Squamous Cell Carcinoma In Situ (Bowen Disease)
David Cassarino, MD, PhD
Key Facts
Terminology
Squamous cell carcinoma in situ (SCCis)
Synonyms: Bowen disease, squamous intraepithelial neoplasia
Full thickness intraepidermal atypia of squamous keratinocytes often with numerous mitotic figures and apoptotic cells
Etiology/Pathogenesis
Chronic UV radiation strongly implicated in SCCis
Some cases of SCCis are related to HPV infection, particularly in anogenital sites
Clinical Issues
Small risk for invasive squamous cell carcinoma
Most common on head and neck region, other sun-exposed sites
Microscopic Pathology
Cells are usually markedly enlarged and atypical appearing, with nuclear hyperchromasia and enlarged nucleoli
Basilar keratinocytes are often spared, leading to so-called “eyeliner” sign
Overlying parakeratosis is usually diffusely present, without skip areas over adnexal structures
Numerous intraepidermal mitotic figures and apoptotic figures typically present
Top Differential Diagnoses
Actinic keratosis (AK)
Invasive squamous cell carcinoma (SCC)
Paget disease and other pagetoid in situ carcinomas
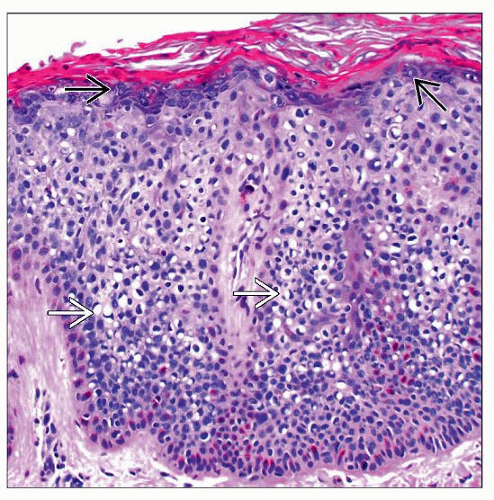 Bowen disease (SCCis) is characterized by a proliferation of atypical intraepidermal keratinocytes filling the entire epidermis, including the granular layer  . Many of the cells show cytoplasmic clearing . Many of the cells show cytoplasmic clearing  . . |
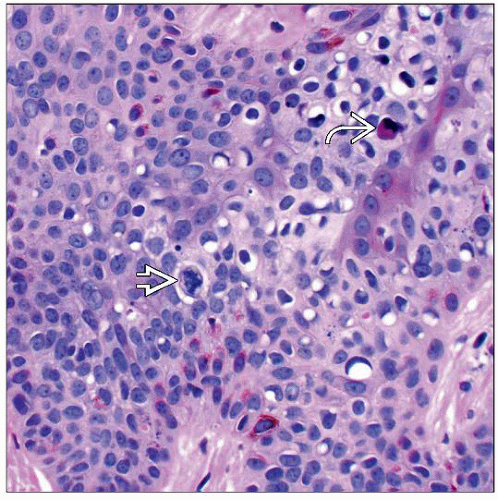 High magnification of Bowen disease shows prominent cytologic atypia, an atypical mitotic figure  in the mid-epidermis, and apoptotic cells in the mid-epidermis, and apoptotic cells  . . |
TERMINOLOGY
Abbreviations
Squamous cell carcinoma in situ (SCCis)
Synonyms
Bowen disease
Squamous intraepithelial neoplasia (SIN)
Definitions
Full thickness intraepidermal atypia of squamous keratinocytes often with numerous mitotic figures and apoptotic cells
ETIOLOGY/PATHOGENESIS
Sun Exposure
Chronic UV radiation strongly implicated in SCCis
Immunosuppression
Increased risk of developing SCCis in immunosuppressed patients, especially organ transplant recipients
HPV Infection
Some cases of SCCis are related to HPV infection, particularly in anogenital sites
SCCis also may arise in verrucae and condylomata
CLINICAL ISSUES
Site
Most common on head and neck region, other sun-exposed sites
Presentation
Scaly patch or plaque lesion
Ulceration and hemorrhage may be present
Treatment
Surgical approaches
Complete surgical excision is standard and definitive therapy
Mohs surgery often performed for facial lesions to minimize amount of tissue taken
Electrodessication and curettage (ED&C) may also be used
Drugs
Topical therapy with immunomodulators, including imiquimod or 5-fluorouracil, may be used
Patients with extensive lesions or poor surgical candidates
Prognosis
Excellent in most cases
Small risk for invasive squamous cell carcinoma
Greater risk in patients with immunosuppression or numerous lesions
MACROSCOPIC FEATURES
General Features
Broad, superficial lesion with epidermal thickening and overlying scale
MICROSCOPIC PATHOLOGY
Histologic Features
Atypical intraepidermal proliferation of squamous cells extending into upper levels of the epidermis
Basilar keratinocytes are often spared, leading to so-called “eyeliner” sign
Overlying parakeratosis often diffusely present, without skip areas over adnexal structures
Follicular epithelial involvement is typically seen
Cells are usually markedly enlarged and atypical appearing, with nuclear hyperchromasia and enlarged nucleoli
Numerous intraepidermal mitotic figures and apoptotic figures typically present
Cytologic Features
Enlarged cells with dense eosinophilic-staining cytoplasm, enlarged hyperchromatic-staining nuclei, and prominent nucleoli
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


