Chapter 22 The Central Nervous System








REACTION OF THE CENTRAL NERVOUS SYSTEM TO INJURY
2 List the most important pathologic reactions of neurons
 Acute injury: This is most commonly caused by hypoxia/ischemia but also under the influence of toxic or infectious agents that can kill neurons. Affected neurons have pyknotic nuclei and an acidophilic cytoplasm, which stains intensely red with eosin (“red is dead”) in standard hematoxylin and eosin (H&E) slides.
Acute injury: This is most commonly caused by hypoxia/ischemia but also under the influence of toxic or infectious agents that can kill neurons. Affected neurons have pyknotic nuclei and an acidophilic cytoplasm, which stains intensely red with eosin (“red is dead”) in standard hematoxylin and eosin (H&E) slides.



5 What are the common forms of cerebral edema?
Three forms of cerebral edema are recognized: vasogenic, cytotoxic, and interstitial.
 Vasogenic edema: It is characterized by the accumulation of fluid in between the neurons and glial cells and most prominently in the Virchow–Robin spaces around the blood vessels. It develops as a consequence of blood–brain barrier dysfunction. Fluid escapes from the vascular space into the interstitial space of the parenchyma across the cytoplasm of vascular endothelial cells or between these cells through the disrupted tight junctions. It may be localized (e.g., around a tumor or an abscess) or generalized (e.g., in encephalitis or following head trauma).
Vasogenic edema: It is characterized by the accumulation of fluid in between the neurons and glial cells and most prominently in the Virchow–Robin spaces around the blood vessels. It develops as a consequence of blood–brain barrier dysfunction. Fluid escapes from the vascular space into the interstitial space of the parenchyma across the cytoplasm of vascular endothelial cells or between these cells through the disrupted tight junctions. It may be localized (e.g., around a tumor or an abscess) or generalized (e.g., in encephalitis or following head trauma).

6 Describe the gross appearance of the brain with generalized vasogenic edema
Typical features seen at autopsy include:





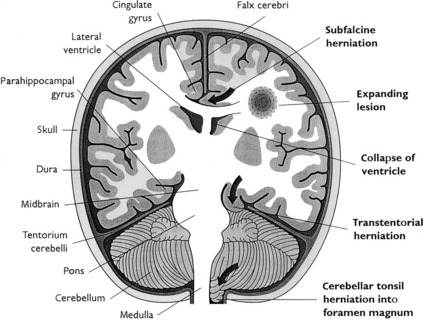
7 Describe various forms of intracranial cerebral or cerebellar herniations
Herniations (Fig. 22-1) occur as a result of increased intracranial volume. Most often, they accompany space-occupying lesions, such as tumors, hematomas, or abscesses, but they may also be caused by trauma. The displacement of parts of the brain is morphologically most evident at three herniation sites:
 Cingulate herniation (subfalcine herniation): It results from a unilateral hemispheric mass lesion (e.g., abscess, hematoma, and tumor) that expands the volume of one hemisphere, dislocates the midline structures (midline shift), and forces the ipsilateral cingulate gyrus to be compressed (“herniate”) underneath the falx cerebri. Focal necrosis and hemorrhage may develop in the herniated tissue together with distant reduction of blood flow (i.e., compression of the anterior cerebral artery).
Cingulate herniation (subfalcine herniation): It results from a unilateral hemispheric mass lesion (e.g., abscess, hematoma, and tumor) that expands the volume of one hemisphere, dislocates the midline structures (midline shift), and forces the ipsilateral cingulate gyrus to be compressed (“herniate”) underneath the falx cerebri. Focal necrosis and hemorrhage may develop in the herniated tissue together with distant reduction of blood flow (i.e., compression of the anterior cerebral artery).

DEVELOPMENTAL DISORDERS
8 Define dysraphic malformations and list the most common forms of this malformation
 Cranial dysraphism: It is associated with incomplete formation of the skull and occurs most often as anencephaly or encephalocele. This severe cerebral malformation is usually incompatible with life.
Cranial dysraphism: It is associated with incomplete formation of the skull and occurs most often as anencephaly or encephalocele. This severe cerebral malformation is usually incompatible with life.
9 List the most frequent causes of congenital CNS malformations
The cause of most congenital CNS malformations is unknown. The following are among the known causes:
 Fetal intrauterine infections such as those causing the TORCH complex, which includes toxoplasmosis, rubella, cytomegalovirus (CMV), herpes virus, and others such as syphilis, listeriosis, leptospirosis, and viral infection with varicella-zoster virus, Epstein–Barr and so on, etc.; human immunodeficiency virus 1 (HIV-1) infection during fetal life may also cause CNS lesions.
Fetal intrauterine infections such as those causing the TORCH complex, which includes toxoplasmosis, rubella, cytomegalovirus (CMV), herpes virus, and others such as syphilis, listeriosis, leptospirosis, and viral infection with varicella-zoster virus, Epstein–Barr and so on, etc.; human immunodeficiency virus 1 (HIV-1) infection during fetal life may also cause CNS lesions.


PHYSICAL INJURY
10 What are the main forms of spinal cord or brain injury caused by physical forces?
Skull fractures are often accompanied by parenchymal injuries, which include:
 Contusions (“bruising”): This type of injury results from rapid deceleration or acceleration of the skull and the brain. Typically it involves a coup lesion at the site of the impact of force or a contrecoup contusion, diametrically opposite to it.
Contusions (“bruising”): This type of injury results from rapid deceleration or acceleration of the skull and the brain. Typically it involves a coup lesion at the site of the impact of force or a contrecoup contusion, diametrically opposite to it.



11 Describe the most common spinal cord injuries
 Hyperextension injury: It typically occurs in the cervical spine and is caused by sudden posterior displacement of the head that causes rupture of the anterior spinal ligament. The so-called posterior angulation of the cervical vertebrae is accompanied by contusion of the posterior segment of the cervical spinal cord.
Hyperextension injury: It typically occurs in the cervical spine and is caused by sudden posterior displacement of the head that causes rupture of the anterior spinal ligament. The so-called posterior angulation of the cervical vertebrae is accompanied by contusion of the posterior segment of the cervical spinal cord.








VASCULAR DISORDERS
15 List the most common aneurysms found in the CNS
 Berry aneurysms: These small saccular aneurysms are typically found in and around the circle of Willis at the base of the brain. They develop at the site of arterial branching corresponding to the congenital weakest part of the vessels. The rupture of these aneurysms leads to a usually fatal subarachnoid and/or intraparenchymal/intraventricular hemorrhage.
Berry aneurysms: These small saccular aneurysms are typically found in and around the circle of Willis at the base of the brain. They develop at the site of arterial branching corresponding to the congenital weakest part of the vessels. The rupture of these aneurysms leads to a usually fatal subarachnoid and/or intraparenchymal/intraventricular hemorrhage.

17 List the most important causes of nontraumatic intracerebral hemorrhage (i.e., hemorrhagic strokes)
 Hypertension: Chronic, severe (usually uncontrolled), systemic hypertension is the most common cause of hemorrhagic stroke. Hypertension accelerates arteriosclerosis of the larger arteries and also causes lipohyalinosis of the smaller branches promoting the development of rupture-prone Charcot–Bouchard aneurysms. Hypertensive hemorrhages occur most often within the basal ganglia and less commonly in the cerebellum or the medulla oblongata.
Hypertension: Chronic, severe (usually uncontrolled), systemic hypertension is the most common cause of hemorrhagic stroke. Hypertension accelerates arteriosclerosis of the larger arteries and also causes lipohyalinosis of the smaller branches promoting the development of rupture-prone Charcot–Bouchard aneurysms. Hypertensive hemorrhages occur most often within the basal ganglia and less commonly in the cerebellum or the medulla oblongata.




19 What are the pathologic consequences of global cerebral ischemia?
Generalized reduction of available oxygen that affects the whole CNS may cause:






INFECTIONS
21 What are the most common routes of entry of infectious agents into the intracranial space?
 Vascular spread: Most infectious agents reach the brain and the meninges through the arterial bloodstream. Venous blood may serve as a carrier of infectious agents from the infected periocular and perinasal tissues.
Vascular spread: Most infectious agents reach the brain and the meninges through the arterial bloodstream. Venous blood may serve as a carrier of infectious agents from the infected periocular and perinasal tissues.


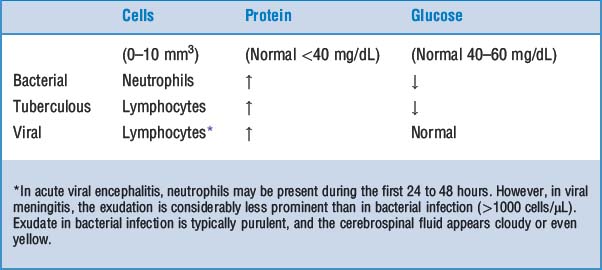
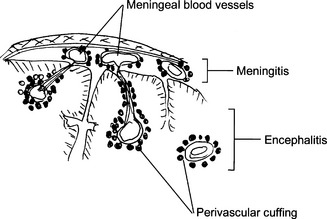
22 What are the most important infectious diseases of the CNS ?
 Meningitis: Infection may be limited to the subarachnoid space (leptomeningitis) or may spread into the brain (meningoencephalitis). Such infection may be classified as acute or chronic. According to the appearance of the cerebrospinal fluid one can classify meningitis as purulent (bacterial) or serous (viral).
Meningitis: Infection may be limited to the subarachnoid space (leptomeningitis) or may spread into the brain (meningoencephalitis). Such infection may be classified as acute or chronic. According to the appearance of the cerebrospinal fluid one can classify meningitis as purulent (bacterial) or serous (viral).








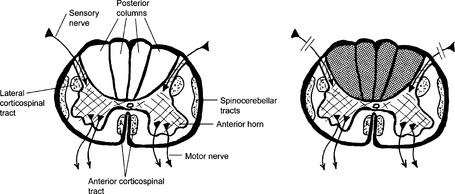
28 What is tabes dorsalis?
Tabes dorsalis (Fig. 22-2) is a manifestation of tertiary syphilis involving the lumbar spinal cord. Syphilitic meningitis leads to fibrosis, compressing the posterior nerve roots. In normal circumstances, these afferent nerves, originating from the spinal ganglia, form the posterior columns in the spinal cord, and transmit proprioceptive and sensory impulses. Wallerian degeneration that results from the injury of axons entering the spinal cord results in posterior columns. Clinically, these patients experience loss of vibration and proprioception, which affects their gait. Joint degeneration resulting in deformities (Charcot joints) is commonly found.














31 List key facts about the pathogenesis and pathology of cerebral abscesses
 Localized suppuration of the brain is caused by pyogenic bacteria (Streptococcus pneumoniae or Staphylococcus aureus) presenting clinically as a destructive, space-occupying lesion.
Localized suppuration of the brain is caused by pyogenic bacteria (Streptococcus pneumoniae or Staphylococcus aureus) presenting clinically as a destructive, space-occupying lesion.


32 List key facts about the clinical presentation of cerebral abscess
 General signs and symptoms of infection and increased intracranial pressure (e.g., somnolence and papilledema). Progressive intracranial hypertension may cause hemiplegia, seizures, and even coma.
General signs and symptoms of infection and increased intracranial pressure (e.g., somnolence and papilledema). Progressive intracranial hypertension may cause hemiplegia, seizures, and even coma.


Key Points: Infections and Immunologic Diseases










35 List viral infections associated with cellular inclusions visible by light microscopy
 There is CMV enlargement of cells, which contain typical bluish “owl-eyed” intranuclear inclusions. The cytoplasm also contains virions and appears bluish.
There is CMV enlargement of cells, which contain typical bluish “owl-eyed” intranuclear inclusions. The cytoplasm also contains virions and appears bluish.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


