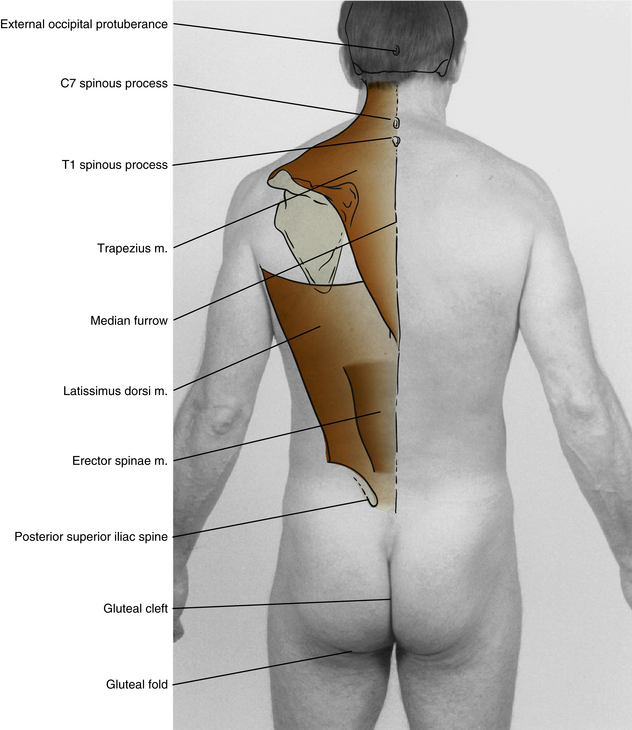
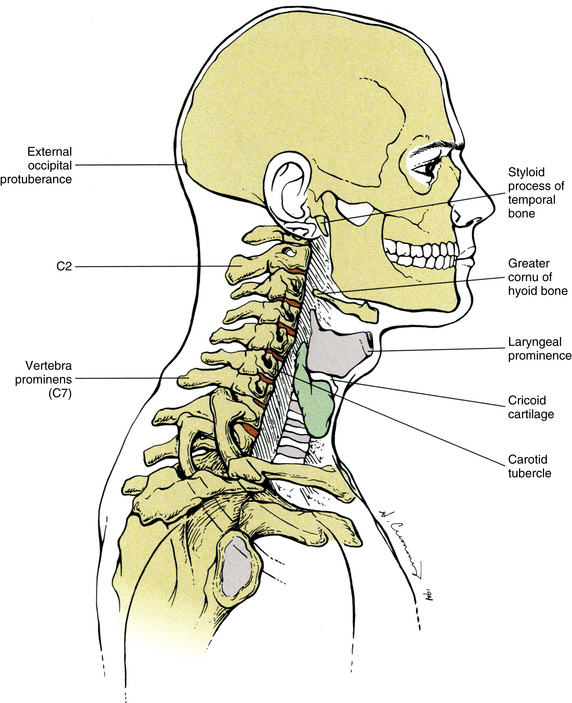
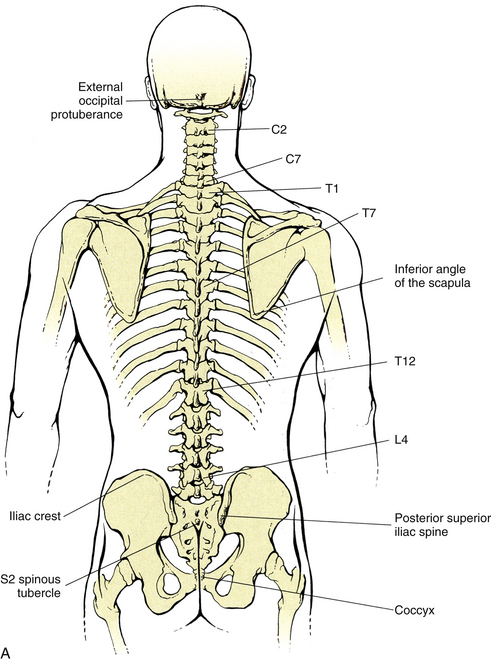
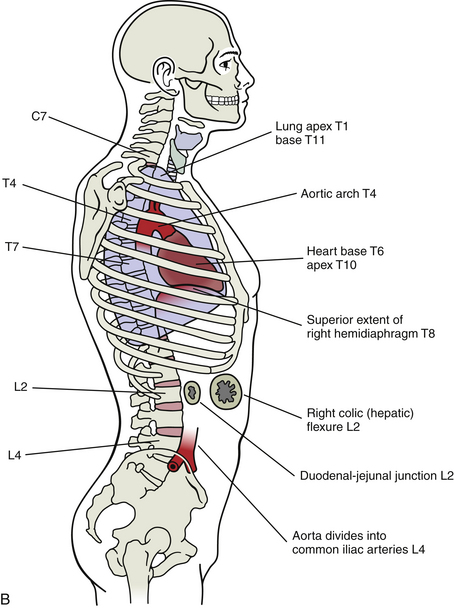
Chapter 1 The locations of structures in reference to the surface of the body are always approximations, although it has been shown that reliability of locating spinal structures by palpation can be enhanced by training and experience (Byfield et al., 1992; Downey et al., 1999; Phillips et al., 2009). Individual variations are common and are influenced by such factors as age, sex, posture, weight, and body type. Respiratory movements also can have marked effects on the locations of structures, especially those of the thorax. Determining the position of the contents of the abdomen can be particularly challenging, and the precise location of abdominal viscera can be established only by verification with appropriate diagnostic imaging procedures. The back, or dorsum, is the posterior part of the trunk and includes skin, muscles, the vertebral column, spinal cord, and various nerves and blood vessels (Gardner, Gray, & O’Rahilly, 1975). The 24 movable vertebrae consist of, from superior to inferior, 7 cervical (C), 12 thoracic (or dorsal) (T), and 5 lumbar (L). Inferior to the lumbar vertebrae, five sacral vertebrae (S) fuse in the adult to form the sacrum. The lowermost three to five vertebrae fuse late in adult life to form the coccyx (Co). Seven processes arise from the posterior portion of the typical vertebra. Several atypical vertebrae have variations in their anatomy and are discussed in Chapters 5, 6, and 7. The spinous process is a midline structure that is directed posteriorly and to a variable degree inferiorly. The transverse processes are a pair of lateral projections. The other four processes are articular, and each vertebra has a superior pair and an inferior pair. These processes are discussed in greater detail in Chapter 2. The remainder of this chapter discusses visual landmarks of the back, palpatory landmarks of the back, spinal cord levels versus vertebral levels, and vertebral levels of structures in the anterior neck and trunk. This information enables the clinician to gain a thorough understanding of surface anatomy and serves as a reference for future patient assessment, both in the physical examination and through diagnostic imaging procedures, including plain film x-ray examination, CT, and MRI. In the midline of the back is a longitudinal groove known as the median furrow (or sulcus) (Fig. 1-1). Superiorly it begins at the external occipital protuberance (EOP) (see the following discussion) and continues inferiorly as the gluteal (anal, natal, or cluneal) cleft (or crena ani) to the level of the S3 spinous tubercle, the remnants of the spinous process of S3. It is shallow in the lower cervical region and deepest in the lumbar region. The median furrow widens inferiorly to form an isosceles triangle with a line connecting the posterior superior iliac spines (PSISs) forming the base above, and the gluteal cleft forming the apex of the triangle below. The PSISs are often visible as a pair of dimples located 3 to 4 cm lateral to the midline at the level of the S2 spinous tubercle. These indentations are known as the lateral lumbar fossae or dimples of Venus. The gluteal fold (or sulcus) is a horizontal skin fold extending laterally from the midline and roughly corresponds with the inferior border of the gluteus maximus muscle. This fold marks the lower extent of the buttocks. Besides these muscles, several bony landmarks usually are visible in the region of the back. The spinous process of C7 (the vertebra prominens) usually is visible in the lower cervical region. Often, the spinous processes of C6 and/or T1 also are visible, especially when the patient’s head is flexed. Approximately 75% of the time, the C7 spinous process is the most prominent of these structures (Stonelake, Burwell, & Webb, 1988). In about 10% and 15% of the population, the C6 and T1 spinous processes, respectively, are actually the most prominent spinous processes in the region. In the adult the vertebral column has several visible normal curves. In the cervical and lumbar regions the spine is anteriorly convex (lordotic), and in the thoracic and sacral areas it is posteriorly convex (kyphotic). Normally there is no lateral deviation of the spinal column, but such curvature is known as scoliosis when present. These curves are covered in more detail in Chapter 2. The EOP (inion) is in the center of the occipital squama (Fig. 1-2). The superior nuchal line extends laterally from the EOP. The transverse process of the atlas may be found directly below and slightly anterior to the mastoid process of the temporal bone. Care must be taken when palpating this structure because of the relatively fragile styloid process of the temporal bone that lies a few millimeters anterior to the C1 transverse process and the great auricular nerve that ascends in the fascia superficial to the C1 transverse process. The spinous process of the axis is the first readily palpable bony structure in the posterior midline below the EOP (see Fig. 1-2), although according to Oliver and Middleditch (1991) the posterior tubercle of C1 may be palpable in some people between the EOP and the spinous process of C2. In the midline below the spinous process of the axis, the second prominent palpable structure is usually the spinous process of C7 or the vertebra prominens. In about 75% of the population the vertebra prominens is the most prominent spinous process, whereas the spinous process of C6 or T1 is more evident in the other 10% and 15% of the population, respectively (Stonelake, Burwell, & Webb, 1988). The other cervical spinous processes are variably more difficult to palpate. The spinous process of C3 is the smallest and can be found at the same horizontal plane as the greater cornua of the hyoid bone. The spinous process of C6 is the last freely movable spinous process with flexion and extension of the neck. The zygapophysial joints between the articular processes of the cervical vertebrae (collectively known as the left and right articular pillars) can be found 1.5 cm lateral of the midline in the posterior neck. With the exception of C1, the tips of the transverse processes of the cervical vertebrae are not individually palpable, but the posterior tubercles of these processes form a bony resistance that may be palpated along a line from the tip of the mastoid process to the root of the neck, approximately a thumb breadth (2.5 cm) lateral of the midline. The anterior aspects of the transverse processes of the cervical vertebrae may be found in the groove between the larynx and sternocleidomastoid muscle (SCM). It may be necessary to slightly retract the SCM laterally to palpate these structures. The anterior tubercles of the transverse processes of C6 are especially large and are known as the carotid tubercles (see Fig. 1-2). These may be palpated at the level of the cricoid cartilage. Care must be taken when locating the carotid tubercles (and the other cervical transverse processes), because they are in the proximity of the common carotid arteries, and they always should be palpated unilaterally. The spinous process of T1 is usually the third prominent bony structure in the midline below the EOP; the spinous processes of C2 and C7 are the first and second, respectively (Fig. 1-3). Note that in about 10% of the population, the C6 spinous process is also very prominent. The spinous process of T3 is located at the same horizontal plane as the root of the spine of the scapula. The spinous process of T4 is located at the extreme of the convexity of the thoracic kyphosis; therefore it is usually the most prominent spinous process below the root of the neck. When patients are standing or sitting with their upper extremities resting along the sides of their trunk, the inferior scapular angle usually is at the horizontal level of the spinous process of T8 (Cooperstein & Haneline, 2007; Haneline et al., 2008). This changes when the patient is lying prone with his or her upper extremities resting toward the floor in a flexed position (the most common posture of the patient when this region of the back is palpated). In this position the scapulae are rotated so that the T9 spinous process is more commonly found at the level of the inferior scapular angle (Cooperstein et al., 2009). Because the spinous processes of the thoracic vertebrae project in an inferior direction to different degrees, the remainder of the vertebrae are located variably superior to the tip of the spinous process of the same vertebral segment (Keogh & Ebbs, 1984). The tips of the transverse processes of T1-4 and T10-12 are located one spinous interspace superior to the tip of the spinous process of the same segment. The tips of the transverse processes of T5-9 are located two spinous interspaces superior to the tips of their respective spinous processes because these spinous processes project inferiorly to a greater degree. For example, the tips of the transverse processes of T3 are located in the same horizontal plane as the inferior tip of the spinous process of T2, whereas the tips of the transverse processes of T8 are at the same horizontal plane as the inferior tip of the spinous process of T6. The transverse processes of the thoracic vertebrae progressively shorten from superior to inferior, so that the tips of the transverse processes of T1 are located 3 cm lateral to the midline, although those of T12 are 2 cm. Sometimes the transverse processes of T12 are small and not readily palpable. The angles of the ribs may be palpated 4 cm lateral to the midline at the horizontal levels of their respective transverse processes. The posterior aspects of the spinous processes of the lumbar vertebrae differ from those of the thoracic vertebrae in that they present more of a flat surface. The spinous processes of L4 and L5 are shorter than the other lumbar spinous processes and are difficult to palpate, especially the L5 spinous process. The spinous process of L4 is the most inferior spinous process that has palpable movement with flexion and extension of the trunk. In the past the L4 spinous process was considered to be in a horizontal plane with the superior margin of the iliac crests (the supracristal plane), although in approximately 20% of the population the tops of the iliac crests were thought to be aligned with the spinous process of L5 (Oliver & Middleditch, 1991). However, more recent evidence, using ultrasound to localize intervertebral levels, shows the supracristal plane to be at the level of L3-4 in nearly 75% of normal volunteers. In the remainder of the healthy population, this plane is fairly evenly found at either L2-3 or L4-5 (Pysyk et al., 2010).
Surface Anatomy of the Back and Vertebral Levels of Clinically Important Structures
The Back
Visual Landmarks of the Back
Palpatory Landmarks of the Back
Cervical Region
Thoracic Region
Lumbosacral Region
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Surface Anatomy of the Back and Vertebral Levels of Clinically Important Structures