Chapter 12 The Gastrointestinal System
1 What is the basic structure of the gastrointestinal (GI) system?
The entire GI tract has a relatively uniform structure and consists of four layers:




2 What are the main diseases of the GI system?


 Functional disorders affecting the digestion, absorption of nutrients, or motility of the intestines
Functional disorders affecting the digestion, absorption of nutrients, or motility of the intestines

3 Discuss the possible consequences of abnormal development of the GI system
 Atresia (absence of lumen; The normal GI system is a tube that develops from cords of embryonic cells. The cells forming the central part of these cords undergo apoptosis, and a lumen is thus formed. If the centrally located cells do not undergo apoptosis, the lumen never forms, and the affected part of the GI system will be atretic, i.e., unpassable.)
Atresia (absence of lumen; The normal GI system is a tube that develops from cords of embryonic cells. The cells forming the central part of these cords undergo apoptosis, and a lumen is thus formed. If the centrally located cells do not undergo apoptosis, the lumen never forms, and the affected part of the GI system will be atretic, i.e., unpassable.)


ESOPHAGUS
4 What are the main clinical symptoms and signs of esophageal disease?
 Dysphagia: Difficulty in swallowing. It may be caused by anatomic lesions (e.g., stricture, webs, and rings), cancer, or functional disorders (e.g., achalasia and paralysis).
Dysphagia: Difficulty in swallowing. It may be caused by anatomic lesions (e.g., stricture, webs, and rings), cancer, or functional disorders (e.g., achalasia and paralysis).


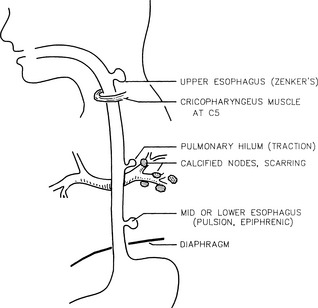
6 What are esophageal diverticula?
Diverticula are outpouchings of the wall of the esophagus. These outpouchings are classified on the basis of the following (Fig. 12.1):










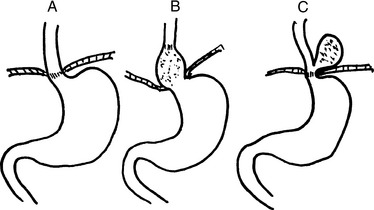
9 What is hiatal hernia?
Hiatal hernia is a protrusion of the stomach above the diaphragm through a widened diaphragmatic hiatus. Hiatal hernias are quite common. Two forms are recognized (Fig. 12-2):
 Sliding hernia (90%): The gastroesophageal junction is pulled into the thorax and is found above the diaphragm. In most instances, it is asymptomatic and diagnosed accidentally during the workup of the patient for some other disease. It may be associated with GERD, heartburn, and dysphagia.
Sliding hernia (90%): The gastroesophageal junction is pulled into the thorax and is found above the diaphragm. In most instances, it is asymptomatic and diagnosed accidentally during the workup of the patient for some other disease. It may be associated with GERD, heartburn, and dysphagia.
12 Discuss the causes of GERD
 Temporary increase in intraabdominal pressure (e.g., after overeating or drinking carbonated drinks)
Temporary increase in intraabdominal pressure (e.g., after overeating or drinking carbonated drinks)















15 What are the causes of infectious esophagitis?
 Fungal infection: Candida albicans and other fungi may grow on the surface of the squamous epithelium, such as in the mouth or the vagina.
Fungal infection: Candida albicans and other fungi may grow on the surface of the squamous epithelium, such as in the mouth or the vagina.

16 What are the most common forms of chemical esophagitis?
 Hydrochloric acid: HCl regurgitated from the stomach is the most common cause of esophagitis in GERD.
Hydrochloric acid: HCl regurgitated from the stomach is the most common cause of esophagitis in GERD.















23 List the risk factors for esophageal cancer
 Environmental factors that could account for the higher incidence of esophageal cancer in areas of Asia and Africa (e.g., soil, tea, or food) have not been identified.
Environmental factors that could account for the higher incidence of esophageal cancer in areas of Asia and Africa (e.g., soil, tea, or food) have not been identified.








STOMACH






30 Discuss why gastric erosions develop in acute gastritis




33 Is it possible to distinguish type A and type B chronic gastritis in biopsy material examined microscopically?



34 Is it possible to clinically distinguish type A from type B chronic gastritis?
As stated previously, the histologic diagnosis of type B chronic gastritis depends primarily on finding H. pylori in the gastric biopsies. Because the gastroscopic findings are similar in both forms of gastritis and H. pylori cannot always be found in advanced stages of the disease, other tests (e.g., urea breath test or antibody test for H. pylori) must be performed. The most important aspects of type A and type B gastritis useful for distinguishing one form of gastritis from the other are listed in Table 12-1.
TABLE 12-1 Major Aspects of Type A And Type B Gastritis
| Feature | Type A Gastritis* | Type B Gastritis |
|---|---|---|
| Distribution of lesions | Fundus, diffuse | Pyloric antrum, focal |
| Gastric secretion | Reduced | Normal, +, or − |
| Antibodies to parietal cells | Yes | No |
| Other autoimmune diseases | Yes | No |
| Vitamin B12 (in serum) | Low | Normal |
| Pernicious anemia | + | − |
| Gastrin (in serum) | Increased | Normal |
| Antibodies to Helicobacter pylori | − | + |
| Incidence | Less common | More common |
| Age dependence | Yes | Yes |
| Cancer risk | Increased | Increased |
* Type A gastritis is associated with four As: autoimmune disease, antibodies to pyloric cells, anemia (pernicious), and achlorhydria (reduced hydrochloric acid secretion).
37 Which factors play a role in the development of peptic ulcers?
Peptic ulcer is a multifactorial disease, and several factors contribute to its pathogenesis:
 Infection: H. pylori is found in 90% of duodenal and 65% of gastric ulcer patients. H. pylori secretes urease, protease, and phospholipases that may cause mucosal injury and may serve as “barrier breakers,” facilitating the chemical injury of mucosal cells. Eradication of H. pylori infections contributes to the healing of peptic ulcers.
Infection: H. pylori is found in 90% of duodenal and 65% of gastric ulcer patients. H. pylori secretes urease, protease, and phospholipases that may cause mucosal injury and may serve as “barrier breakers,” facilitating the chemical injury of mucosal cells. Eradication of H. pylori infections contributes to the healing of peptic ulcers.









Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


