient who can still moan, withdraw, or roll around during exam
Stupor: An unarousable patient who can still moan, withdraw, or roll around during exam
 Coma: A patient who offers no purposeful response to stimulations of any kind
Coma: A patient who offers no purposeful response to stimulations of any kind
12 What is memory? How do you assess it?
Memory is the ability to register and recall prior sensory input. For testing purposes:


(1)Language
22 What is cerebellar speech?
Another disorder of articulation of sound, rather than ideation or perception (ataxic speech).
23 Beside cerebellar speech, what are the two most important types of dysarthria?
 Spastic dysarthria. This is due to damage of upper motor neurons (connecting the cortex to the spine), resulting in excessive and uncontrolled tone.
Spastic dysarthria. This is due to damage of upper motor neurons (connecting the cortex to the spine), resulting in excessive and uncontrolled tone.
 Flaccid dysarthria. This is due instead to damage of lower motor neurons, compromising all aspects of speech production. Lesions of individual cranial nerve(s) (brain stem stroke or peripheral facial nerve paralysis) also can cause dysarthria. For instance, Bell’s palsy may cause difficulty in saying “mo-mo-mo” (see Table 19-1).
Flaccid dysarthria. This is due instead to damage of lower motor neurons, compromising all aspects of speech production. Lesions of individual cranial nerve(s) (brain stem stroke or peripheral facial nerve paralysis) also can cause dysarthria. For instance, Bell’s palsy may cause difficulty in saying “mo-mo-mo” (see Table 19-1).
Table 19-1 Dysarthria and Possible Cranial Nerve Involvement
| Syndrome | Sounds | Possible Cranial Nerve Involved |
|---|---|---|
| Labial | “mo-mo-mo” | CN VII (facial nerve) |
| Lingual | “la-la-la-la” | CN XII (hypoglossal nerve) |
| Pharyngeal | “ka-ka-ka” | CN IX and X (glossopharyngeal nerve and vagus nerve) |
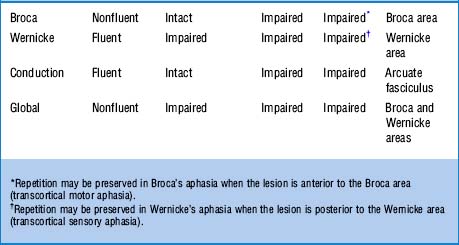
25 What are the most important defects in aphasia?



26 What are the clinical differences between fluent and nonfluent aphasia?
 In fluent aphasia (Wernicke’s), talking is easy, but words are often jumbled and meaningless. There is difficulty in naming objects, repeating sentences, or comprehending. Speech is full of emptiness and gibberish “jargon,” even though patients seem unaware of it. In fact, they may even appear confused and almost psychotic. Reading impairment parallels the speech deficit. The responsible lesion is in the temporal or parietal lobe.
In fluent aphasia (Wernicke’s), talking is easy, but words are often jumbled and meaningless. There is difficulty in naming objects, repeating sentences, or comprehending. Speech is full of emptiness and gibberish “jargon,” even though patients seem unaware of it. In fact, they may even appear confused and almost psychotic. Reading impairment parallels the speech deficit. The responsible lesion is in the temporal or parietal lobe.

31 What is cortical dementia? What is subcortical dementia?


B. Cranial Nerves Examination
35 How do you test CN I (olfactory nerve)?
By asking patients to close their eyes, occlude one nostril, and then smell through the open naris a distinctive scent—like cinnamon, cloves, or peppermint. Transient anosmia is common, usually resulting from simple colds or intercurrent sinus infection. Chronic anosmia (especially if congenital) is instead quite important (see Chapter 6, question 33). Note that anosmia can also be seen in frontal/temporal lobectomies or Parkinson’s disease.
36 How do you test CN II (optic nerve)?
 Visual acuity:Ask the patient to read an eye chart from a distance of 20 feet. Glasses or contacts are allowed, since the test measures the best corrected vision. A normal person reads at 20 feet letters that others also can read at 20 feet (20/20 vision). A person who reads at 20 feet letters that others can read at 40 is said to have an acuity of 20/40 (see Chapter 4, questions 1–15).
Visual acuity:Ask the patient to read an eye chart from a distance of 20 feet. Glasses or contacts are allowed, since the test measures the best corrected vision. A normal person reads at 20 feet letters that others also can read at 20 feet (20/20 vision). A person who reads at 20 feet letters that others can read at 40 is said to have an acuity of 20/40 (see Chapter 4, questions 1–15).
 Visual fields: Their assessment can localize damage anywhere from the retina to the occipital lobes, resulting in loss of vision of only a discrete area (or field). The best way to detect visual cuts is by confrontation: place yourself head-to-head and eye-to-eye with the patient, while both of you occlude the opposite eye (because while looking into each other’s eyes, both you and the patient have the same peripheral vision). To determine whether the patient can see what you see, move objects into his/her peripheral vision, starting from above, then below, then left and right. Patients should be able to see the objects at the same time you do. If they cannot, they probably have a visual cut corresponding to a particular region of peripheral vision (see Chapter 4, questions 20–35).
Visual fields: Their assessment can localize damage anywhere from the retina to the occipital lobes, resulting in loss of vision of only a discrete area (or field). The best way to detect visual cuts is by confrontation: place yourself head-to-head and eye-to-eye with the patient, while both of you occlude the opposite eye (because while looking into each other’s eyes, both you and the patient have the same peripheral vision). To determine whether the patient can see what you see, move objects into his/her peripheral vision, starting from above, then below, then left and right. Patients should be able to see the objects at the same time you do. If they cannot, they probably have a visual cut corresponding to a particular region of peripheral vision (see Chapter 4, questions 20–35).
37 How do you test CN III, IV, and VI?
Together, since oculomotor (III), trochlear (IV), and abducens (VI) work in concert to produce the various eye movements. To test them, ask patients to hold the head stationary while following your finger as it moves through the main directions of gaze: left-up, left-middle, left-down, and right-up, right-middle, and right-down. Normal eyes move symmetrically and smoothly. Any restriction or double vision (from inability of the eyes to move together) suggests damage to III, IV, or VI (see Chapter 4, questions 84–90).
38 What abnormal eye movements result from damage to CN III, IV, or VI?
 The oculomotor supplies medial, superior, and inferior rectus; inferior oblique; and levator palpebrae (which raises the eyelid). It also contains parasympathetic fibers that constrict the pupil. Hence, its lesions result in a partially abducted eye that is difficult to adduct, raise, or lower. In fact, it is frequently turned out (exotropia). There also is a drooping eyelid (ptosis) and a pupil that may be larger (mydriatic) and difficult to constrict. In more subtle cases, there may only be diplopia or blurred vision. A CN III palsy that spares the pupils (i.e., ptosis, and external rotation of the globe, but symmetric and equally reactive pupils) suggests diabetes, but also vasculitides and multiple sclerosis.
The oculomotor supplies medial, superior, and inferior rectus; inferior oblique; and levator palpebrae (which raises the eyelid). It also contains parasympathetic fibers that constrict the pupil. Hence, its lesions result in a partially abducted eye that is difficult to adduct, raise, or lower. In fact, it is frequently turned out (exotropia). There also is a drooping eyelid (ptosis) and a pupil that may be larger (mydriatic) and difficult to constrict. In more subtle cases, there may only be diplopia or blurred vision. A CN III palsy that spares the pupils (i.e., ptosis, and external rotation of the globe, but symmetric and equally reactive pupils) suggests diabetes, but also vasculitides and multiple sclerosis.


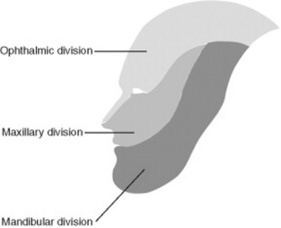
39 How do you test CN V (trigeminal nerve)?
It depends on whether you are testing a motor or sensory component. The divisions of the trigeminal nerve are shown in Figure 19-1.
 The sensory component is predominant, providing pain, tactile, and thermic sensations to the face. Note that sensation to the tragus, most of the external ear, and angle of the jaw is not trigeminal and thus is preserved in diseases of the V (it is supplied instead by cervical sensory roots).
The sensory component is predominant, providing pain, tactile, and thermic sensations to the face. Note that sensation to the tragus, most of the external ear, and angle of the jaw is not trigeminal and thus is preserved in diseases of the V (it is supplied instead by cervical sensory roots).

40 Where are the sensory and motor nuclei of the trigeminal nerve?
They are both in the pons. Yet the sensory also extends into the cervical cord.
41 How do you test the sensory function of CN V?
By pinprick or light touch over the areas of distribution of the trigeminal branches: upper (supplied by V1, or ophthalmic; forehead), mid (V2, or maxillary; cheek), and lower (V3, or mandibular; jaw). Sensory function of the ophthalmic branch is also tested by the corneal reflex (see question 58).
42 How do you test the motor function of CN V?
By feeling the masseters during teeth clinching. Contraction must be strong and symmetric.
45 What is the significance of a sensory deficit of the trigeminal nerve?
It depends on whether it involves both the face and body, or only the face:


47 What is the jaw-jerk reflex?
A reflex that tests the integrity of sensory (afferent) and motor (efferent) components of the V. To test for it, place your index finger (or tongue depressor) over the patients’ chin, while asking them to keep their mouth slightly open. Then, gently tap the index finger with your reflex hammer. Abnormal responses include jaw deviation or brisk closure. Exaggerated masseteric contraction, often with clonus, suggests upper motor neuron pathology (i.e., above the trigeminal nucleus in the mid-pons). This occurs in 70% of pseudobulbar palsy patients (see below, question 65).
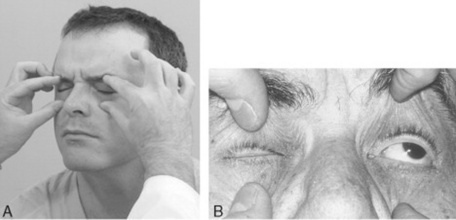
48 How do you test CN VII (facial nerve)?
Through the muscles of facial expression. Damage to CN VII causes inability to wrinkle the forehead, tightly close the eye (Fig. 19-2), or smile. It also causes facial asymmetry (i.e., ipsilateral widening of the palpebral fissure and sagging of the nasolabial fold).
60 How do you test CN VIII (acoustic/vestibular nerve)?
It depends on the function you want to test, vestibular or auditory:
 Vestibular function should be assessed by the Romberg, positional vertigo, and caloric irrigation tests only in cases of vertigo and dizziness.
Vestibular function should be assessed by the Romberg, positional vertigo, and caloric irrigation tests only in cases of vertigo and dizziness.
 Auditory function may instead be compromised in very subtle ways. Hence, the need for routine testing. This can be simply done by asking patients if they can hear whispered words, the soft noise of a ticking watch, or fingers rubbing against each other near the ear. Conductive and sensorineural hearing loss can be separated by Rinne and Weber tests (see Chapter 5, questions 59–65).
Auditory function may instead be compromised in very subtle ways. Hence, the need for routine testing. This can be simply done by asking patients if they can hear whispered words, the soft noise of a ticking watch, or fingers rubbing against each other near the ear. Conductive and sensorineural hearing loss can be separated by Rinne and Weber tests (see Chapter 5, questions 59–65).
64 What is the anatomy of CN IX (glossopharyngeal) and CN X (vagus)? How do you test them?
Axons from several brain stem nuclei mingle together to emerge from the neuraxis through two separate nerves, named by early neuroanatomists as glossopharyngeal (IX) and vagal (X) (the vagus was so termed since, as a vagabond, it wanders long distances in the body). In reality, the origin of the two nerves is essentially identical. Function also is similar: motor control of the palate and pharynx (plus, for the IX, sensory supply to the pharynx and posterior third of the tongue). Hence, their clinical testing is not entirely separable. Since the brain stem nuclei of these two nerves receive bilateral innervation from the cortex, their dysfunction results from one of three possibilities: (1) bilateral damage to the cortex or pyramidal tracts (pseudobulbar palsy), (2) brain stem disease (lateral medullary syndrome), or (3) peripheral nerve lesions (jugular foramen syndrome). You can test IX and X by asking patients to say “ahhh” or “ehhh” (see Chapter 6, questions 53 and 54) while observing whether the velum of the palate rises symmetrically. Alternatively, you can use the gag and palatal reflexes. The latter is elicited by touching the patient’s palate with a cotton swab, which causes elevation of the soft palate and ipsilateral deviation of the uvula. The gag is instead triggered by touching the posterior wall of the pharynx (or alternatively, the tonsillar area or base of the tongue). It causes tongue retraction and elevation/constriction of the pharyngeal musculature. In unilateral CN IX and X paralysis, these reflexes result in deviation of the uvula toward the normal side. Lesions of the IX also will result in loss of taste in the posterior third of the tongue, and loss of pain and touch sensations in the same area plus the soft palate and pharyngeal walls. Conversely, unilateral paralysis of CN X’s recurrent laryngeal nerve will cause hoarseness. Bilateral paralysis will cause stridor (requiring tracheostomy).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


