Chapter 3 The Skin
Basic Terminology and Diagnostic Techniques
1 How many skin diseases exist? What are the two main categories of skin lesions?
There are more than 1400 skin diseases. Yet, only 30 are important, common, and worth knowing. The first step toward their recognition is the separation of primary from secondary lesions (Table 3-1).
 Primary lesions result only from disease and have not been changed by additional events (such as trauma, scratching, or medical treatment; see Table 3-1). To better identify primary lesions, pay attention to their colors, shape, arrangement, and distribution.
Primary lesions result only from disease and have not been changed by additional events (such as trauma, scratching, or medical treatment; see Table 3-1). To better identify primary lesions, pay attention to their colors, shape, arrangement, and distribution.

Table 3-1 Dermatologic Lesions
| skin lesions | ||
|---|---|---|
| Primary | Secondary | Special |
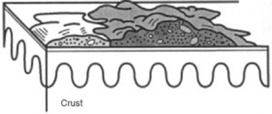
| Solid (Nonpalpable) | Crusts | Purpurae |
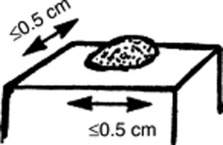
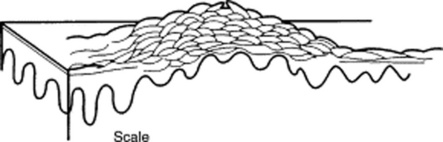
| • Macules (≤0.5 cm) | Scales | Petechiae |
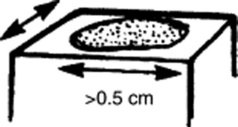
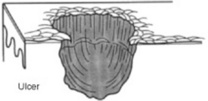
| • Patches (>0.5 cm) | Ulcers | Ecchymoses |
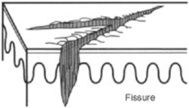
| Fissures | Teleangiectasias | |
| Solid (Palpable) | Excorations | Comedones |
| • Papules (≤0.5 cm) | Scars | Burrows |
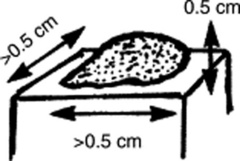
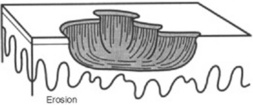
| • Plaques (>0.5 cm) | Erosions | Target lesions |
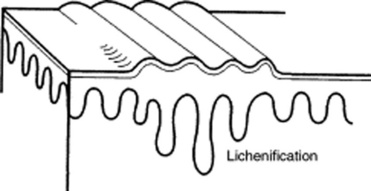
| • Nodules (deeper plaques) | Lichenification | |
| • Wheals (pruritic plaques) | Atrophy | |
| • Tumors (larger nodules) | Scars | |
| Sinuses | ||
| Fluid-Lesions | ||
| • Vesicles (fluid-filled papules) | ||
| • Pustules (pus-filled papules) | ||
| • Bullae (fluid-filled plaques) | ||
| • Cysts (fluid-filled nodules) | ||
2 What are the major primary lesions?
 Macules: Flat, nonpalpable, circumscribed areas of discoloration ≤0.5 cm in diameter. Typical macules are the familiar freckles.
Macules: Flat, nonpalpable, circumscribed areas of discoloration ≤0.5 cm in diameter. Typical macules are the familiar freckles.




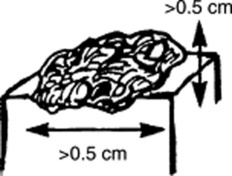
 Tumors: Nodules that are either >2 cm in diameter or poorly demarcated. Usually neoplastic.
Tumors: Nodules that are either >2 cm in diameter or poorly demarcated. Usually neoplastic.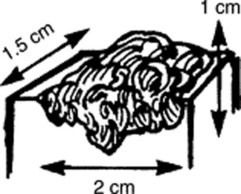







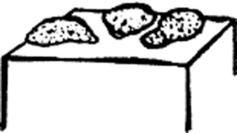
 Pustules: Pus-filled papules. Typically seen in patients with impetigo or acne.
Pustules: Pus-filled papules. Typically seen in patients with impetigo or acne.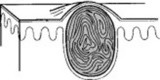









3 What are the major secondary lesions?
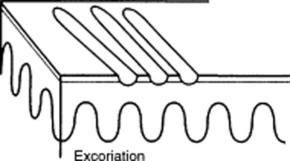
 Excoriations: Linear erosions produced by scratching. Often raised, scratch marks may also present as crust on top of a primary lesion that has been partially scratched off. They are almost exclusively confined to the eczematous diseases.
Excoriations: Linear erosions produced by scratching. Often raised, scratch marks may also present as crust on top of a primary lesion that has been partially scratched off. They are almost exclusively confined to the eczematous diseases.







 Sinuses: Connective channels between the surface of the skin and deeper components.
Sinuses: Connective channels between the surface of the skin and deeper components.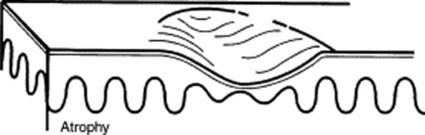
4 Are there other ways to classify skin lesions?
Many ways. One divides lesions into four groups based on the relationship with the surrounding skin:







6 What is the configuration of a skin lesion?
It is the outline of the lesion as observed from above. The most common configurations are:




9 And so, what are the required components of a dermatologic diagnosis?
 Morphology: Color, shape, dimensions (width and height, if necessary), elevation/depression, and palpable features (smoothness, induration, tenderness, scaling, and crusting)
Morphology: Color, shape, dimensions (width and height, if necessary), elevation/depression, and palpable features (smoothness, induration, tenderness, scaling, and crusting)
 Distribution (body location): Generalized versus localized
Distribution (body location): Generalized versus localized
 Distribution (arrangement to one another): Clustered, confluent, dermatomal
Distribution (arrangement to one another): Clustered, confluent, dermatomal




14 How should fingernails and toenails be assessed?
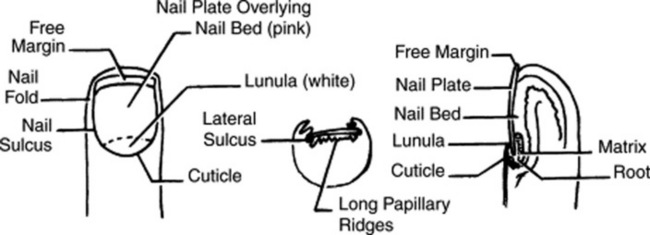
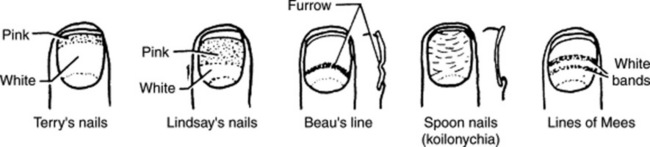
If covered by polish, clean them first with a solvent like acetone. Then pay attention to color and shape but also to anatomic details (Fig. 3-25):
 Lunula: The white half-moon at the proximal edge of the nail bed
Lunula: The white half-moon at the proximal edge of the nail bed
 Cuticle: The thin skin adherent to the nail at its proximal portion
Cuticle: The thin skin adherent to the nail at its proximal portion
 Perionychium: The epidermis forming the ungual wall at the sides and back of the nail
Perionychium: The epidermis forming the ungual wall at the sides and back of the nail
15 What systemic conditions are associated with changes in nail shape or growth?
 Clubbing: Inflammatory bowel disease, pulmonary malignancy, asbestosis, chronic bronchitis, chronic obstructive pulmonary disease, cirrhosis, congenital heart disease, endocarditis, atrioventricular malformation and fistulas (see also question 19)
Clubbing: Inflammatory bowel disease, pulmonary malignancy, asbestosis, chronic bronchitis, chronic obstructive pulmonary disease, cirrhosis, congenital heart disease, endocarditis, atrioventricular malformation and fistulas (see also question 19)
 Koilonychia (spoon nails) (Fig. 3-26): Iron deficiency anemia, hemochromatosis, Raynaud’s disease, systemic lupus disease, trauma, nail-patella syndrome
Koilonychia (spoon nails) (Fig. 3-26): Iron deficiency anemia, hemochromatosis, Raynaud’s disease, systemic lupus disease, trauma, nail-patella syndrome

 Pitting: Psoriasis, Reiter’s syndrome, incontinentia pigmenti, alopecia areata
Pitting: Psoriasis, Reiter’s syndrome, incontinentia pigmenti, alopecia areata
 Beau’s lines (see Fig. 3-26): Any severe systemic illness that disrupts nail growth, Raynaud’s disease, pemphigus, trauma
Beau’s lines (see Fig. 3-26): Any severe systemic illness that disrupts nail growth, Raynaud’s disease, pemphigus, trauma

16 What systemic conditions are associated with changes in nail color?
 Terry’s nails (see Fig. 3-26): Hepatic failure, cirrhosis, diabetes, congestive heart failure, hyperthyroidism, malnutrition
Terry’s nails (see Fig. 3-26): Hepatic failure, cirrhosis, diabetes, congestive heart failure, hyperthyroidism, malnutrition
 Azure lunula: Wilson’s disease, silver poisoning, quinacrine
Azure lunula: Wilson’s disease, silver poisoning, quinacrine
 Lindsay’s nails (half-and-half nails) (see Fig. 3-26): Specific for renal failure
Lindsay’s nails (half-and-half nails) (see Fig. 3-26): Specific for renal failure
 Muehrcke’s lines: Specific for hypoalbuminemia
Muehrcke’s lines: Specific for hypoalbuminemia
 Lines of Mees’ (see Fig. 3-26): Arsenic poisoning, Hodgkin’s disease, congestive heart failure, leprosy, malaria, chemotherapy, carbon monoxide poisoning, other systemic insults
Lines of Mees’ (see Fig. 3-26): Arsenic poisoning, Hodgkin’s disease, congestive heart failure, leprosy, malaria, chemotherapy, carbon monoxide poisoning, other systemic insults

 Longitudinal striations: Alopecia areata, vitiligo, atopic dermatitis, psoriasis
Longitudinal striations: Alopecia areata, vitiligo, atopic dermatitis, psoriasis

 Telangiectasia: Rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, scleroderma
Telangiectasia: Rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, scleroderma





Nails
19 What is clubbing?
A condition that can be (1) idiopathic; (2) congenital (dominant trait); or (3) a clue to serious underlying pathology, including cardiovascular, hepatobiliary, mediastinal, endocrine, gastrointestinal, neoplastic, infectious, and, especially, pulmonary (see Chapter 13, questions 101–116).
22 What are the nail findings of psoriasis?
 Pitting (previously discussed)
Pitting (previously discussed)

 Beau’s lines in the proximal nail matrix (see later)
Beau’s lines in the proximal nail matrix (see later)
 Leukonychia: Areas of white nail plate; due to parakeratotic foci in the mid-matrix
Leukonychia: Areas of white nail plate; due to parakeratotic foci in the mid-matrix
 Subungual hyperkeratosis: Excessive proliferation of the nail bed that can lead to onycholysis
Subungual hyperkeratosis: Excessive proliferation of the nail bed that can lead to onycholysis

 Nail plate crumbling: Weakened nail plate, bed, and matrix from diseased underlying structures
Nail plate crumbling: Weakened nail plate, bed, and matrix from diseased underlying structures

 Dilated tortuous capillaries in the dermal papillae
Dilated tortuous capillaries in the dermal papillae
 Spotted lunula: Distal matrix involvement characterized by erythema of the lunula
Spotted lunula: Distal matrix involvement characterized by erythema of the lunula
26 What is longitudinal ridging (Reedy nails)?
A normal variant of patients older than 50, but one that also can occur in younger subjects. It may even represent a brittle nail variation. Ridges typically extend from the proximal nail fold to the distal plate, with some being very prominent, especially in older women. They are usually multiple, but at times may be single—like in patients with lichen planus (see questions 38 and 210–216).
38 What is lichen planus of the nail?
A condition present in 10% of patients with lichen planus. The most common finding is thinning of the nail plate, leading to longitudinal grooving and ridging (see also question 26). Hyperpigmentation, subungual hyperkeratosis, onycholysis, and longitudinal melanonychia can also be present.
41 What are azure half-moons in nail beds?
The nails of Wilson’s disease (hepatolenticular degeneration). Lunulae are not white, but bluish.
48 What is paronychia?
An acute or chronic inflammation of the perionychium, with redness, swelling, and tenderness.
Fluid-Filled Lesions: PUS (Pustules)—Table 3-2
Acne
54 What does acne look like?
Table 3-2 Fluid-Filled lesions
| Fluid-Filled Lesions | ||
|---|---|---|
| Pus-Filled | Clear Fluid | |
| Pustular | Vesiculo-Bullous | Bullous |
| Acne vulgaris | H. simplex | Pemphygus vulgaris |
| Acne rosacea | H. zoster/varicella | Pemphygoid |
| Steroid acne | Dermatophytoses | Drug reactions |
| • Erythema multiforme | ||
| • Stevens-Johnson | ||
| • TEN | ||
| Folliculitis (bacterial/fungal) | Insect bites | Poison ivy/contact dermatitis |
| Intertriginous candidiasis | Dermatitis herpetiformis | Bullous impetigo |
| Porphyria cutanea tarda | ||
| Lupus erythematosus | ||
Fluid-Filled Lesions: Clear Fluid (Vesiculobullous Diseases)
62 What is the typical clinical course of herpes simplex?


63 What are the other clinical presentations of herpes simplex?



66 Who develops varicella?
Mostly children younger than 10 years. Only 5% of cases occur in subjects older than 15.
73 What are the other presentations of herpes zoster?



79 Are there any other causes of PV?
A form of PV (but also BP, see question 80) can be drug induced, resulting from penicillamine, captopril, thiol-containing compounds, and rifampin. Emotional stress can also trigger it. Finally, PV may occur in other autoimmune diseases, including myasthenia gravis and thymoma.
82 What is Asboe-Hansen sign?
Another sign of PV; lateral pressure on the edge of a blister may spread it into unaffected skin.
84 What is erythema multiforme (EM)?
A relatively benign process characterized by target or targetoid lesions, with or without blisters, in a symmetric and acral distribution. In fact, the rash favors palms and soles, dorsum of hands, face, and extensor surfaces of extremities (Fig. 3-27). It is often associated with oral lesions, but rarely involves more than one mucosal surface. Although it can be caused by drugs, it is most commonly a sequela of herpes virus infection. It has low morbidity, no mortality, but frequent recurrences. It may be associated with epidermal detachment, yet denudation always involves <10% of BSA.

85 What is Stevens-Johnson syndrome (SJS)?
A potential dermatologic emergency. First described in 1922 by the American pediatricians Albert Stevens and Frank Johnson, SJS is characterized by widespread purpuric macules and targetoid lesions, usually more common on face and torso, and with concomitant mucosal involvement of more than one site (usually the eyes, mouth, and genitalia; Fig. 3-28). Lesions may undergo full-thickness epidermal necrosis, although this is limited by definition to <10% of cutaneous surface. Hence, mortality is much less than in TEN (only 5%).

86 What is toxic epidermal necrolysis (TEN)?
Also known as Lyell’s syndrome, this is a true dermatologic emergency characterized by widespread skin and mucosal denudation. Skin lesions are erythematous and target-like macules associated with full-thickness epidermal necrosis and detachment of >30% BSA (Fig. 3-29). It is fatal in 50% of the cases, usually because of sepsis and respiratory distress. Mortality is related to BSA involvement: 11% for BSA (which is actually more of a SJS-TEN transitional form), and 35% for BSA >30%.
91 What are the sequelae of SJS/TEN?




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


