Chapter 13 The Hepatobiliary System







2 What are the most common morphologic signs of liver injury?
 Vacuolar change: Affected hepatocytes are enlarged and have a swollen, clear cytoplasm. This hydropic swelling of hepatocytes is a common response to injury. It is reversible, but if intensified or prolonged, it may lead to liver cell necrosis.
Vacuolar change: Affected hepatocytes are enlarged and have a swollen, clear cytoplasm. This hydropic swelling of hepatocytes is a common response to injury. It is reversible, but if intensified or prolonged, it may lead to liver cell necrosis.

3 How does the liver respond to injury?
 Inflammation: Injured liver cells must be removed. To this end, the body sends in inflammatory cells that react with injured hepatocytes. For example, hepatocytes infected with hepatitis virus elicit a T-cell response. These lymphocytes enter the liver and kill the infected hepatocytes, which are thereafter removed by macrophages.
Inflammation: Injured liver cells must be removed. To this end, the body sends in inflammatory cells that react with injured hepatocytes. For example, hepatocytes infected with hepatitis virus elicit a T-cell response. These lymphocytes enter the liver and kill the infected hepatocytes, which are thereafter removed by macrophages.





5 Discuss the necroinflammatory indices, that is, the laboratory tests used to monitor the integrity of liver cells
6 Which tests are used to measure hepatic secretory function?
 Albumin: Normally, the blood contains 3.5 to 5.0 g/dL (35–50 g/L) albumin, the most copious plasma protein. Chronic liver injury will reduce blood concentration of albumin to less than 3 g/dL.
Albumin: Normally, the blood contains 3.5 to 5.0 g/dL (35–50 g/L) albumin, the most copious plasma protein. Chronic liver injury will reduce blood concentration of albumin to less than 3 g/dL.
7 Discuss the tests used to measure biliary excretion
 Bilirubin: Bilirubin that has been conjugated in the liver to be excreted into the intestine may accumulate in the blood of patients who have bile duct obstruction.
Bilirubin: Bilirubin that has been conjugated in the liver to be excreted into the intestine may accumulate in the blood of patients who have bile duct obstruction.

JAUNDICE













12 Why is it important to fractionate bilirubin in the serum?
According to laboratory analysis, hyperbilirubinemia can be classified as follows:



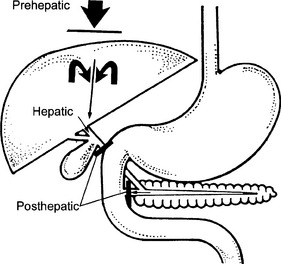
13 Describe the main forms of jaundice
Three pathogenetic forms of jaundice are recognized clinically (Fig. 13-1):



15 What are the main causes of predominantly unconjugated hyperbilirubinemia?




 Resorption of bilirubin from internal hemorrhages (e.g., massive hematoma and intestinal hemorrhage)
Resorption of bilirubin from internal hemorrhages (e.g., massive hematoma and intestinal hemorrhage)
17 What is the cause of jaundice in genetic diseases characterized by unconjugated hyperbilirubinemia?
21 List common causes of mixed hyperbilirubinemia
Mixed hyperbilirubinemia is a sign of “hepatic jaundice” and it is typically seen in:


















HEPATIC FAILURE







28 What are the clinical features of chronic liver failure?
 Cirrhosis with changes in the shape and size of the liver best visible by computed axial tomography (CAT) scan
Cirrhosis with changes in the shape and size of the liver best visible by computed axial tomography (CAT) scan









A mnemonic for the consequences of liver failure is jaundice:
30 What are the main forms of portal hypertension?
Three forms of portal hypertension are recognized depending on the site of obstruction:
 Presinusoidal: This is due to obstruction of the portal vein or its major intrahepatic branches. Typically, this occurs in portal vein thrombosis or fibrosis of bile ducts (e.g., schistosomiasis) that affects the adjacent blood vessels in the liver.
Presinusoidal: This is due to obstruction of the portal vein or its major intrahepatic branches. Typically, this occurs in portal vein thrombosis or fibrosis of bile ducts (e.g., schistosomiasis) that affects the adjacent blood vessels in the liver.




32 Where do portal–systemic anastomoses develop in portal hypertension?
Shunting of portal venous blood into the systemic circulation occurs at three anatomic sites:
 Esophageal and gastric veins: Esophageal varices are the most common site of massive bleeding in patients with chronic liver disease. Exsanguination from ruptured esophageal varices is a major cause of death in cirrhosis.
Esophageal and gastric veins: Esophageal varices are the most common site of massive bleeding in patients with chronic liver disease. Exsanguination from ruptured esophageal varices is a major cause of death in cirrhosis.

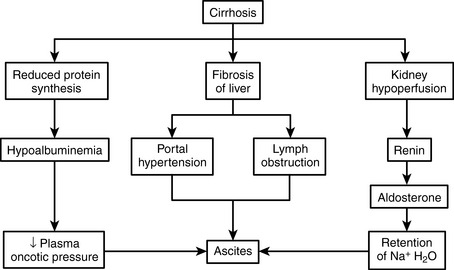
33 Discuss the pathogenesis of ascites in cirrhosis
The pathogenesis of ascites is not fully understood, but it appears to be a consequence of several disturbances found in patients with cirrhosis (Fig. 13-2):
 Portal hypertension: Increased hydrostatic pressure leads to transudation of fluid into the abdominal cavity.
Portal hypertension: Increased hydrostatic pressure leads to transudation of fluid into the abdominal cavity.


35 Explain the pathogenesis of palmar erythema, gynecomastia, and spider angiomas in patients with cirrhosis
36 Explain the bleeding tendency commonly found in patients with cirrhosis
 Reduced concentration of coagulation factors in blood: One should remember that most of the plasma coagulation factors are produced in the liver. Loss of synthetic activity of hepatocytes results in hypofibrinogenemia and reduced levels of all other coagulation proteins. Typically PT and activated partial thromboplastin time are prolonged.
Reduced concentration of coagulation factors in blood: One should remember that most of the plasma coagulation factors are produced in the liver. Loss of synthetic activity of hepatocytes results in hypofibrinogenemia and reduced levels of all other coagulation proteins. Typically PT and activated partial thromboplastin time are prolonged.

Massive uncontrollable bleeding is a major cause of death in patients with cirrhosis.
INFECTIOUS DISEASES
37 Discuss the most important infectious diseases affecting the liver
 Viral diseases: These diseases are most often caused by hepatotropic viruses (e.g., hepatitis virus A, B, and C) but also may occur in the course of other viral infections (e.g., herpes simplex and cytomegalovirus [CMV]).
Viral diseases: These diseases are most often caused by hepatotropic viruses (e.g., hepatitis virus A, B, and C) but also may occur in the course of other viral infections (e.g., herpes simplex and cytomegalovirus [CMV]).

39 Do all hepatitis viruses belong to the same group, and do they share the same structural properties?
40 Is liver biopsy useful for diagnosing acute viral hepatitis?
 The changes caused by various hepatotropic viruses are nonspecific. Microscopically, acute HAV cannot be distinguished from HBV or other hepatitides of this type.
The changes caused by various hepatotropic viruses are nonspecific. Microscopically, acute HAV cannot be distinguished from HBV or other hepatitides of this type.

< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


