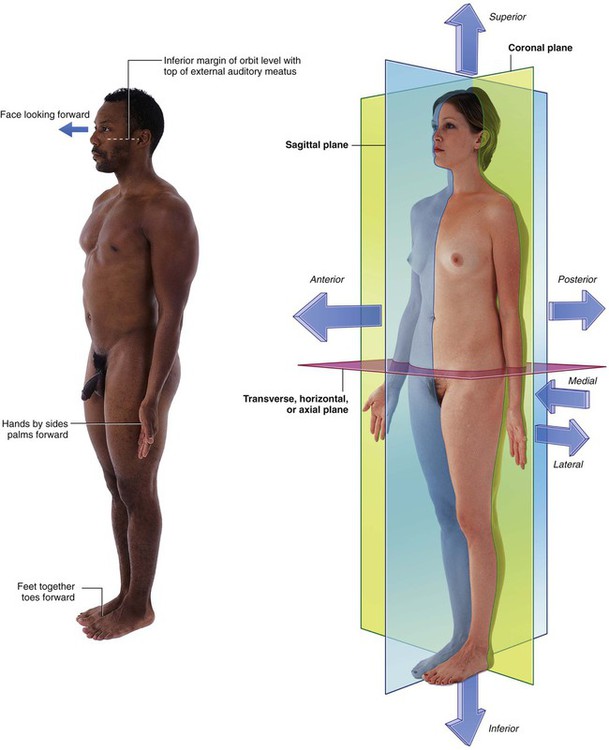
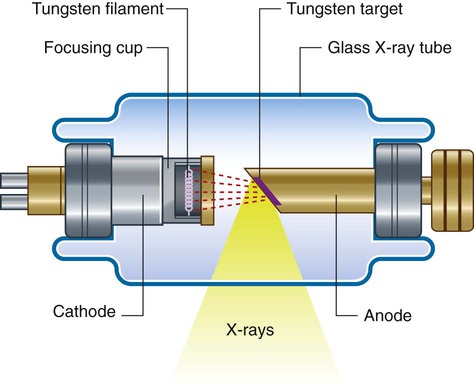
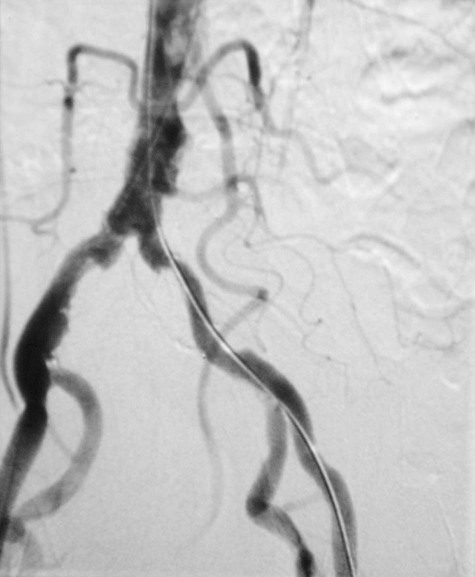
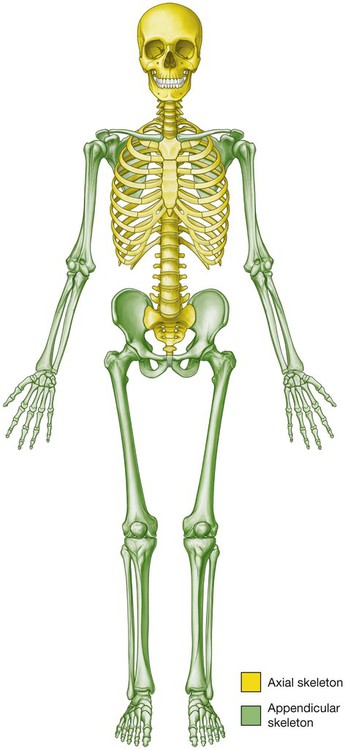
Anatomy can be studied following either a regional or a systemic approach. The anatomical position is the standard reference position of the body used to describe the location of structures (Fig. 1.1). The body is in the anatomical position when standing upright with feet together, hands by the side and face looking forward. The mouth is closed and the facial expression is neutral. The rim of bone under the eyes is in the same horizontal plane as the top of the opening to the ear, and the eyes are open and focused on something in the distance. The palms of the hands face forward with the fingers straight and together and with the pad of the thumb turned 90° to the pads of the fingers. The toes point forward. Three major pairs of terms are used to describe the location of structures relative to the body as a whole or to other structures (Fig. 1.1). Other terms used to describe positions include proximal and distal, cranial and caudal, and rostral. The basic physics of X-ray generation has not changed. X-rays are photons (a type of electromagnetic radiation) and are generated from a complex X-ray tube, which is a type of cathode ray tube (Fig. 1.2). The X-rays are then collimated (i.e., directed through lead-lined shutters to stop them from fanning out) to the appropriate area, as determined by the radiographic technician. As the X-rays pass through the body they are attenuated (reduced in energy) by the tissues. Those X-rays that pass through the tissues interact with the photographic film. Modifications to this X-ray technique allow a continuous stream of X-rays to be produced from the X-ray tube and collected on an input screen to allow real-time visualization of moving anatomical structures, barium studies, angiography, and fluoroscopy (Fig. 1.3). To demonstrate specific structures, such as bowel loops or arteries, it may be necessary to fill these structures with a substance that attenuates X-rays more than bowel loops or arteries do normally. It is, however, extremely important that these substances are nontoxic. Barium sulfate, an insoluble salt, is a nontoxic, relatively high-density agent that is extremely useful in the examination of the gastrointestinal tract. When barium sulfate suspension is ingested it attenuates X-rays and can therefore be used to demonstrate the bowel lumen (Fig. 1.4). It is common to add air to the barium sulfate suspension, by either ingesting “fizzy” granules or directly instilling air into the body cavity, as in a barium enema. This is known as a double-contrast (air/barium) study. During angiography it is often difficult to appreciate the contrast agent in the vessels through the overlying bony structures. To circumvent this, the technique of subtraction angiography has been developed. Simply, one or two images are obtained before the injection of contrast media. These images are inverted (such that a negative is created from the positive image). After injection of the contrast media into the vessels, a further series of images are obtained, demonstrating the passage of the contrast through the arteries into the veins and around the circulation. By adding the “negative precontrast image” to the positive postcontrast images, the bones and soft tissues are subtracted to produce a solitary image of contrast only. Before the advent of digital imaging this was a challenge, but now the use of computers has made this technique relatively straightforward and instantaneous (Fig. 1.5). Ultrasonography of the body is widely used for all aspects of medicine. Traditionally ultrasound is used for assessing the abdomen (Fig. 1.6) and the fetus in pregnant women. Ultrasound is also widely used to assess the eyes, neck, soft tissues, and peripheral musculoskeletal system. Probes have been placed on endoscopes, and endoluminal ultrasound of the esophagus, stomach, and duodenum is now routine. Endocavity ultrasound is carried out most commonly to assess the genital tract in women using a transvaginal or transrectal route. In men, transrectal ultrasound is the imaging method of choice to assess the prostate in those with suspected prostate hypertrophy or malignancy. The process of magnetic resonance imaging (MRI) is dependent on the free protons in the hydrogen nuclei in molecules of water (H2O). Because water is present in almost all biological tissues, the hydrogen proton is ideal. The protons within a patient’s hydrogen nuclei can be regarded as small bar magnets, which are randomly oriented in space. The patient is placed in a strong magnetic field, which aligns the bar magnets. When a pulse of radio waves is passed through the patient the magnets are deflected, and as they return to their aligned position they emit small radio pulses. The strength and frequency of the emitted pulses and the time it takes for the protons to return to their pre-excited state produce a signal. These signals are analyzed by a powerful computer, and an image is created (Fig. 1.9). By altering the sequence of pulses to which the protons are subjected, different properties of the protons can be assessed. These properties are referred to as the “weighting” of the scan. By altering the pulse sequence and the scanning parameters, T1-weighted images (Fig. 1.10A) and T2-weighted images (Fig. 1.10B) can be obtained. These two types of imaging sequences provide differences in image contrast, which accentuate and optimize different tissue characteristics. From the clinical point of view: Depending on how the radiopharmaceutical is absorbed, distributed, metabolized, and excreted by the body after injection, images are obtained using a gamma camera (Fig. 1.11). High-density contrast medium is ingested to opacify the esophagus, stomach, small bowel, and large bowel. As described previously (p. 6), the bowel is insufflated with air (or carbon dioxide) to provide a double-contrast study. In many countries, endoscopy has superseded upper gastrointestinal imaging, but the mainstay of imaging the large bowel is the double-contrast barium enema. Typically the patient needs to undergo bowel preparation, in which powerful cathartics are used to empty the bowel. At the time of the examination a small tube is placed into the rectum and a barium suspension is run into the large bowel. The patient undergoes a series of twists and turns so that the contrast passes through the entire large bowel. The contrast is emptied and air is passed through the same tube to insufflate the large bowel. A thin layer of barium coats the normal mucosa, allowing mucosal detail to be visualized (see Fig. 1.4). Whenever a patient undergoes an X-ray or nuclear medicine investigation, a dose of radiation is given (Table 1.1). As a general principle it is expected that the dose given is as low as reasonably possible for a diagnostic image to be obtained. Numerous laws govern the amount of radiation exposure that a patient can undergo for a variety of procedures, and these are monitored to prevent any excess or additional dosage. Whenever a radiograph is booked, the clinician ordering the procedure must appreciate its necessity and understand the dose given to the patient to ensure that the benefits significantly outweigh the risks. Table 1.1 The approximate dosage of radiation exposure as an order of magnitude The skeleton can be divided into two subgroups, the axial skeleton and the appendicular skeleton. The axial skeleton consists of the bones of the skull (cranium), vertebral column, ribs, and sternum, whereas the appendicular skeleton consists of the bones of the upper and lower limbs (Fig. 1.12). The skeletal system consists of cartilage and bone. There are three types of cartilage: Cartilage is nourished by diffusion and has no blood vessels, lymphatics, or nerves.
The Body
What is anatomy?
How can gross anatomy be studied?
 With a regional approach, each region of the body is studied separately and all aspects of that region are studied at the same time. For example, if the thorax is to be studied, all of its structures are examined. This includes the vasculature, the nerves, the bones, the muscles, and all other structures and organs located in the region of the body defined as the thorax. After studying this region, the other regions of the body (i.e., the abdomen, pelvis, lower limb, upper limb, back, head, and neck) are studied in a similar fashion.
With a regional approach, each region of the body is studied separately and all aspects of that region are studied at the same time. For example, if the thorax is to be studied, all of its structures are examined. This includes the vasculature, the nerves, the bones, the muscles, and all other structures and organs located in the region of the body defined as the thorax. After studying this region, the other regions of the body (i.e., the abdomen, pelvis, lower limb, upper limb, back, head, and neck) are studied in a similar fashion.
Important anatomical terms
The anatomical position
Terms to describe location
Anterior (ventral) and posterior (dorsal), medial and lateral, superior and inferior
 Anterior (or ventral) and posterior (or dorsal) describe the position of structures relative to the “front” and “back” of the body. For example, the nose is an anterior (ventral) structure, whereas the vertebral column is a posterior (dorsal) structure. Also, the nose is anterior to the ears and the vertebral column is posterior to the sternum.
Anterior (or ventral) and posterior (or dorsal) describe the position of structures relative to the “front” and “back” of the body. For example, the nose is an anterior (ventral) structure, whereas the vertebral column is a posterior (dorsal) structure. Also, the nose is anterior to the ears and the vertebral column is posterior to the sternum.
Proximal and distal, cranial and caudal, and rostral
 Proximal and distal are used with reference to being closer to or farther from a structure’s origin, particularly in the limbs. For example, the hand is distal to the elbow joint. The glenohumeral joint is proximal to the elbow joint. These terms are also used to describe the relative positions of branches along the course of linear structures, such as airways, vessels, and nerves. For example, distal branches occur farther away toward the ends of the system, whereas proximal branches occur closer to and toward the origin of the system.
Proximal and distal are used with reference to being closer to or farther from a structure’s origin, particularly in the limbs. For example, the hand is distal to the elbow joint. The glenohumeral joint is proximal to the elbow joint. These terms are also used to describe the relative positions of branches along the course of linear structures, such as airways, vessels, and nerves. For example, distal branches occur farther away toward the ends of the system, whereas proximal branches occur closer to and toward the origin of the system.
Imaging
Diagnostic imaging techniques
Plain radiography
Contrast agents
Subtraction angiography
Ultrasound
Doppler ultrasound
Magnetic resonance imaging
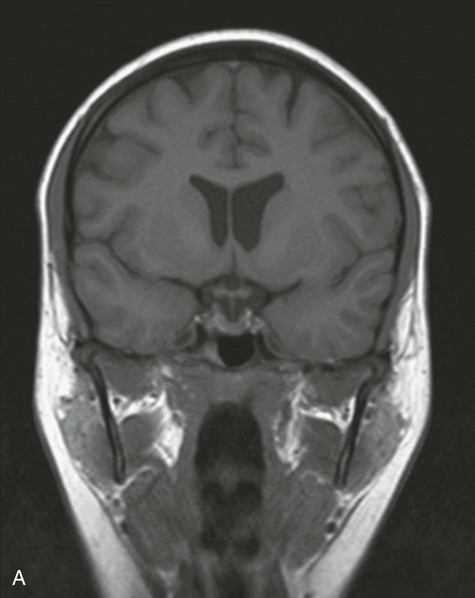
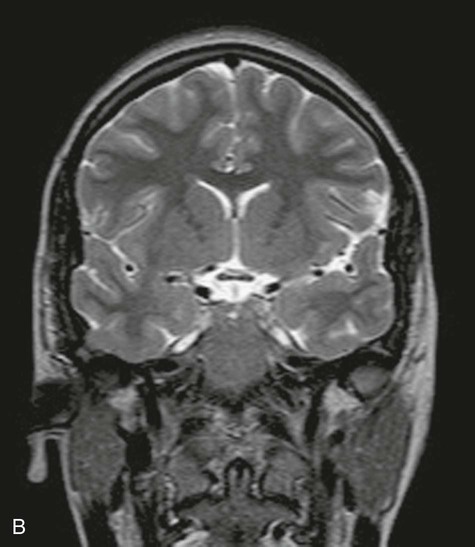
 Most T1-weighted images show dark fluid and bright fat—for example, within the brain the cerebrospinal fluid (CSF) is dark;
Most T1-weighted images show dark fluid and bright fat—for example, within the brain the cerebrospinal fluid (CSF) is dark;
Nuclear medicine imaging
 a reasonable half-life (e.g., 6 to 24 hours),
a reasonable half-life (e.g., 6 to 24 hours),
 an easily measurable gamma ray, and
an easily measurable gamma ray, and
 energy deposition in as low a dose as possible in the patient’s tissues.
energy deposition in as low a dose as possible in the patient’s tissues.
Image interpretation
Plain radiography
Gastrointestinal contrast examinations
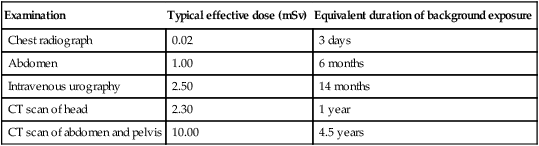
Safety in imaging
Examination
Typical effective dose (mSv)
Equivalent duration of background exposure
Chest radiograph
0.02
3 days
Abdomen
1.00
6 months
Intravenous urography
2.50
14 months
CT scan of head
2.30
1 year
CT scan of abdomen and pelvis
10.00
4.5 years
Body systems
Skeletal system
Cartilage
 hyaline—most common; matrix contains a moderate amount of collagen fibers (e.g., articular surfaces of bones);
hyaline—most common; matrix contains a moderate amount of collagen fibers (e.g., articular surfaces of bones);
Bone
 supportive structures for the body,
supportive structures for the body,
 reservoirs of calcium and phosphorus,
reservoirs of calcium and phosphorus,
 levers on which muscles act to produce movement, and
levers on which muscles act to produce movement, and
 Long bones are tubular (e.g., humerus in upper limb; femur in lower limb).
Long bones are tubular (e.g., humerus in upper limb; femur in lower limb).
 Short bones are cuboidal (e.g., bones of the wrist and ankle).
Short bones are cuboidal (e.g., bones of the wrist and ankle).
 Flat bones consist of two compact bone plates separated by spongy bone (e.g., skull).
Flat bones consist of two compact bone plates separated by spongy bone (e.g., skull).
 Irregular bones are bones with various shapes (e.g., bones of the face).
Irregular bones are bones with various shapes (e.g., bones of the face).
 Sesamoid bones are round or oval bones that develop in tendons.
Sesamoid bones are round or oval bones that develop in tendons.![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Body