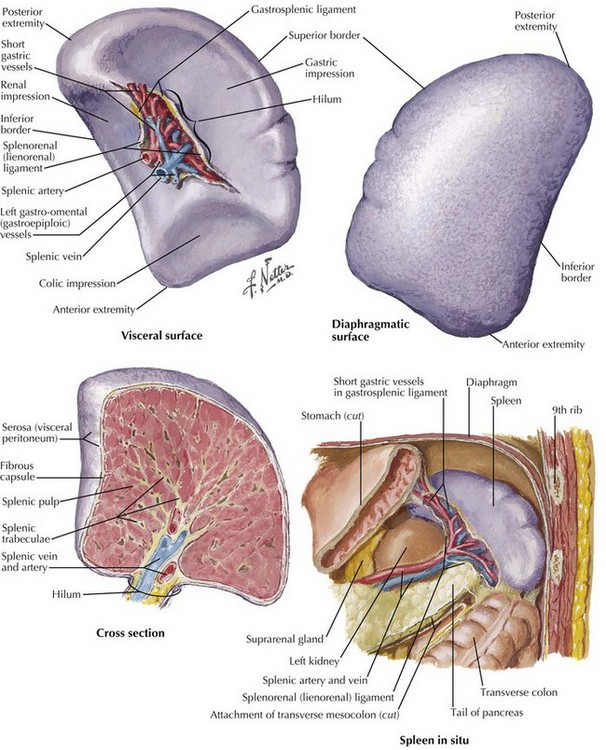
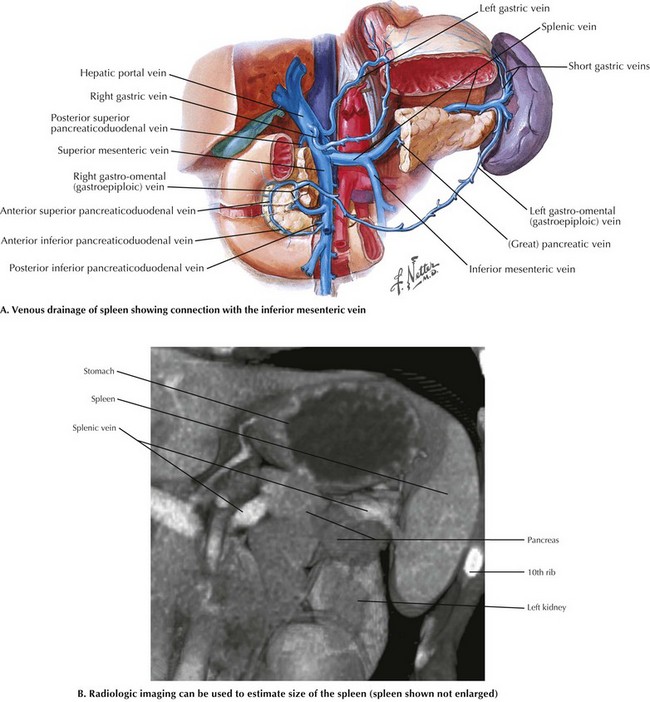
Chapter 17 The key to safe splenectomy is understanding the anatomy surrounding the spleen (Fig. 17-1). The spleen must be safely mobilized from all the surrounding structures to prevent common perioperative complications related to the splenic anatomy, including gastric injury or leak during division of short gastric vessels; pancreatitis or pancreatic fistula from the pancreatic tail during mobilization of the splenic hilum; colon injury during division splenic flexure; left pleural effusion or left pulmonary atelectasis from excessive diaphragm manipulation; and bleeding from short gastric vessels, splenic artery, or splenic vein. During the postoperative period, splenic vein thrombosis can lead to inferior mesenteric vein or portal vein thrombosis, with serious consequences (Fig. 17-2, A). The most serious long-term complication of splenectomy is sepsis, which can be decreased with preoperative immunization for the common encapsulated organisms, including meningococcal, pneumococcal, and Haemophilus influenzae type B infections, either 2 weeks before or on the last day of admission after surgery.
Splenectomy
Surgical Principles
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine