Chapter 4
Muscles That Influence the Spine
Second only to the vertebral column and spinal cord, the muscles of the spine are the most important structures of the back. A thorough understanding of the back muscles is fundamental to a comprehensive understanding of the spine and its function. The purpose of this chapter is to discuss the muscles of the back and other muscles that have an indirect influence on the spine. The intercostal muscles provide an example of the latter category. These muscles do not actually attach to the spine, but their action can influence the spine by virtue of their attachment to the ribs. The abdominal wall muscles, diaphragm, hamstrings, and others can be placed into this same category. These muscles have a less direct yet important influence on the spine. Chapter 5 discusses the sternocleidomastoid, scalene, suprahyoid, and infrahyoid muscles.
There is a complicated interplay of many muscles when a motion of the body, especially of the spine, is produced. Sometimes this is termed muscle coordination. Some of the specifics of this complex interplay are only beginning to be understood, especially in asymmetric motions of the trunk (van Dieen, 1996; Danneels et al., 2001; Andersson et al., 2002; Masani et al., 2009; Shin & D’Souza, 2010; Comfort, Pearson, & Mather, 2011). Muscles known as prime movers are the most important. Other muscles, known as synergists, assist the prime movers. For example, the psoas major and rectus abdominis muscles are prime movers of the spine during flexion of the lumbar spine from a supine position, as in the performance of a sit-up. However, the erector spinae muscles also undergo an eccentric contraction toward the end of the sit-up. This contraction of the erector spinae group helps to control the motion of the trunk and allows a graceful, safe accomplishment of the movement. The erector spinae muscles are acting as synergists in this instance.
Besides producing motion, muscle contraction also stabilizes the spine by making it stiffer. This is important not only for maintaining posture (Cholewicki et al., 1997; Quint et al., 1998) but also for providing a stable base for other motions of the body, such as appendicular motions (Lorimer Moseley et al., 2002; Akuthota et al., 2008; Borghuis et al., 2008; Zazulak et al., 2008).
Muscle coordination seems to be under the control of the central nervous system. The central nervous system is constantly receiving afferent information from the muscles and other surrounding tissues, such as ligaments and tendons. On the basis of this information, the central nervous system appears to use reflex pathways to finely control muscle activity. Some of the details of this process are beginning to be understood (Kang et al., 2002; Hultborn, 2006). Interestingly, the specifics of the interplay of the muscles in producing a motion of the body are not always constant. In other words, the same motion may not always be produced by the same muscles working together in the same way. The central nervous system can alter muscle activity depending on the circumstances, such as muscle fatigue, to accomplish the same goal (Clark et al., 2003). This appears to be especially true when there is an abnormality in the system, such as pain or abnormal joint function (McPartland et al., 1997; Hirayama et al., 2001; Lehman et al., 2001; van Dieen et al., 2003; Tsao, Galea, & Hodges, 2008).
The muscles of the spine and other muscles associated with the back can, and frequently do, sustain injury. Other painful conditions of muscles (or fascia) are commonly seen by clinicians besides frank injury or pathology of muscles. For example, fatigue of the back muscles can be a source of pain (e.g., motion-induced intermittent low back pain) (Takahashi et al., 2007). In addition, myofascial trigger points can be a source of pain and are sometimes associated with a condition known as myofascial pain syndrome (Travell & Simons, 1983, 1992; Wheeler, 2004). Another condition is fibromyalgia or fibromyalgia syndrome (Krsnich-Shriwise, 1997; Arnold, 2010). Both of these conditions are not well understood but are being increasingly accepted as true syndromes. They are similar in presentation but are distinct entities (Schneider, 1995). A complete understanding of the anatomy of the muscles associated with the spine aids in the differential diagnosis of pain arising from muscles versus pain arising from neighboring ligaments or other structures.
The back muscles are discussed from superficial to deep. This is accomplished by dividing the muscles into six layers, with layer one the most superficial and layer six the deepest. Other important muscles of the spine are described after a discussion of the six layers of back muscles. These include the suboccipital muscles, small muscles of the spine, anterior and lateral muscles of the cervical spine, and iliac muscles. The muscles that have an indirect yet important influence on the spine are discussed last. The muscles that influence the spine are summarized in Tables 4-1 and 4-2 and Box 4-1 (Table 4-2 and Box 4-1 are found at the end of the chapter).
BOX 4-1 Summary of Actions of Spinal Muscles
Muscles Acting on the Head at the Atlanto-Axial and Atlanto-Occipital Joints
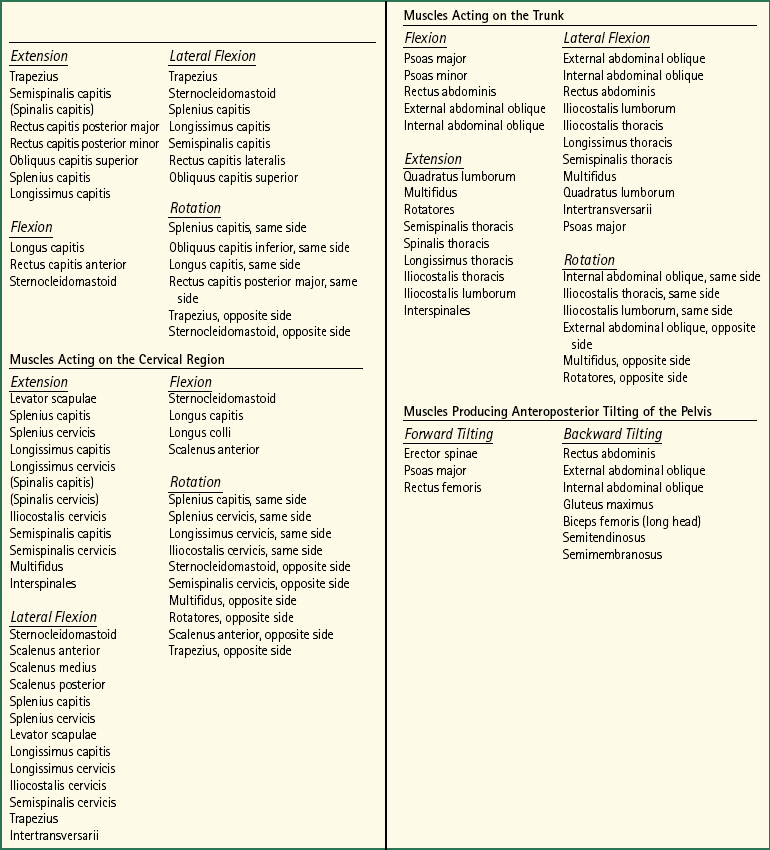
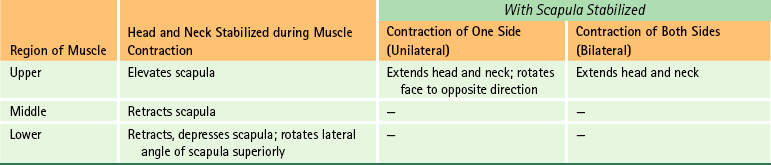
Table 4-2
Summary of Muscles Affecting the Spine1
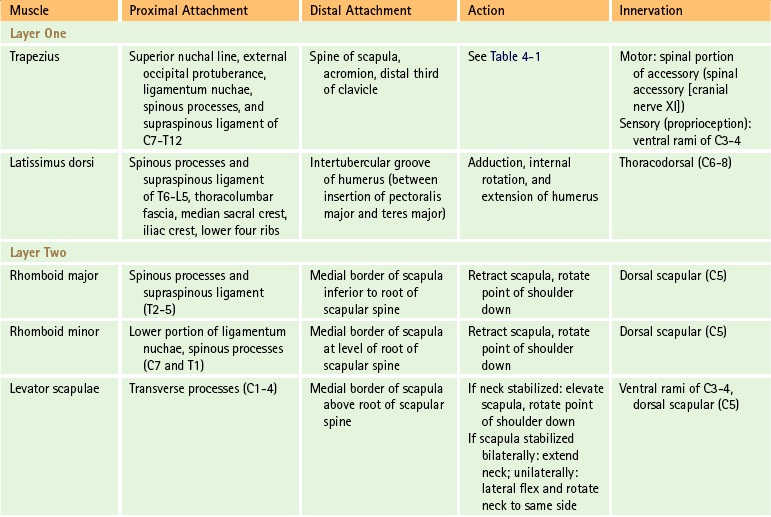
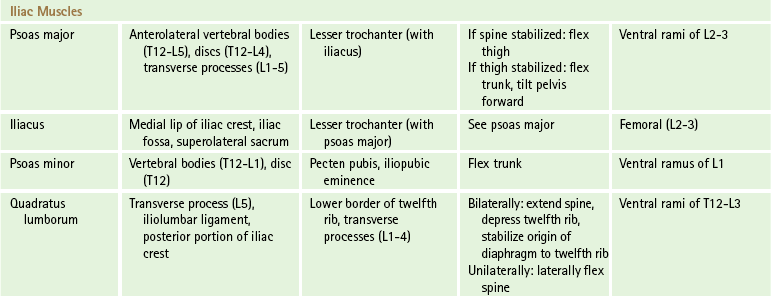
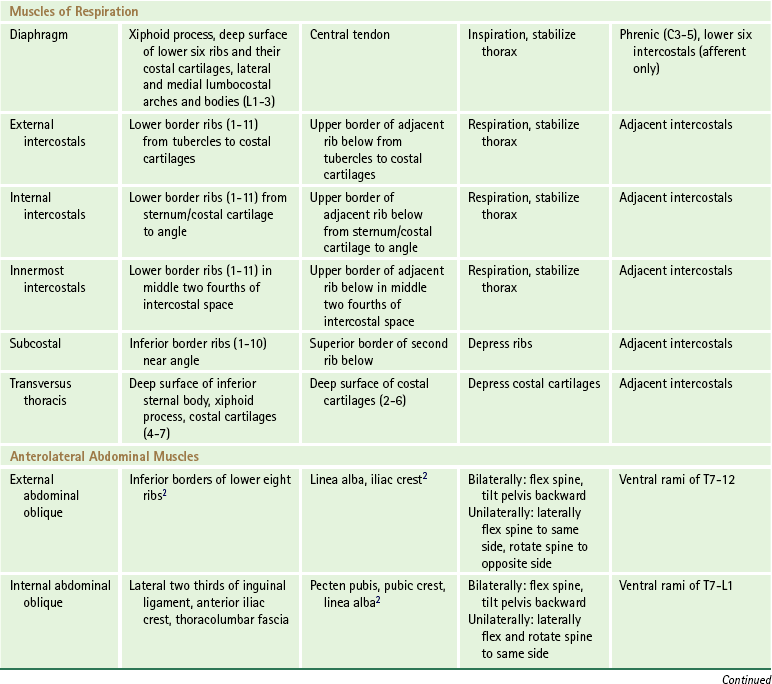
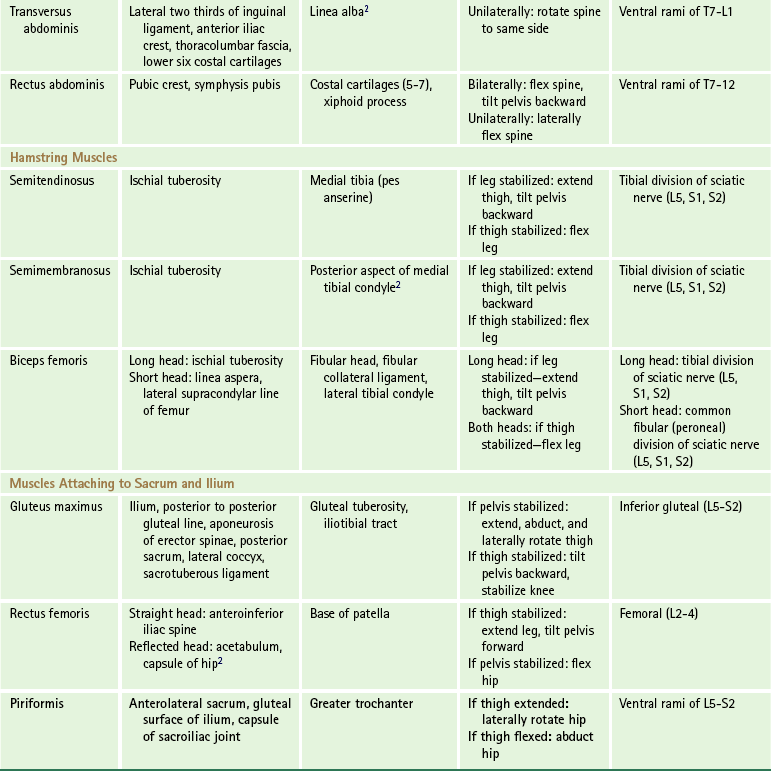
1See Tables 5-10 through 5-12 for information on the scalene, sternocleidomastoid, and suprahyoid and infrahyoid muscles.
Six Layers of Back Muscles
The first layer of back muscles consists of the trapezius and latissimus dorsi muscles (Fig. 4-1). These two muscles course from the spine (and occiput) to either the shoulder girdle (scapula and clavicle) or the humerus, respectively.
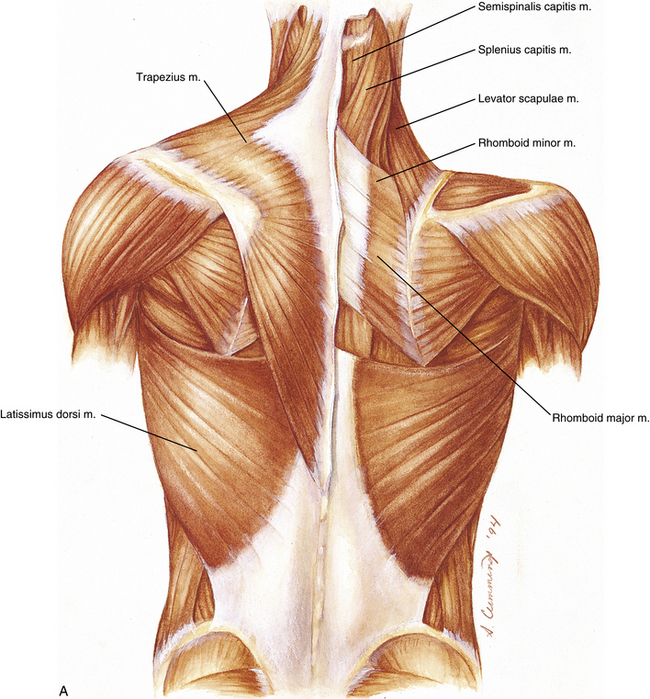
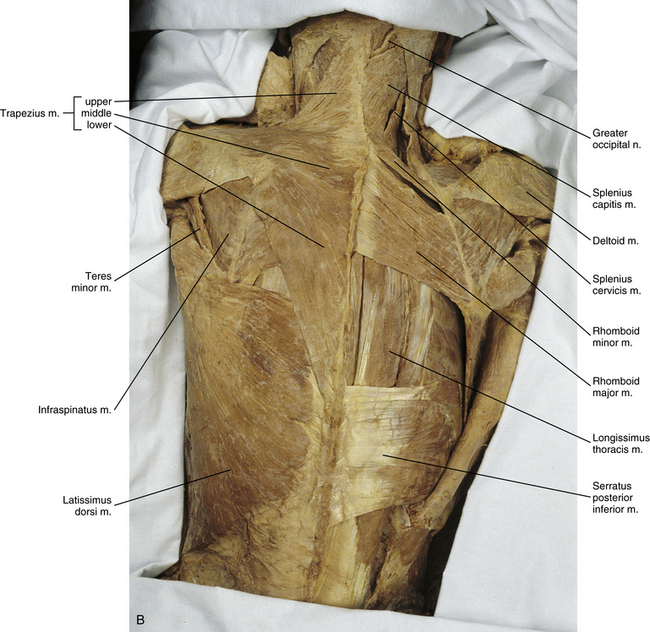
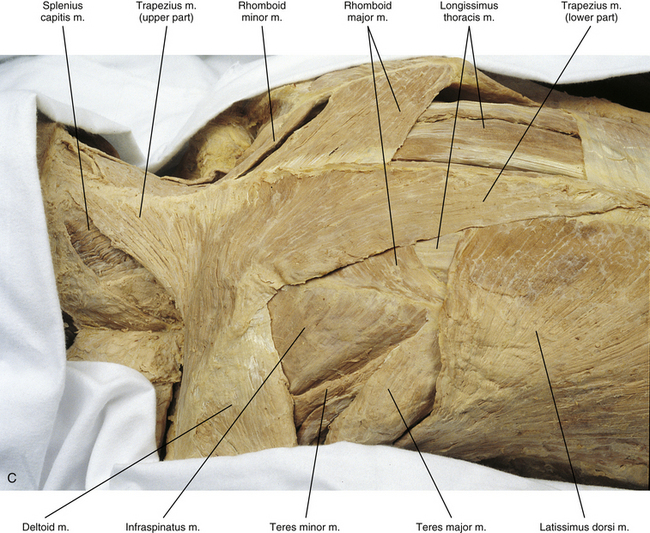
FIG. 4-1 A, First (left) and second (right) layers of back muscles. B, Dissection of these same two layers. C, Close-up, taken from a left posterior oblique perspective. The serratus posterior inferior muscle of the third layer can also be seen in panel B and in Figure 4-2, A and B.
Trapezius Muscle
The trapezius muscle is the most superficial and superior back muscle (see Fig. 4-1). It is a large, strong muscle that is innervated by the accessory nerve (cranial nerve XI). In addition to its innervation from the accessory nerve, the trapezius muscle receives some proprioceptive fibers from the third and fourth cervical ventral rami. Because the trapezius muscle is so large, it has many attachment sites. This muscle arises in the midline from the superior nuchal line, external occipital protuberance, ligamentum nuchae of the posterior neck, spinous processes of C7 to T12, and supraspinous ligament between C7 and T12. It attaches distally onto the spine of the scapula, acromion, and distal third of the clavicle. Detailed morphometric measurements have been performed on this muscle (Kamibayashi & Richmond, 1998).
Because of its size and the many locations of its attachments, the trapezius muscle also has many actions. Most of these actions result in movement of the neck and scapula (i.e., the “shoulder girdle” as a whole). The function of the trapezius muscle depends on which region of the muscle is contracting (upper, middle, or lower). The middle portion retracts the scapula, whereas the lower portion depresses the scapula and at the same time rotates the scapula so that its lateral angle moves superiorly (i.e., rotates the point of the shoulder up). The actions of the upper part of the trapezius muscle also depend on whether the head or neck or the scapula is stabilized. When moving the head and neck, the actions of the upper fibers of the trapezius muscle are also determined by whether the muscle is contracting unilaterally or bilaterally. When the head and neck are stabilized by other muscles, then there is some conflicting evidence as to whether the upper fibers of the trapezius muscle help in elevation of the scapula. Based upon information gathered from cadaveric dissections of the attachment points and directions of the upper fibers of the trapezius muscle, Johnson and colleagues (1994) concluded that these fibers do not aid in elevation of the scapula. On the other hand, there is good electromyographic evidence that the upper fibers of the trapezius muscle are active during elevation of the shoulder (Campos et al., 1994; Guazzelli et al., 1994). Table 4-1 summarizes the actions of the trapezius muscle and Table 4-2 summarizes all of the muscles that are discussed in this chapter.
Latissimus Dorsi Muscle
The latissimus dorsi muscle is the more inferior and lateral of the two muscles that constitute the first layer of back muscles (see Fig. 4-1). This large muscle has an extensive region for its proximal attachment, which includes the following:
• Spinous processes and supraspinous ligament of T6-L5 (although the supraspinous ligament ends between L2 and L4)
• Posterior sacrum (median sacral crest) (see Chapter 8)
Thoracolumbar (or Lumbodorsal) Fascia
Because of its clinical significance, the anatomy of the thoracolumbar fascia deserves further discussion. This fascia extends from the thoracic region to the sacrum. It forms a thin covering over the erector spinae muscles in the thoracic region, whereas in the lumbar region the thoracolumbar fascia is strong and is composed of three layers. The posterior layer attaches to the lumbar spinous processes, interspinous ligaments between these processes, and median sacral crest. This layer has its own superficial and deep laminae (Macintosh & Bogduk, 1987a). This posterior layer is a strong sheet of dense connective tissue that links two of the largest muscles of the body—latissimus dorsi and gluteus maximus. It is, therefore, important in transferring forces between the spine, pelvis, and lower limbs (Vleeming & Stoeckart, 2007). The middle layer attaches to the tips of the lumbar transverse processes and intertransverse ligaments and extends superiorly from the iliac crest to the twelfth rib. The anterior layer covers the anterior aspect of the quadratus lumborum muscle and attaches to the anterior surfaces of the lumbar transverse processes. Superiorly the anterior layer forms the lateral arcuate ligament (see Diaphragm). The anterior layer continues inferiorly to the ilium and iliolumbar ligament. The posterior and middle layers surround the erector spinae muscles posteriorly and anteriorly, respectively (see Fifth Layer), and meet at the lateral edge of the erector spinae, where these two layers are joined by the anterior layer (Standring et al., 2008). Barker and Briggs (1999) have demonstrated in a cadaveric study that the thoracolumbar fascia may continue more superiorly than classically described. They found that the superficial lamina of the posterior layer ran superiorly to be continuous with the rhomboid muscles, whereas the deep lamina of the posterior layer was continuous superiorly with the splenius muscles. These superior extensions of the fascia were of variable thickness, but seemed thick enough to transmit tension. This means that the thoracolumbar fascia may have a more global influence on biomechanics than thought previously.
The lateral union of the three principal layers of the thoracolumbar fascia serves as a posterior aponeurosis for origin of the transversus abdominis muscle. More recent evidence has shown that because of its indirect attachment to the lumbar transverse processes via the thoracolumbar fascia, the transversus abdominis muscle may play a greater role in lumbar segmental control than previously believed (Barker et al., 2007). The direction of the fibers within each lamina of the posterior layer makes the thoracolumbar fascia stronger along its lines of greatest stress. When the thoracolumbar fascia is tractioned laterally by the action of the abdominal muscles, the distinct direction of fibers of the posterior layer’s two laminae helps aid in extension of the spine and the maintenance of an erect posture.
Some investigators believe that because the posterior and middle layers surround the erector spinae muscles, injury to these muscles at times may lead to a “compartment” type of syndrome within these two layers of the thoracolumbar fascia (Peck et al., 1986). This syndrome results from edema within the erector spinae muscles. The edema stems from injury and increases the pressure in the relatively closed compartment composed of the erector spinae muscles wrapped within the posterior and middle layers of the thoracolumbar fascia. This may result in increased pain and straightening of the lumbar lordosis (Peck et al., 1986). However, further research is necessary to determine the best approach available to diagnose this condition and the frequency with which it occurs.
Second Layer
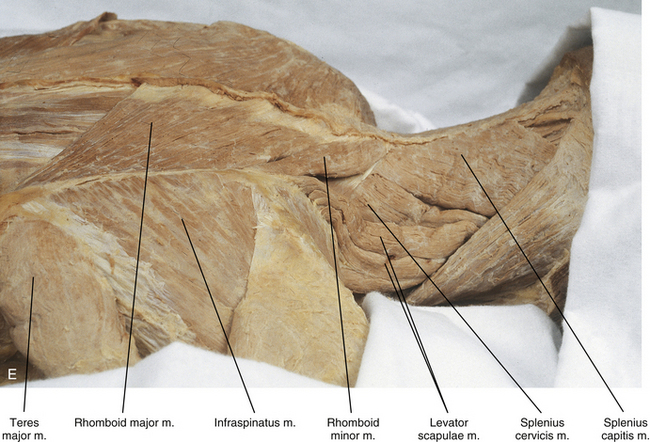
The second layer of back muscles includes three muscles that, along with the first layer, connect the upper limb to the vertebral column. All three muscles lie deep to the trapezius muscle and attach distally onto the scapula’s medial border. They include the rhomboid major, rhomboid minor, and levator scapulae muscles (see Fig. 4-1). Detailed morphometric measurements have been performed on these muscles (Kamibayashi & Richmond, 1998).
Levator Scapulae Muscle
The levator scapulae muscle arises by tendinous slips from the transverse processes of the atlas and axis (see Chapter 5) and the posterior tubercles of the transverse processes of C3 and C4. Its fibers descend and attach onto the scapula’s medial border between the root of the scapular spine and the superior angle. It is innervated by branches from the ventral rami of the C3 and C4 spinal nerves and the dorsal scapular nerve (C5). If the cervical spine is fixed, the levator scapulae muscle helps in elevating and rotating the scapula such that the lateral angle moves inferiorly (i.e., rotates the point of the shoulder down). When the scapula is stabilized, contraction of this muscle laterally flexes and rotates the neck to the same side. Bilateral contraction helps in extension of the cervical spine.
Third Layer
The third layer of back muscles consists of two thin, almost quadrangular muscles: the serratus posterior superior and serratus posterior inferior (Fig. 4-2, A and B).
Serratus Posterior Superior and Serratus Posterior Inferior Muscles
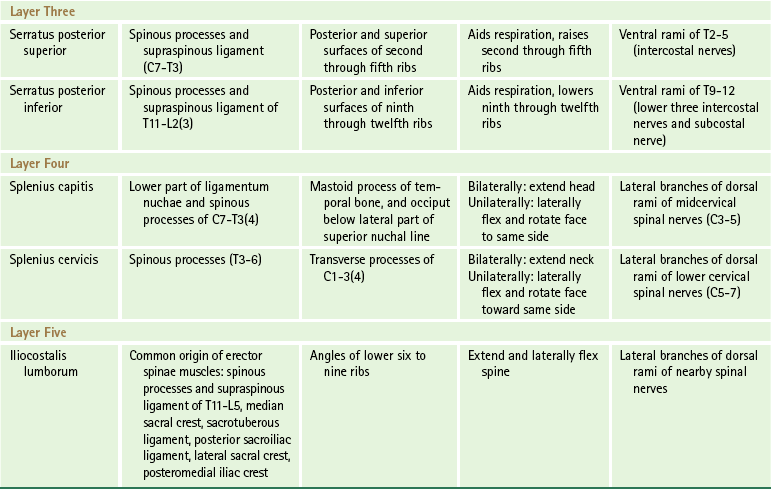
The serratus posterior inferior muscle arises from the spinous processes and intervening supraspinous ligament of T11 to L2. Its fibers run superolaterally to attach onto the posterior and inferior surfaces of the lower four ribs, and this muscle is innervated by the lower three intercostal nerves (T9 to T11) and the subcostal nerve. These nerves are all anterior primary divisions of their respective spinal nerves. The serratus posterior superior and inferior muscles may help with respiration. More specifically, the serratus posterior superior muscle elevates the second through fourth ribs, which may aid inspiration. The serratus posterior inferior muscle lowers the ninth through twelfth ribs, which may help with forced expiration. However, electromyographic evidence refutes a respiratory function for these muscles (Vilensky et al., 2001); they may function primarily in proprioception.
Fourth Layer
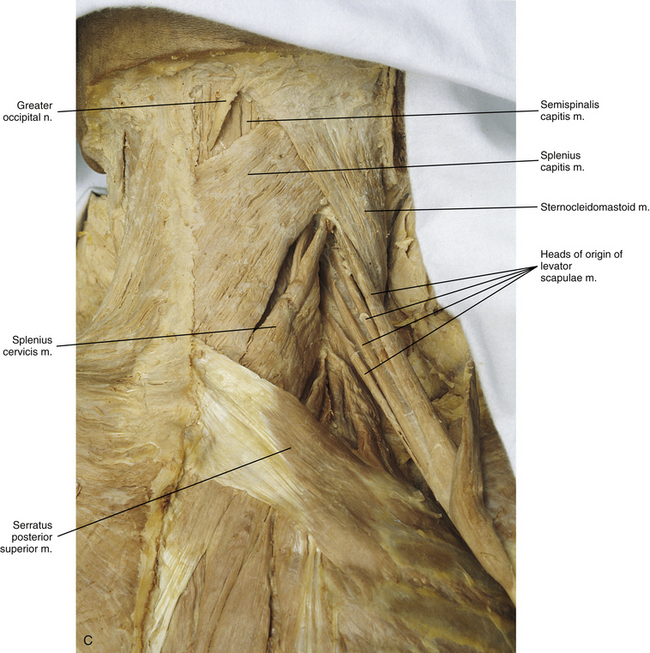
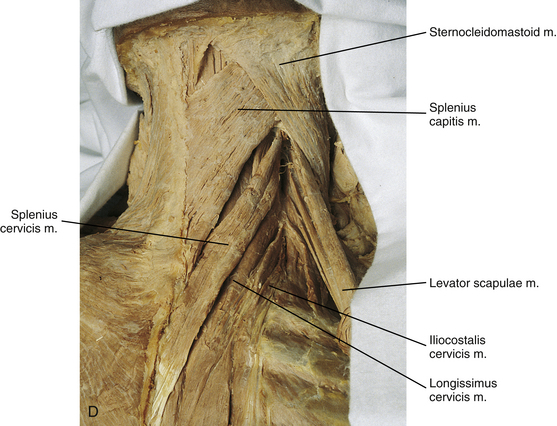
The most superficial layer of deep back muscles is the fourth layer, which consists of two muscles whose fibers ascend in a superolateral direction. This layer is composed of the splenius capitis and splenius cervicis muscles (Fig. 4-2, C to E). Detailed morphometric measurements have been performed on these muscles (Kamibayashi & Richmond, 1998).
Splenius Capitis and Splenius Cervicis Muscles
The splenius cervicis muscle arises from the spinous processes of T3 through T6, and its fibers run parallel to the fibers of the splenius capitis muscle to attach superiorly onto the transverse processes of the atlas and axis and the posterior tubercles of the transverse processes of C3 and sometimes C4. These attachment sites are deep to the origins of the levator scapulae. The splenius capitis and cervicis muscles are innervated by lateral branches of the posterior primary divisions (dorsal rami) of the midcervical and lower cervical spinal nerves, respectively. When the splenius muscles of both sides act together, they extend the head and neck. When the muscles of one side contract, they laterally flex the head and neck and slightly rotate the face toward the side of contraction.
Fifth Layer
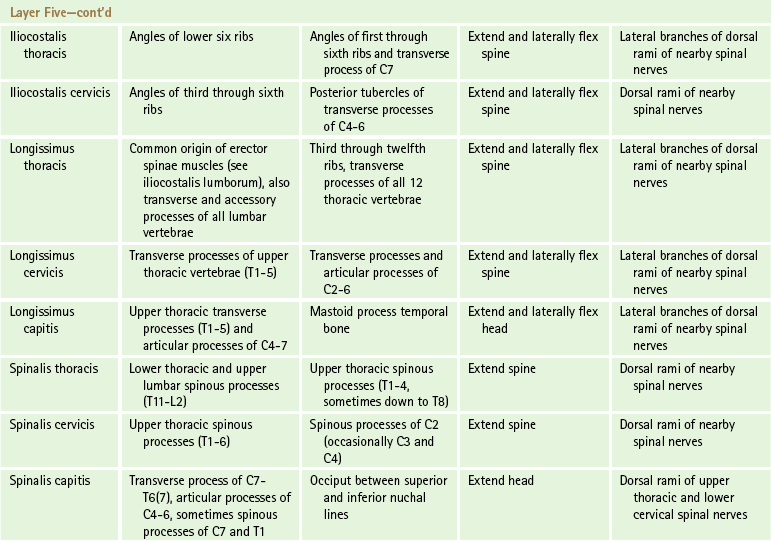
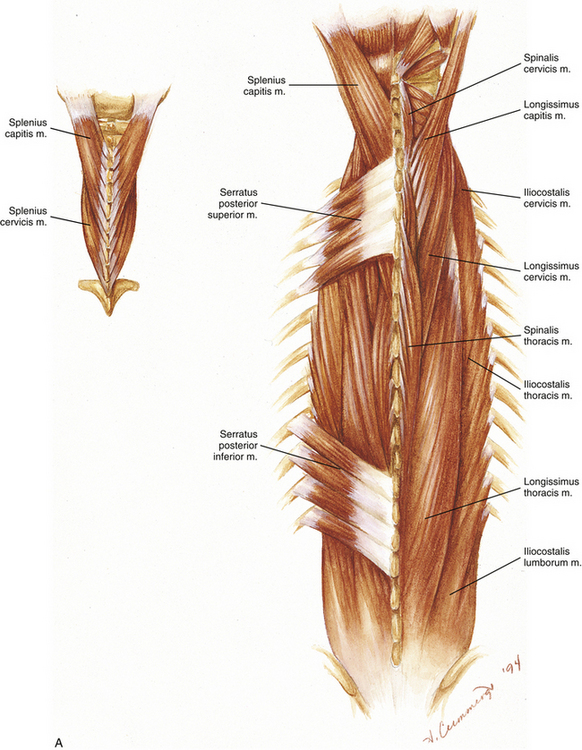
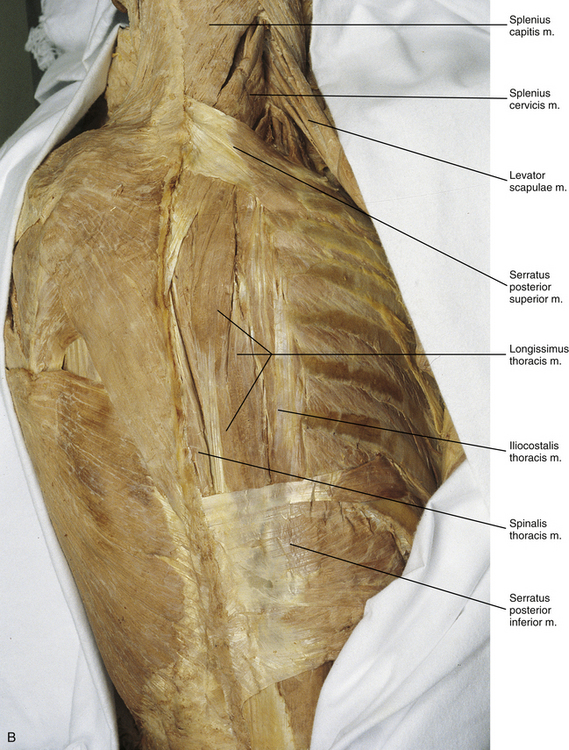
The largest group of back muscles is the fifth layer. This layer is composed of the erector spinae group of muscles (Fig. 4-3, A; see also Fig. 4-2, A and B). This erector spinae group is also collectively known as the sacrospinalis muscle. The muscles that comprise this group are a series of longitudinal muscles that course the length of the spine, filling a groove lateral to the spinous processes. Because of this location, these muscles generally have a similar function, which is to extend and laterally flex the spine. The erector spinae muscles are all segmentally innervated by lateral branches of the posterior primary divisions (dorsal rami) of the nearby spinal nerves and are covered posteriorly in the thoracic and lumbar regions by the thoracolumbar fascia. These longitudinal muscles can be divided into three groups. These three groups are, from lateral to medial, the iliocostalis, the longissimus, and the spinalis groups of muscles. Each of these groups, in turn, consists of three subdivisions. The subdivisions are named according to the general area of the spine to which they insert (e.g., lumborum, thoracis, cervicis, capitis). The descriptions that follow attempt to simplify the arrangement of the erector spinae group as much as possible. In reality, there is much individual variation in the actual arrangements of these muscles with many long sequentially overlapping multisegmental bundles and diverse multilayered insertions (Nomizo & Sakai, 2009). This complex arrangement also leads to apparent discrepancies in the segmental innervation pattern of this group of muscles. The erector spinae muscles are discussed from the most lateral group to the most medial, and each group is discussed from inferior to superior.
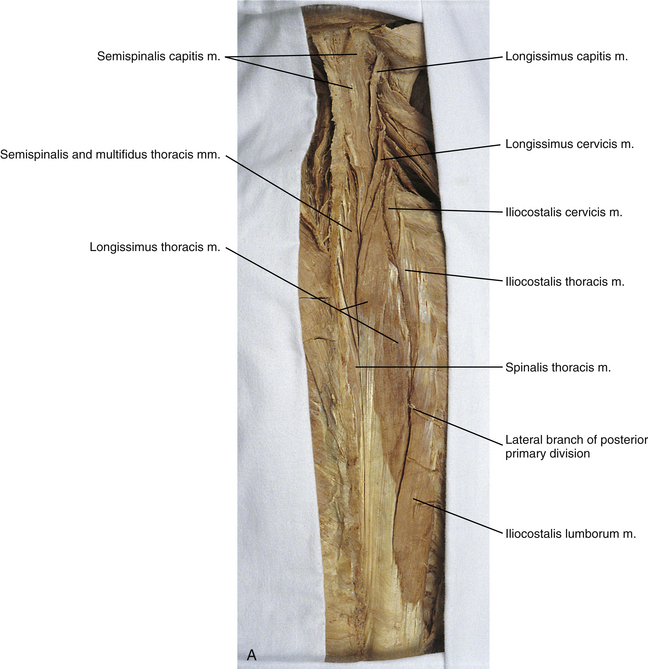
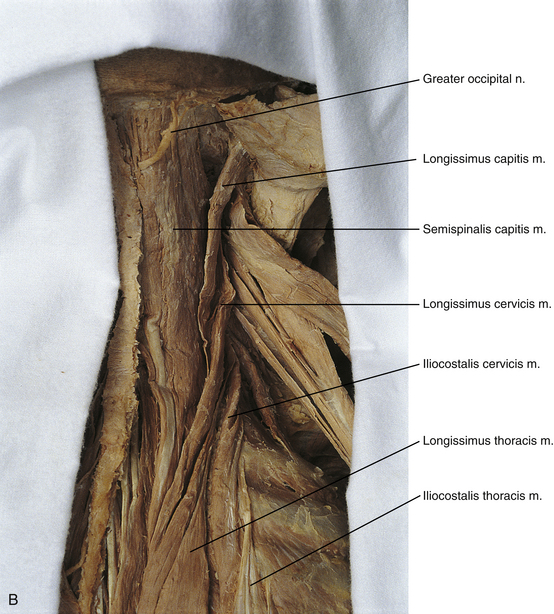

Iliocostalis Muscles
The iliocostalis (iliocostocervicalis) group of muscles is subdivided into lumborum, thoracis, and cervicis muscles (see Fig. 4-3, A and B). Inferiorly the iliocostalis muscles derive from the common origin of the erector spinae muscles.
Iliocostalis lumborum: The iliocostalis lumborum muscle is the most inferior and lateral of the erector spinae muscles. It originates from the common origin of the erector spinae muscles, which includes the following:
• Spinous processes and supraspinous ligament of T11 through L5 (supraspinous ligament ends between L2 and L4)
• Long posterior sacroiliac ligament
The iliocostalis lumborum muscle runs superiorly to attach onto the posterior and inferior surfaces of the angles of the lower six to nine ribs. This muscle extends and laterally flexes the thoracolumbar spine and is innervated by lateral branches of the posterior primary divisions of lumbar and lower thoracic spinal nerves.
Macintosh and Bogduk (1987b) further described the anatomy of the iliocostalis lumborum muscle based on a series of elegant dissections. They found that part of this muscle arises from the posterior superior iliac spine and the posterior aspect of the iliac crest and ascends to attach onto the lower eight or nine ribs. They called this part the iliocostalis lumborum pars thoracis. Another part of the classically described iliocostalis lumborum muscle begins from the tips of the lumbar spinous processes and associated middle layer of the thoracolumbar fascia of L1 to L4 (see Thoracolumbar [or Lumbodorsal] Fascia) and attaches onto the anterior edge of the iliac crest. They called this part the iliocostalis lumborum pars lumborum and found that it formed a considerable mass of muscle. More recent evidence from the Visible Human Project corroborates this classification (Daggfeldt et al., 2000).
Iliocostalis thoracis: The iliocostalis thoracis muscle starts from the superior aspect of the angles of the lower six ribs and ascends to end on the angles of approximately the upper six ribs and transverse process of the C7 vertebra. This muscle extends and laterally flexes the thoracic spine and is innervated by the lateral branches of the posterior primary divisions (dorsal rami) of the thoracic spinal nerves.
Iliocostalis cervicis: The iliocostalis cervicis muscle arises from the superior aspect of the angle of the third through sixth ribs and attaches superiorly onto the posterior tubercles of the transverse processes of the C4 to C6 vertebrae. It laterally flexes and extends the lower cervical region and is innervated by the dorsal rami of the upper thoracic and lower cervical spinal nerves.
Longissimus Muscles
The longissimus muscles are located medial to the iliocostalis group. The longissimus group consists of thoracis, cervicis, and capitis divisions. The lateral branches of the posterior primary divisions (dorsal rami) of the spinal nerves exit the thorax and then course laterally and posteriorly between the iliocostalis muscles and longissimus thoracis muscle (see Fig. 4-3, A). This fact is used in the gross anatomy laboratory not only to quickly find the lateral branches of the posterior primary divisions, but also to demonstrate the separation between these two large muscle masses. After providing motor and sensory innervation to the sacrospinalis muscle, the lateral branches continue to the skin of the back, providing cutaneous sensory innervation.
Longissimus thoracis: The longissimus thoracis muscle is the largest of the erector spinae muscles. It arises from the common origin of the erector spinae muscles (see Iliocostalis Lumborum). In addition, many fibers begin from the transverse and accessory processes of the lumbar vertebrae (see Chapter 7). This muscle is the longest muscle of the back, thus the name longissimus. It ends superiorly on the third through twelfth ribs, between their angles and tubercles (see Chapter 6). The longissimus thoracis muscle also attaches onto the transverse processes of all 12 thoracic vertebrae. This muscle functions to hold the thoracic and lumbar regions erect, and laterally flexes the spine when it acts unilaterally. It is innervated by lateral branches of the thoracic and lumbar posterior primary divisions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


