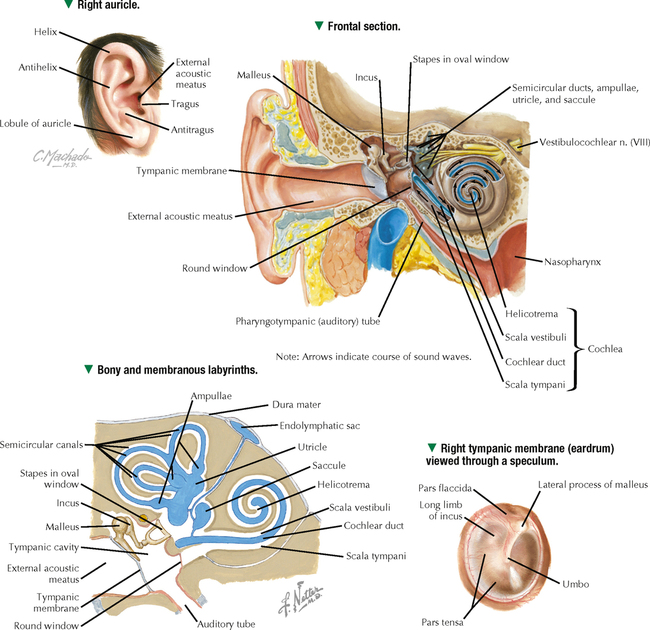
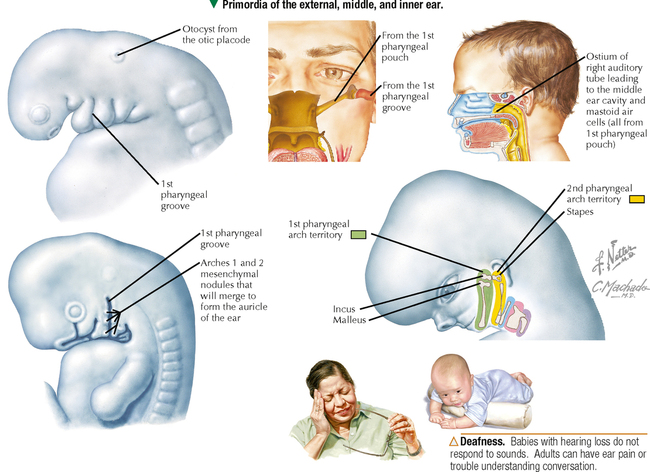
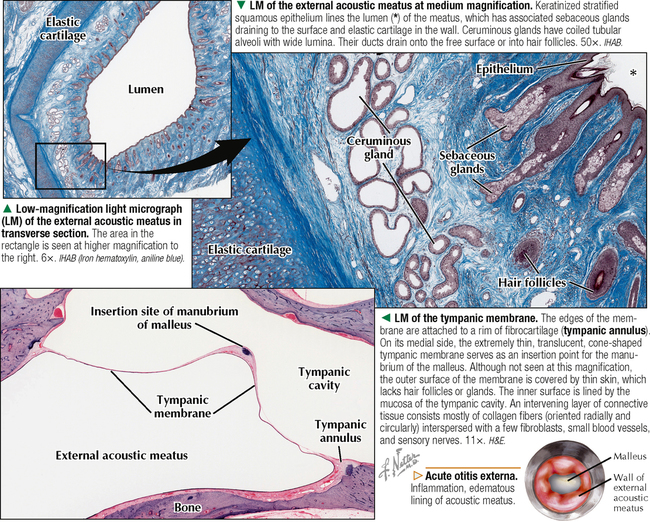
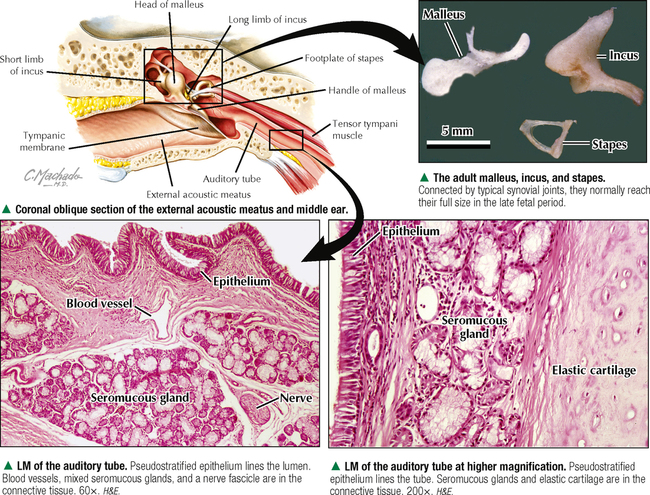
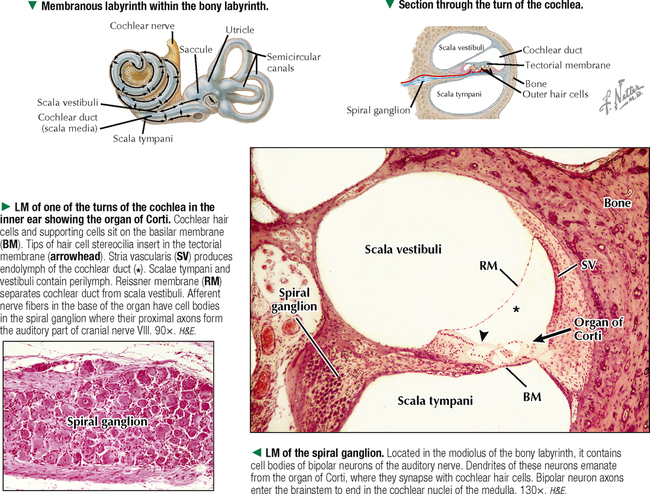
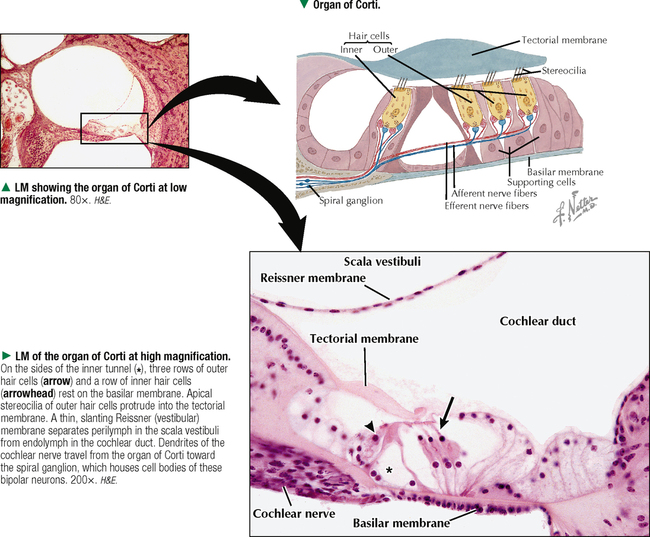
20 SPECIAL SENSES 20.1. Overview 20.2. Development of the Ear 20.3. Histology and Function of the External Acoustic Meatus 20.4. Histology and Function of the Middle Ear and Auditory Tube 20.5. Histology and Function of the Cochlea 20.6. Histology of the Organ of Corti 20.7. Ultrastructure and Function of Cochlear Hair Cells 20.8. Histology of Vestibular Receptors: Crista Ampullaris and Macula 20.9. Scanning Electron Microscopy of the Crista Ampullaris 20.10. Ultrastructure and Function of Vestibular Hair Cells 20.11. Histology and Function of Olfactory Mucosa 20.12. Scanning Electron Microscopy of Olfactory Epithelium 20.13. Structure and Distribution of Taste Buds 20.14. Histology and Function of Taste Buds 20.15. Ultrastructure of Taste Buds 20.16. Structure and Function of Cutaneous Sensory Receptors 20.17. Ultrastructure and Function of Merkel Cell–Neurite Complexes 20.18. Histology and Function of Meissner and Pacinian Corpuscles 20.19. Structure and Function of Interoceptors: Carotid Body and Sinus 20.20. Ultrastructure and Function of a Carotid Body 20.21. Histology and Function of Muscle Spindles 20.22. Ultrastructure and Function of Muscle Spindles 20.23. Innervation of Muscle Spindles 20.24. Ultrastructure and Function of Golgi Tendon Organs 20.1 OVERVIEW Sense organs include the ear, olfactory mucosa, taste buds, cutaneous receptors, interoceptors (monitor the internal environment), proprioceptors in muscles, tendons, and joints, and eye. Specialized receptor organs in ears sense hearing and balance. The ear has three parts: external, middle, and inner (labyrinth). The external ear, consisting of the auricle (pinna) and external acoustic meatus, conducts sound waves from the external environment to the tympanic membrane (eardrum). The middle ear (tympanic cavity) is an air-filled cavity in the petrous temporal bone that transforms sound waves into mechanical vibrations. Lined by a mucous membrane, it contains three auditory ossicles and communicates with the nasopharynx via the auditory (eustachian) tube. The inner ear has special receptors for hearing and maintenance of equilibrium. The bony labyrinth in the inner ear contains perilymph, which surrounds the endolymph-filled membranous labyrinth. The bony labyrinth—a series of communicating channels hollowed out in the petrous temporal bone—consists of a vestibule that houses the saccule, utricle, semicircular canals, and cochlea. The membranous labyrinth is lined by epithelium, which is modified in parts containing nerve endings. Specialized sensory areas are cristae ampullaris of the semicircular canals (detect angular acceleration), maculae of the utricle and saccule (respond mostly to gravity and linear movement of the head), and organ of Corti of the cochlea (responds to sound). Despite some differences, all three receptors conform to a similar histologic plan: receptor (sensory) hair cells, supporting cells, afferent nerve endings at the bases of hair cells connected to a ganglion, and a gelatinous glycoprotein coat in contact with endolymph and associated with “hairs” (stereocilia) of the hair cells. In the inner ear, vibrations are transduced by hair cells into specific nerve impulses via the vestibulocochlear cranial nerve (VIII). 20.2 DEVELOPMENT OF THE EAR The pharynx of the 4-week embryo shows several segmented lateral outpouchings called pharyngeal (or branchial) pouches, with intervening pharyngeal clefts (or grooves), which make the neck region look furrowed. The first pharyngeal cleft (between the first and second pouches) deepens and gives rise to the external acoustic meatus. The ectoderm of the first pharyngeal cleft grows inward and fuses with endoderm that lines the first pharyngeal pouch to form the tympanic membrane. At the same time, bilateral ectodermal thickenings—otic placodes—arise on the surface at the level of the hindbrain. Each placode invaginates, separates from the surface, and gives rise to a small saccule called the otocyst. With continued growth, it develops into the membranous labyrinth of the inner ear. Then, coiling of the otocyst, accompanied by a series of complex constrictions and outgrowths, gives rise to the saccule, utricle, three semicircular canals, and cochlea. The endolymphatic duct develops as a medial tubular outgrowth of the utricle. By the second trimester, the characteristic form and anatomic parts of the inner ear are established. Surrounding mesenchyme differentiates into hyaline cartilage, which is replaced via endochondral ossification to form the bony labyrinth. The three small middle ear ossicles (malleus, incus, and stapes) originate from cartilage of the first two pharyngeal pouches: the malleus and incus from cartilage of the first pouch; the stapes, from cartilage of the second pouch. Bone soon replaces cartilage, and the three ossicles form a chain united by small synovial joints. They will transmit vibrations from the tympanic membrane to the inner ear. Vibrations are then transmitted to the fluid-filled membranous labyrinth and then the organ of Corti, where hair cells are stimulated for sound reception. The tympanic cavity, auditory tube, and mastoid air cells arise from endoderm of the first pharyngeal pouch; the auricle, from mesenchyme of the first and second pharyngeal pouches. CLINICAL POINT The most serious ear disorders are those of the inner ear that lead to deafness. Congenital deafness may be acquired by intrauterine infection with neurotrophic viruses such as German measles (rubella) virus and cytomegalovirus or parasites such as Toxoplasma (toxoplasmosis). In congenital rubella syndrome, rubella virus affects the embryo, especially at 7–8 weeks, and causes atrophy or serious damage to the organ of Corti. Inherited congenital deafness disorders are usually autosomal recessive and lead to defective neural connections or faulty development of cochlear hair cells. 20.3 HISTOLOGY AND FUNCTION OF THE EXTERNAL ACOUSTIC MEATUS The external acoustic meatus, a resonator for sound, is an S-shaped tubular cul-de-sac about 2.5 cm long. The outer two thirds have elastic cartilage in the wall, which is continuous with that of the auricle. A thin layer of skin continuous with that of the epidermis of the auricle lines the meatus. Thin skin also lines the inner osseous part, which is a tunnel through temporal bone. It consists of keratinized stratified squamous epithelium and dense collagenous connective tissue of the dermis. Associated with the epithelium of the cartilaginous part are hair follicles, sebaceous glands, and ceruminous glands. Secretions from both glands contribute to yellowish earwax (cerumen). Ceruminous glands—branched, highly coiled tubuloalveolar glands—are modified apocrine sweat glands consisting of cuboidal secretory cells that face the glandular lumen and a deeper layer of myoepithelial cells. Gland excretory ducts open directly onto the skin surface or into a hair follicle. Lipid-rich cerumen has both hydrophobic and acidic properties to protect against pathogens and infection by stopping water from entering the skin and causing maceration. It also contains bacterial lysozyme. The external acoustic meatus keeps temperature and humidity relatively constant to protect the eardrum and preserve its elasticity. The tympanic membrane, which separates the external acoustic meatus from the tympanic cavity, takes the form of a flat cone with its tip facing medially. It is a thin layer of dense fibrous connective tissue covered externally by thin skin and internally by thin mucous membrane. It is supplied with small blood vessels and sensory nerve fibers, which reach the center of the membrane. CLINICAL POINT Acute otitis externa, commonly called swimmer’s ear, is inflammation, often with infection, of the external ear. The usual cause is infection with bacteria (Pseudomonas aeruginosa or Staphylococcus aureus) and less often fungus. Hot, humid climates; excessive moisture; and swimming in contaminated waters are predisposing factors. Because the epidermis of the external auditory meatus is richly innervated with sensory nerves, progressive inflammation and edema lead to mild or severe ear pain (otalgia), and blockage (stenosis) of this canal may lead to conductive deafness. Topical antibiotics and steroids are usual treatments. 20.4 HISTOLOGY AND FUNCTION OF THE MIDDLE EAR AND AUDITORY TUBE The middle ear is an air space in temporal bone that is lined by mucous membrane consisting of, in most areas, simple cuboidal epithelium. Its lateral wall is the tympanic membrane; its medial wall contains the vestibular (oval) and cochlear (round) windows. Three auditory ossicles extend across the tympanic cavity. The malleus is shaped like a hammer, and its handle directly attaches to the tympanic membrane. The malleus head articulates with the anvil-shaped incus, which, in turn, articulates with the stirrup-shaped stapes. The base (footplate) of the stapes transmits vibrations to the oval window. Two skeletal muscles insert into the ossicles in the middle ear and contract in response to sounds. The tensor tympani (innervated by cranial nerve V) inserts into the malleus handle and adjusts tympanic membrane tension. The stapedius (innervated by cranial nerve VII) attaches to the neck of the stapes and dampens its oscillatory vibrations. The auditory (eustachian) tube, 3–4 cm long, consists of bony and cartilagenous parts and connects tympanic cavity with nasopharynx. Most of its medial wall near the pharynx contains elastic cartilage, which is J-shaped in transverse section. Mostly pseudostratified ciliated columnar epithelium with goblet cells lines its lumen. As part of the mucociliary system of the middle ear, cilia beat synchronously toward the pharynx. The auditory tube is normally ventilated three or four times per minute, as it opens with swallowing, to allow equalization of pressure between the middle ear and pharynx. Impaired tube patency leads to relative negative pressure in the middle ear. Underlying connective tissue contains mixed seromucous glands and various amounts of lymphatic tissue. At the opening of the auditory tube with the pharynx, aggregates of lymphoid nodules form the tubal tonsil. CLINICAL POINT Otitis media is inflammation of the middle ear. Persistent, severe earache is an initial sign; hearing loss may occur. Common in young children, it is often caused by migration of pathogens or microorganisms from the nasopharynx to the middle ear via the auditory tube. It may also be due to an inflammatory process in the nasopharynx, allergy, hypertrophic adenoids, or benign or malignant tumors. Contributing is obstruction of the auditory tube by inflammation and mucosal edema. Dysfunction of this tube limits its ability to drain middle ear secretions. 20.5 HISTOLOGY AND FUNCTION OF THE COCHLEA The cochlea, a spiral canal shaped like a snail shell, is embedded in temporal bone. It forms 23/4 turns from base to apex, is 30–35 mm long, and has a lumen with three compartments: scala media (cochlear duct), scala vestibuli, and scala tympani. The cochlear duct is filled with endolymph; perilymph fills the other two scalae. The scalae vestibuli and tympani communicate through the helicotrema, a small opening at the cochlear apex. The cochlear duct is a triangular space in transverse section. Its lateral border makes up the stria vascularis—a richly vascularized pseudostratified epithelium that secretes endolymph. Reissner (vestibular) membrane, which marks the roof of the cochlear duct, consists of two layers of simple squamous epithelium and delineates cochlear duct from scala vestibuli. A thicker basilar membrane forms the floor of the cochlear duct and separates it from scala tympani. Superimposed on the basilar membrane is highly specialized epithelium—the organ of Corti—that consists of hair cells and supporting cells. Cochlear hair cells are specialized auditory receptor cells. They have apical stereocilia whose tips are embedded in the gelatinous tectorial membrane. Arising from the base of the organ of Corti are afferent nerve fibers that synapse with bases of hair cells. Nerve fibers converge toward the spiral ganglion, which contains cell bodies of neurons of the cochlear part of cranial nerve VIII. These bipolar neurons send axons to the brain’s auditory cortex. CLINICAL POINT Deafness (hearing loss), a common condition often related to advancing age, takes one of two forms. Conductive hearing loss is due to a lesion in the external auditory canal or middle ear; sensorineural hearing loss is caused by a lesion in the cochlea or cochlear division of cranial nerve VIII. To distinguish the two types clinically, hearing by air or bone conduction is tested via a vibrating tuning fork and audiometry. Presenting an acoustic stimulus in air tests for the conductive type. Placing a tuning fork in contact with the skull tests for the sensorineural type, which accounts for 90% of all cases of deafness. 20.6 HISTOLOGY OF THE ORGAN OF CORTI The organ of Corti in the cochlear duct is exquisitely designed for its role in auditory sensation. Lying on the basilar membrane, it is composed of hair cells, which have a complex organization, with several types of columnar supporting cells. Hair cells are arranged segmentally in two groups on the sides of an inner tunnel. A group of typically rounded inner hair cells is in one row; a group of outer hairs cells, usually more cylindrical, forms three rows. Ultrastructural criteria identify two different types of hair cells (I and II). Hair cells are polarized and bear apical stereocilia that project into the lumen of the endolymph-filled cochlear duct. Bases of hair cells are embedded in recesses formed by neighboring supporting cells that are rich in cytoskeletal components. Synapsing with these bases are afferent and efferent nerve terminals of cranial nerve VIII. Also, some supporting cells at the outer part of the organ of Corti produce the tectorial membrane, into which tips of stereocilia of the tallest outer hair cells project. The tectorial membrane, a gelatinous, resilient cuticular sheet that extends over hair cells, is made of glycoprotein in which are embedded 4-nm microfilaments Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading… Related Related posts: CARDIOVASCULAR SYSTEM RESPIRATORY SYSTEM THE CELL FEMALE REPRODUCTIVE SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Essential Histology Jun 18, 2016 | Posted by admin in HISTOLOGY | Comments Off on SPECIAL SENSES Full access? Get Clinical Tree
20 SPECIAL SENSES 20.1. Overview 20.2. Development of the Ear 20.3. Histology and Function of the External Acoustic Meatus 20.4. Histology and Function of the Middle Ear and Auditory Tube 20.5. Histology and Function of the Cochlea 20.6. Histology of the Organ of Corti 20.7. Ultrastructure and Function of Cochlear Hair Cells 20.8. Histology of Vestibular Receptors: Crista Ampullaris and Macula 20.9. Scanning Electron Microscopy of the Crista Ampullaris 20.10. Ultrastructure and Function of Vestibular Hair Cells 20.11. Histology and Function of Olfactory Mucosa 20.12. Scanning Electron Microscopy of Olfactory Epithelium 20.13. Structure and Distribution of Taste Buds 20.14. Histology and Function of Taste Buds 20.15. Ultrastructure of Taste Buds 20.16. Structure and Function of Cutaneous Sensory Receptors 20.17. Ultrastructure and Function of Merkel Cell–Neurite Complexes 20.18. Histology and Function of Meissner and Pacinian Corpuscles 20.19. Structure and Function of Interoceptors: Carotid Body and Sinus 20.20. Ultrastructure and Function of a Carotid Body 20.21. Histology and Function of Muscle Spindles 20.22. Ultrastructure and Function of Muscle Spindles 20.23. Innervation of Muscle Spindles 20.24. Ultrastructure and Function of Golgi Tendon Organs 20.1 OVERVIEW Sense organs include the ear, olfactory mucosa, taste buds, cutaneous receptors, interoceptors (monitor the internal environment), proprioceptors in muscles, tendons, and joints, and eye. Specialized receptor organs in ears sense hearing and balance. The ear has three parts: external, middle, and inner (labyrinth). The external ear, consisting of the auricle (pinna) and external acoustic meatus, conducts sound waves from the external environment to the tympanic membrane (eardrum). The middle ear (tympanic cavity) is an air-filled cavity in the petrous temporal bone that transforms sound waves into mechanical vibrations. Lined by a mucous membrane, it contains three auditory ossicles and communicates with the nasopharynx via the auditory (eustachian) tube. The inner ear has special receptors for hearing and maintenance of equilibrium. The bony labyrinth in the inner ear contains perilymph, which surrounds the endolymph-filled membranous labyrinth. The bony labyrinth—a series of communicating channels hollowed out in the petrous temporal bone—consists of a vestibule that houses the saccule, utricle, semicircular canals, and cochlea. The membranous labyrinth is lined by epithelium, which is modified in parts containing nerve endings. Specialized sensory areas are cristae ampullaris of the semicircular canals (detect angular acceleration), maculae of the utricle and saccule (respond mostly to gravity and linear movement of the head), and organ of Corti of the cochlea (responds to sound). Despite some differences, all three receptors conform to a similar histologic plan: receptor (sensory) hair cells, supporting cells, afferent nerve endings at the bases of hair cells connected to a ganglion, and a gelatinous glycoprotein coat in contact with endolymph and associated with “hairs” (stereocilia) of the hair cells. In the inner ear, vibrations are transduced by hair cells into specific nerve impulses via the vestibulocochlear cranial nerve (VIII). 20.2 DEVELOPMENT OF THE EAR The pharynx of the 4-week embryo shows several segmented lateral outpouchings called pharyngeal (or branchial) pouches, with intervening pharyngeal clefts (or grooves), which make the neck region look furrowed. The first pharyngeal cleft (between the first and second pouches) deepens and gives rise to the external acoustic meatus. The ectoderm of the first pharyngeal cleft grows inward and fuses with endoderm that lines the first pharyngeal pouch to form the tympanic membrane. At the same time, bilateral ectodermal thickenings—otic placodes—arise on the surface at the level of the hindbrain. Each placode invaginates, separates from the surface, and gives rise to a small saccule called the otocyst. With continued growth, it develops into the membranous labyrinth of the inner ear. Then, coiling of the otocyst, accompanied by a series of complex constrictions and outgrowths, gives rise to the saccule, utricle, three semicircular canals, and cochlea. The endolymphatic duct develops as a medial tubular outgrowth of the utricle. By the second trimester, the characteristic form and anatomic parts of the inner ear are established. Surrounding mesenchyme differentiates into hyaline cartilage, which is replaced via endochondral ossification to form the bony labyrinth. The three small middle ear ossicles (malleus, incus, and stapes) originate from cartilage of the first two pharyngeal pouches: the malleus and incus from cartilage of the first pouch; the stapes, from cartilage of the second pouch. Bone soon replaces cartilage, and the three ossicles form a chain united by small synovial joints. They will transmit vibrations from the tympanic membrane to the inner ear. Vibrations are then transmitted to the fluid-filled membranous labyrinth and then the organ of Corti, where hair cells are stimulated for sound reception. The tympanic cavity, auditory tube, and mastoid air cells arise from endoderm of the first pharyngeal pouch; the auricle, from mesenchyme of the first and second pharyngeal pouches. CLINICAL POINT The most serious ear disorders are those of the inner ear that lead to deafness. Congenital deafness may be acquired by intrauterine infection with neurotrophic viruses such as German measles (rubella) virus and cytomegalovirus or parasites such as Toxoplasma (toxoplasmosis). In congenital rubella syndrome, rubella virus affects the embryo, especially at 7–8 weeks, and causes atrophy or serious damage to the organ of Corti. Inherited congenital deafness disorders are usually autosomal recessive and lead to defective neural connections or faulty development of cochlear hair cells. 20.3 HISTOLOGY AND FUNCTION OF THE EXTERNAL ACOUSTIC MEATUS The external acoustic meatus, a resonator for sound, is an S-shaped tubular cul-de-sac about 2.5 cm long. The outer two thirds have elastic cartilage in the wall, which is continuous with that of the auricle. A thin layer of skin continuous with that of the epidermis of the auricle lines the meatus. Thin skin also lines the inner osseous part, which is a tunnel through temporal bone. It consists of keratinized stratified squamous epithelium and dense collagenous connective tissue of the dermis. Associated with the epithelium of the cartilaginous part are hair follicles, sebaceous glands, and ceruminous glands. Secretions from both glands contribute to yellowish earwax (cerumen). Ceruminous glands—branched, highly coiled tubuloalveolar glands—are modified apocrine sweat glands consisting of cuboidal secretory cells that face the glandular lumen and a deeper layer of myoepithelial cells. Gland excretory ducts open directly onto the skin surface or into a hair follicle. Lipid-rich cerumen has both hydrophobic and acidic properties to protect against pathogens and infection by stopping water from entering the skin and causing maceration. It also contains bacterial lysozyme. The external acoustic meatus keeps temperature and humidity relatively constant to protect the eardrum and preserve its elasticity. The tympanic membrane, which separates the external acoustic meatus from the tympanic cavity, takes the form of a flat cone with its tip facing medially. It is a thin layer of dense fibrous connective tissue covered externally by thin skin and internally by thin mucous membrane. It is supplied with small blood vessels and sensory nerve fibers, which reach the center of the membrane. CLINICAL POINT Acute otitis externa, commonly called swimmer’s ear, is inflammation, often with infection, of the external ear. The usual cause is infection with bacteria (Pseudomonas aeruginosa or Staphylococcus aureus) and less often fungus. Hot, humid climates; excessive moisture; and swimming in contaminated waters are predisposing factors. Because the epidermis of the external auditory meatus is richly innervated with sensory nerves, progressive inflammation and edema lead to mild or severe ear pain (otalgia), and blockage (stenosis) of this canal may lead to conductive deafness. Topical antibiotics and steroids are usual treatments. 20.4 HISTOLOGY AND FUNCTION OF THE MIDDLE EAR AND AUDITORY TUBE The middle ear is an air space in temporal bone that is lined by mucous membrane consisting of, in most areas, simple cuboidal epithelium. Its lateral wall is the tympanic membrane; its medial wall contains the vestibular (oval) and cochlear (round) windows. Three auditory ossicles extend across the tympanic cavity. The malleus is shaped like a hammer, and its handle directly attaches to the tympanic membrane. The malleus head articulates with the anvil-shaped incus, which, in turn, articulates with the stirrup-shaped stapes. The base (footplate) of the stapes transmits vibrations to the oval window. Two skeletal muscles insert into the ossicles in the middle ear and contract in response to sounds. The tensor tympani (innervated by cranial nerve V) inserts into the malleus handle and adjusts tympanic membrane tension. The stapedius (innervated by cranial nerve VII) attaches to the neck of the stapes and dampens its oscillatory vibrations. The auditory (eustachian) tube, 3–4 cm long, consists of bony and cartilagenous parts and connects tympanic cavity with nasopharynx. Most of its medial wall near the pharynx contains elastic cartilage, which is J-shaped in transverse section. Mostly pseudostratified ciliated columnar epithelium with goblet cells lines its lumen. As part of the mucociliary system of the middle ear, cilia beat synchronously toward the pharynx. The auditory tube is normally ventilated three or four times per minute, as it opens with swallowing, to allow equalization of pressure between the middle ear and pharynx. Impaired tube patency leads to relative negative pressure in the middle ear. Underlying connective tissue contains mixed seromucous glands and various amounts of lymphatic tissue. At the opening of the auditory tube with the pharynx, aggregates of lymphoid nodules form the tubal tonsil. CLINICAL POINT Otitis media is inflammation of the middle ear. Persistent, severe earache is an initial sign; hearing loss may occur. Common in young children, it is often caused by migration of pathogens or microorganisms from the nasopharynx to the middle ear via the auditory tube. It may also be due to an inflammatory process in the nasopharynx, allergy, hypertrophic adenoids, or benign or malignant tumors. Contributing is obstruction of the auditory tube by inflammation and mucosal edema. Dysfunction of this tube limits its ability to drain middle ear secretions. 20.5 HISTOLOGY AND FUNCTION OF THE COCHLEA The cochlea, a spiral canal shaped like a snail shell, is embedded in temporal bone. It forms 23/4 turns from base to apex, is 30–35 mm long, and has a lumen with three compartments: scala media (cochlear duct), scala vestibuli, and scala tympani. The cochlear duct is filled with endolymph; perilymph fills the other two scalae. The scalae vestibuli and tympani communicate through the helicotrema, a small opening at the cochlear apex. The cochlear duct is a triangular space in transverse section. Its lateral border makes up the stria vascularis—a richly vascularized pseudostratified epithelium that secretes endolymph. Reissner (vestibular) membrane, which marks the roof of the cochlear duct, consists of two layers of simple squamous epithelium and delineates cochlear duct from scala vestibuli. A thicker basilar membrane forms the floor of the cochlear duct and separates it from scala tympani. Superimposed on the basilar membrane is highly specialized epithelium—the organ of Corti—that consists of hair cells and supporting cells. Cochlear hair cells are specialized auditory receptor cells. They have apical stereocilia whose tips are embedded in the gelatinous tectorial membrane. Arising from the base of the organ of Corti are afferent nerve fibers that synapse with bases of hair cells. Nerve fibers converge toward the spiral ganglion, which contains cell bodies of neurons of the cochlear part of cranial nerve VIII. These bipolar neurons send axons to the brain’s auditory cortex. CLINICAL POINT Deafness (hearing loss), a common condition often related to advancing age, takes one of two forms. Conductive hearing loss is due to a lesion in the external auditory canal or middle ear; sensorineural hearing loss is caused by a lesion in the cochlea or cochlear division of cranial nerve VIII. To distinguish the two types clinically, hearing by air or bone conduction is tested via a vibrating tuning fork and audiometry. Presenting an acoustic stimulus in air tests for the conductive type. Placing a tuning fork in contact with the skull tests for the sensorineural type, which accounts for 90% of all cases of deafness. 20.6 HISTOLOGY OF THE ORGAN OF CORTI The organ of Corti in the cochlear duct is exquisitely designed for its role in auditory sensation. Lying on the basilar membrane, it is composed of hair cells, which have a complex organization, with several types of columnar supporting cells. Hair cells are arranged segmentally in two groups on the sides of an inner tunnel. A group of typically rounded inner hair cells is in one row; a group of outer hairs cells, usually more cylindrical, forms three rows. Ultrastructural criteria identify two different types of hair cells (I and II). Hair cells are polarized and bear apical stereocilia that project into the lumen of the endolymph-filled cochlear duct. Bases of hair cells are embedded in recesses formed by neighboring supporting cells that are rich in cytoskeletal components. Synapsing with these bases are afferent and efferent nerve terminals of cranial nerve VIII. Also, some supporting cells at the outer part of the organ of Corti produce the tectorial membrane, into which tips of stereocilia of the tallest outer hair cells project. The tectorial membrane, a gelatinous, resilient cuticular sheet that extends over hair cells, is made of glycoprotein in which are embedded 4-nm microfilaments Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading… Related Related posts: CARDIOVASCULAR SYSTEM RESPIRATORY SYSTEM THE CELL FEMALE REPRODUCTIVE SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Essential Histology Jun 18, 2016 | Posted by admin in HISTOLOGY | Comments Off on SPECIAL SENSES Full access? Get Clinical Tree