Chapter 12 Heart Murmurs
Introduction and Basic Issues
Table 12-2 Classification of Murmurs Described in This Chapter*
| A. Functional (27–65) | B. Systolic (66–194) | C. Diastolic (197–258) |
|---|---|---|
| Systolic | Semilunar Ejection | Atrioventricular Stenosis |
| • Still’s murmur (46–50) | • Aortic stenosis | • Mitral stenosis (197–209) |
| • Valvular (82–115) | ||
| • Subvalvular hyper-trophic (116–128) | ||
| • Subvalvular “fixed” (129) | ||
| • Supravalvular (130) | ||
| • Pulmonary systolic ejection murmur (51) | • Pulmonic stenosis (132–133) | • Mitral diastolic flow murmur (210) |
| • Supraclavicular arterial bruit (52) | • Ventricular septal defect (134–138) | • Tricuspid stenosis (211–212) |
| • Aortic sclerosis (56–65) | • Tricuspid diastolic flow murmur (213–215) | |
| Continuous | AV Regurgitation | Semilunar Regurgitation |
| • Venous hum (53) | • Mitral regurgitation (142–170) | • Aortic regurgitation (216–251) |
| • Mammary soufflé (54) | • Mitral valve prolapse(171–184) | • Pulmonic regurgitation (252–258) |
| • Tricuspid regurgitation (185–194) | ||
| Diastolic | ||
| • Very rare, and always associated with either S3 or a diastolic rumble (33–34) |
* Not including continuous extracardiac murmurs like that of patent ductus arteriosus. The numbers in parentheses refer to the pertinent questions.
Cardiac auscultation is the centerpiece of physical diagnosis, and recognizing murmurs is its most challenging aspect. It requires the identification of sounds jam-packed in less than 0.8 second, often overlapping, and not infrequently at the threshold of audibility. Stethoscopy is like learning a musical instrument and similarly rewarding. Hence, despite being as old as the battle of Waterloo, this little tool and its skillful use still occupy an important role in 21st-century medicine.
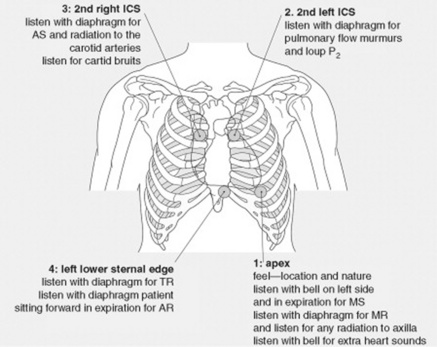
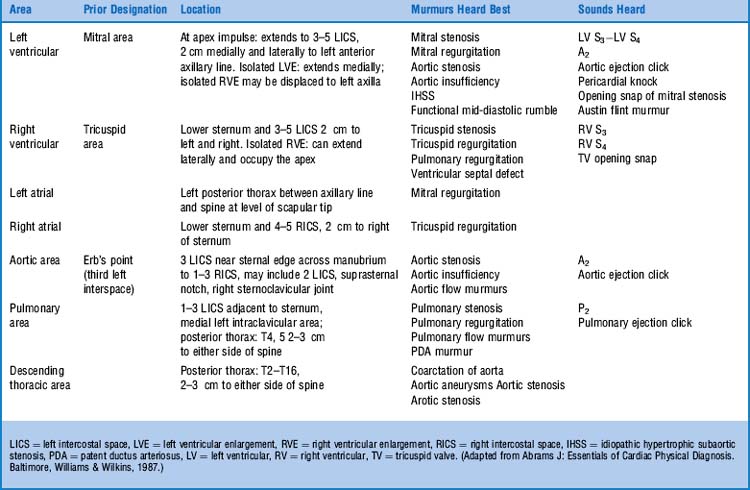
1 What are the auscultatory areas of murmurs?
The classic ones are shown in Fig. 12-1 and Table 12-1. Auscultation typically starts in the aortic area, continuing in clockwise fashion: first over the pulmonic, then the mitral (or apical), and finally the tricuspid areas. Since murmurs may radiate widely, they often become audible in areas outside those historically assigned to them. Hence, “inching” the stethoscope (i.e., slowly dragging it from site to site) can be the best way not to miss important findings.
5 What, then, should be the approach to a newly detected murmur?
The first step should be to use the cardiovascular exam to separate pathologic from functional murmurs (see below, questions 28–33). This is essential to avoid expensive and possibly dangerous laboratory tests. Then, if the murmur is identified as organic, the physical examination should provide clues to its site of origin, its hemodynamic cause, and, possibly, its severity.
Mechanisms of Production
9 What are the structural abnormalities that produce local narrowing and turbulent flow?
Any of the following abnormalities in the orifice through which blood flows:
 Abnormal size (the smaller the orifice, the greater the turbulence; the greater the turbulence, the louder the murmur). This phenomenon also may occur when blood moves from a small into a large space, such as a dilated aortic root.
Abnormal size (the smaller the orifice, the greater the turbulence; the greater the turbulence, the louder the murmur). This phenomenon also may occur when blood moves from a small into a large space, such as a dilated aortic root.
 Irregular shape (for example, an irregular valve opening)
Irregular shape (for example, an irregular valve opening)
 Irregular edge (the sharper the edge of the orifice, the higher the turbulence)
Irregular edge (the sharper the edge of the orifice, the higher the turbulence)
Classification
10 How are murmurs classified?
The first (and most important) separation is purely clinical: pathologic versus functional. The real classification, however, is based on the phase of the cardiac cycle where the murmur is located. Accordingly, murmurs are divided into systolic, diastolic, and continuous. This is clinically relevant, since diastolic and continuous murmurs are (almost) always pathologic, whereas systolic murmurs are often functional (Fig. 12-2).
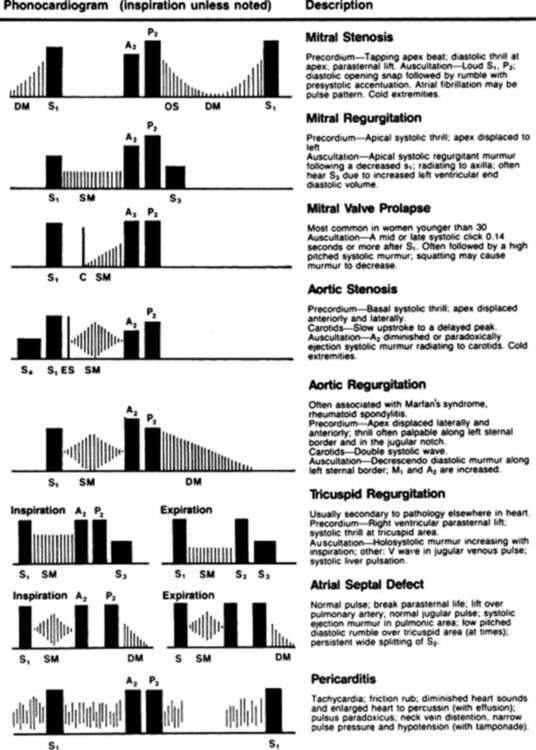
Figure 12-2 Phonocardiographic description of pathologic cardiac murmurs.
(From James EC, Corry RJ, Perry JF: Principles of Basic Surgical Practice. Philadelphia, Hanley & Belfus, 1987.)




14 Once the phase of the cardiac cycle has been identified, which other characteristics of a murmur should be analyzed and described?
1. The timing: Murmurs can span throughout systole (holosystolic) or diastole (holodiastolic), or they may occur only in the early, mid, or late phases of each interval:
 Systolic murmurs: Holosystolic and late systolic murmurs are clinically more important than early or mid-systolic murmurs because they are usually pathologic. Since benign systolic murmurs are flow generated, and since flow is maximal during the early part of systole, all benign systolic murmurs tend to be short and early peaking. They are never beyond S2. In fact, a murmur that touches S2 (whether holosystolic or late systolic) is pathologic and reflective of atrioventricular (A-V) regurgitation. Conversely, a murmur that occurs during the first half of systole (whether early or mid-systolic) is often benign and reflective of semilunar ejection. Hence, the longer the murmur, the worse the disease.
Systolic murmurs: Holosystolic and late systolic murmurs are clinically more important than early or mid-systolic murmurs because they are usually pathologic. Since benign systolic murmurs are flow generated, and since flow is maximal during the early part of systole, all benign systolic murmurs tend to be short and early peaking. They are never beyond S2. In fact, a murmur that touches S2 (whether holosystolic or late systolic) is pathologic and reflective of atrioventricular (A-V) regurgitation. Conversely, a murmur that occurs during the first half of systole (whether early or mid-systolic) is often benign and reflective of semilunar ejection. Hence, the longer the murmur, the worse the disease.
2. The intensity (or loudness): Traditionally graded by the Levine system from 1/6 to 6/6:
 1/6: A murmur so soft as to be heard only intermittently and always with concentration and effort. Never immediately.
1/6: A murmur so soft as to be heard only intermittently and always with concentration and effort. Never immediately.




18 Which interventions and maneuvers can be used at the bedside to modify the intensity and characteristics of murmurs and make them more easily recognizable?
22 What is the effect of Valsalva on sounds and murmurs?
Valsalva not only has important hemodynamic effects (that can be used for the recognition of congestive heart failure—see Chapter 2, questions 121–127), but may also elicit a diagnostic auscultatory response in patients with HOCM or mitral valve prolapse (MVP). This is mediated by a reduction in left ventricular diameter (caused by the strain), which in turn increases the left ventricular gradient of HOCM, thus intensifying its subvalvular systolic ejection murmur. This is the opposite of what happens to other murmurs of left ventricular outflow obstruction (such as, for example, valvular AS or PS), which instead soften with Valsalva (because of decreased venous return, with a resulting decrease in transvalvular gradients). The strain phase of Valsalva also anticipates the prolapse of a floppy mitral valve (by making the ventricle smaller, and thus “loosening up” the chordae tendineae). As a result, the click will occur earlier, and the murmur will lengthen. Hence, only two murmurs get enhanced by the straining phase of Valsalva: HOCM and MVP. In HOCM, the murmur gets louder, whereas in MVP it gets longer. Note that the release period of Valsalva may have opposite effects, based on the site of origin of the acoustic event being examined: right-sided murmurs will generally revert to their baseline intensity within 2–3 cardiac cycles, whereas left-sided murmurs will instead take a little longer (up to 5–10 cardiac cycles).
A. Functional Murmurs
28 How can physical examination help differentiate functional from pathologic murmurs?
There are two golden and three silver rules.
1. The first golden rule is to always judge (systolic) murmurs like people: by the company they keep. Hence, murmurs that keep bad company (like symptoms; extra sounds; thrill; abnormal arterial or venous pulse, ECG, or chest x-ray) should be considered pathologic until proven otherwise. These murmurs should receive lots of evaluation, technology-based included.
2. The second golden rule is that a diminished or absent S2 usually indicates a poorly moving and abnormal semilunar valve. This is the hallmark of pathology. As a flip side, functional systolic murmurs are always accompanied by a well-preserved S2, with normal split.
3. The three silver rules are:



34 What are the causes of benign diastolic murmurs?
Rapid ventricular filling—very much like the physiologic S3. In fact, these benign diastolic murmurs are always associated with either a physiologic S3 or some other type of benign rumbling murmur of filling (like Still’s—see below, questions 46–50). They never occur in isolation.
35 What are the clinical implications of functional murmurs?





36 How common are these functional murmurs?
Extremely common. In young adults, systolic murmurs have a 5–52% prevalence, with echocardiography being normal in 86–100%. They also are extremely commonly in pregnant women, with as many as 80% having a benign ejection murmur during gestation. Finally, systolic murmurs are present in 29–60% of elderly medical outpatients or nursing home residents (see aortic sclerosis, questions 56–65), with echocardiography being normal in 44–100% of cases. Hence, functional murmurs are the most common heart murmurs encountered by the generalist. Indeed, each of us probably had a functional murmur at some point in life.
39 Is high flow velocity present in nonpediatric patients?
Yes. For example, in tachycardia, anemia, fever, or, quite simply, during and after exercise.
40 How significant is a murmur that appears only after exercise, anemia, or fever?
It might still be quite significant because:



43 What are the functional murmurs caused by reduced flow velocity?
The most common is aortic sclerosis, wherein the aorta is dilated and tortuous.
44 How many types of functional murmurs are known?
In order of frequency, the four systolic murmurs are:
 Precordial vibratory murmur (Still’s)
Precordial vibratory murmur (Still’s)
 Pulmonary ejection systolic murmur
Pulmonary ejection systolic murmur
 Supraclavicular (carotid) arterial bruit
Supraclavicular (carotid) arterial bruit

The first three occur in children and adolescents, whereas the fourth one is typical of the elderly.
The two functional continuous murmurs are:


45 What is the mechanism responsible for the generation of these functional murmurs?
It depends of the phase of the cardiac cycle:
 Functional systolic murmurs are due to rapid and vigorous ejection, across normal semilunar valves and into the large vessels. Because their site of origin is probably the large vessels themselves, these findings are loudest at the cardiac base (i.e., over the pulmonic [second to third left interspace] or aortic area [second to third right interspace]). Since the left ventricle generates higher pressures than the right, most functional systolic murmurs tend to occur over the aortic area.
Functional systolic murmurs are due to rapid and vigorous ejection, across normal semilunar valves and into the large vessels. Because their site of origin is probably the large vessels themselves, these findings are loudest at the cardiac base (i.e., over the pulmonic [second to third left interspace] or aortic area [second to third right interspace]). Since the left ventricle generates higher pressures than the right, most functional systolic murmurs tend to occur over the aortic area.


53 What is a venous hum?
It is a continuous and physiologic venous sound—not uncommon in children, but rare in adults. For a more extensive description, refer to Chapter 10, questions 120–123.
55 What can one do to sort out functional murmurs from pathologic ones?
1. Start with history, specifically:



2. Then continue with the physical examination, looking for clubbing and cyanosis and any abnormalities in the following areas of the cardiovascular exam:








3. Then carefully evaluate the murmur in its main characteristics, especially:







 Variations with Valsalva maneuver (remember that the pulmonary ejection, the Still’s murmur, and the venous hum all disappear with the onset of Valsalva, whereas the murmurs of HOCM and MVP increase—see question 22)
Variations with Valsalva maneuver (remember that the pulmonary ejection, the Still’s murmur, and the venous hum all disappear with the onset of Valsalva, whereas the murmurs of HOCM and MVP increase—see question 22)

4. Finally, gather simple laboratory tests (such as an electrocardiogram or a chest x-ray), and look for any associated “bad company.”
B. Systolic Murmurs
66 How common are systolic murmurs?
Extremely common, especially if ejection. Hence, the need to separate functional from pathologic.
67 What are the causes of a systolic murmur?
1. Ejection (i.e., increased “forward” flow over a semilunar valve). This can be:
 Physiologic: Normal valve, but flow high enough to cause turbulence (anemia, exercise, fever, and other hyperkinetic heart syndromes)
Physiologic: Normal valve, but flow high enough to cause turbulence (anemia, exercise, fever, and other hyperkinetic heart syndromes)
2. Regurgitation: “Backward” flow from a high- into a low-pressure bed. Although this is usually due to incompetent A-V valves (mitral/tricuspid), it also can be due to ventricular septal defect.
68 What characteristics of a systolic murmur help differentiate ejection from regurgitation?
 The relationship of the murmur to S2. Regurgitant systolic murmurs typically extend into S2 (and sometimes even beyond it), whereas ejection murmurs always end before it. This may be difficult to detect, since S2 is often soft (and even absent in severe semilunar stenosis).
The relationship of the murmur to S2. Regurgitant systolic murmurs typically extend into S2 (and sometimes even beyond it), whereas ejection murmurs always end before it. This may be difficult to detect, since S2 is often soft (and even absent in severe semilunar stenosis).
 The change of the murmur after a longer diastole. This is especially evident after a premature beat (see question 26), with ejection murmurs of semilunar stenosis becoming louder, and regurgitant murmurs of atrioventricular insufficiency remaining constant.
The change of the murmur after a longer diastole. This is especially evident after a premature beat (see question 26), with ejection murmurs of semilunar stenosis becoming louder, and regurgitant murmurs of atrioventricular insufficiency remaining constant.
 The response of the murmur to bedside maneuvers (previously discussed)
The response of the murmur to bedside maneuvers (previously discussed)
 The musical quality of the murmur. This is only present in situations of regurgitation.
The musical quality of the murmur. This is only present in situations of regurgitation.
(1) Systolic Ejection Murmurs



74 In addition to pitch, are there other differences between ejection and regurgitant murmurs?






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


