103
CHAPTER OUTLINE
Medical office visits are ideal for early identification of drug and alcohol use by adolescents because they provide opportunities for a medical professional to interview teenagers in a private and confidential setting. Several professional societies recommend that all adolescents be screened for drug and alcohol use at every primary care visit (1–3). There are several goals for such screening: (a) to determine whether a teen has ever used alcohol or drugs; (b) to determine whether teens who have used alcohol or drugs are at low risk or high risk for developing substance use disorders; (c) to give pertinent health advice to teens who are at risk of acute consequences of alcohol or other drug use as well as to give positive feedback to teens who have never used; and (d) to refer teens who are at high risk of long-term consequences of substance use to the appropriate level of intervention. These goals can be summarized as screening, brief intervention, and referral to treatment. Providers often note many barriers to screening appropriately in the office setting; the two most common concerns were a lack of time and lack of training to manage a positive screen appropriately (4). This chapter describes screening procedures and tools that can be used in primary care to quickly and accurately determine the risk level, brief interventions that can be implemented with teens in different risk categories, and strategies that encourage teens to follow-up when referral for more intensive services is required.
SCREENING FOR USE
Clinicians should begin asking adolescents about substance use and other sensitive questions as soon as the young person is old enough to be interviewed without the parent present. The exact age will vary from patient to patient, falling between 11 and 13 years for most adolescents. However, the National Institute on Alcohol Abuse and Alcoholism recommends screening children as low as age 9 years as one in three adolescents began drinking before the age of 13 (5). After meeting with the parent and patient together and reviewing the ground rules of confidentiality, the clinician should ask the parent to leave the room in order to ask the adolescent personal questions. In addition, the clinician should emphasize that the details discussed will remain confidential unless he or she has safety concerns about the patient or others. Determining whether a reported behavior reaches the level of a safety concern is a matter of clinical judgment. (see Chapter 109, “Ethical Issues in Addiction Practice,” which discusses confidentiality in greater detail). Reassure the adolescent that in the instance that it is necessary to inform a parent of safety issue, the clinician will notify him or her of the disclosure prior to telling a parent, so the patient does not feel blindsided or betrayed.
The Home, Education, Activities/Alcohol, Drugs, Sex, Suicidality (HEADSS) psychosocial interview for adolescents includes questions about alcohol and drug use in the context of a more extensive psychosocial history (6), allowing the interviewer to develop rapport with the adolescent prior to asking more personal questions. The Strengths, School, Home, Activities, Drugs, Emotions, Sex, Safety (SSHADESS) screen is similar to the HEADSS screen but goes further, allowing a clinician to identify the patient’s strengths at the start of the interview to help increase the young person’s comfort level (7). When asking about drugs and alcohol (the “D” in HEADSS or SSHADESS), the interviewer should ask three straightforward questions: (a) “Have you ever drunk alcohol (more than a few sips)?” (b) “Have you ever smoked marijuana?” (c) “Have you ever used anything else to get high, including illicit drugs (like cocaine, heroin, or methamphetamine); medications that were not prescribed to you or used in a way other than ordered by a doctor; over-the-counter medications; or inhalant chemicals?” For younger children, it may be helpful to begin with a very simple question about friends’ use (“Do you have any friends who have drunk alcohol or used drugs in the past year?”) prior to initiating the introductory questions above (8).
To maximize the sensitivity of the question, the interviewer should begin the question with “Have you ever…”; however, if the patient is well known to the interviewer or if this is a repeat screening, the interviewer may choose to begin with “Since your last appointment with me…” The interviewer should avoid ambiguous questions, such as “Do you drink/smoke?” as answers to these questions may be interpreted differently by the patient and clinician.
Adolescents who report complete abstinence from alcohol and drugs should be given praise and encouragement regarding the good decisions they have made. Any adolescent who reports having used alcohol or drugs should be further screened with a developmentally appropriate screening tool.
SCREENING FOR RISKS AND PROBLEMS
A screening is an assessment applied to populations that intends to identify individuals at risk for a particular condition. Several tools have been developed to screen patients for high-risk use of alcohol and other drugs. In general, these tools fall into two broad categories: written assessments (such as the AUDIT [Alcohol Use Disorders Identification Test] (9) and POSIT [Problem Oriented Screening Instrument for Teenagers] (10)) and oral screens (such as the CRAFFT (11) and CAGE (12)). Written tools have a number of potential advantages—they can be self-administered and completed in a waiting room before the patient is seen by the clinician, and they often screen for several disorders simultaneously, including mental health, behavioral, and substance use disorders. Both the AUDIT and the POSIT have been well studied and have excellent psychometric properties for screening adolescents (13–15). However, there are also disadvantages to written assessments—patients must have an adequate reading level in order to complete the screen, and screens should be completed in privacy, which is often not possible in a busy waiting room. These assessments also require training and time in order to score and interpret properly.
Oral screens are generally composed of a few questions that an interviewer can ask quickly. The CAGE questions are a popular screen for alcohol disorders and have been shown to have good psychometric properties for identifying alcoholism among middle-aged men (16). Unfortunately, this screen is not good for identifying hazardous drinking (17,18), nor is it valid for screening teenagers. Some research has shown that these questions are not developmentally appropriate for adolescents, and their sensitivity is low for identifying high-risk alcohol use among adolescents (14).
The CRAFFT screen is a series of six questions developed to screen adolescents for alcohol and other drug use disorders simultaneously. CRAFFT is a mnemonic acronym. During the past 12 months, have you ever (a) ridden in a car driven by someone, including yourself, who was high or had been using alcohol or drugs? (b) used alcohol or drugs to relax, feel better about yourself, or fit in? (c) used alcohol or drugs while you are by yourself, alone? (d) forgotten things you did while using alcohol or drugs? (e) had your family or friends tell you that you should cut down on your drinking or drug use? (f) gotten into trouble while you were using alcohol or drugs? (19).
Each “yes” response is scored 1 point. A score of 2 or greater is a positive screen and indicates that the adolescent is at high risk for having an alcohol- or drug-related disorder (20).
Recent studies have shown that adolescents prefer non-interactive CRAFFT screening with paper questionnaires to being interviewed by a clinician (either a nurse or a physician) (21). Patients reported increased honesty in answering when not directly confronted face to face. The same study demonstrated that screening via computer was statistically tied with paper screening regarding patients’ likelihood of being honest when answering substance abuse screening questions. Current active research is focusing more closely on using electronic mechanisms such as computers or tablets to facilitate screening (22).
Regardless of mechanism, all adolescents who have used alcohol or another drug should be asked the CRAFFT questions or should be screened with an alternative formal screening tool. Past research has demonstrated that even experienced adolescent medicine specialists significantly underestimate adolescents’ risk level when relying on clinical impressions alone (23). Additionally, even adolescents who report abstinence from alcohol and drugs should be asked whether they have ever ridden in a car with a driver who was high or had used alcohol or drugs. After completing the opening questions regarding alcohol and drug use and the follow-up screen, the clinician can determine the appropriate next step.
SCREEN-SPECIFIC STRATEGIES
Physician Brief Advice
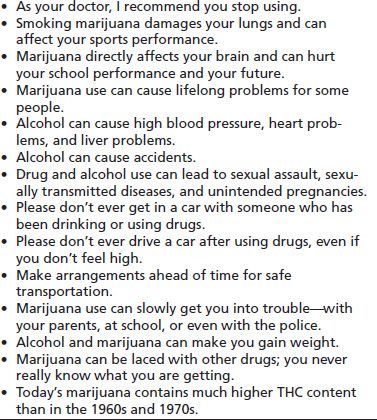
Brief advice is a 2- to 3-minute statement from the provider that reinforces the choice of the adolescent who is not actively using alcohol or drugs by conveying that use can be harmful. Examples of brief advice statements are provided in Table 103-1. Brief intervention goes further and may include elements such as motivational interviewing and creation of an abstinence challenge to deter use; these are discussed in detail later in this chapter. Brief intervention has been shown to reduce or stabilize risk, decrease drinking rates among college students, and decrease substance abuse rates in the 14- to 18-year-old age group (24,25).
TABLE 103-1 BRIEF ADVISE SAMPLE STATEMENTS
No Use: Praise and Encouragement
Lisa is a 14-year-old girl who presents for her annual physical examination before the start of soccer season. On her CRAFFT screen, she answers “No” to all of the opening questions and “No” to the Car question. Adolescents who have been abstinent from alcohol and drugs and who have never ridden with an intoxicated driver should receive praise and encouragement from their clinicians. Adolescents should be encouraged to discuss drug use or ask questions in the future should the need arise. Statements such as “It sounds as if you have made smart choices by not using drugs or alcohol. If that ever changes, I hope you will feel comfortable enough to talk to me about it” aim both to praise the young person’s abstinence and to avail the opportunity for open communication in the future.
Physician Assessment
Medium Risk: No Use/Car +
Rob is a 17-year-old male about to begin his last year of high school. He takes all honors and advance placement classes and plans to apply to very competitive colleges. He uses neither alcohol nor drugs himself, but once got a ride home from a friend who had been drinking. All adolescents who have ridden with an intoxicated driver should receive risk reduction advice. The “Contract for Life” (26) is a document developed by Students Against Destructive Decisions (SADD) that asks adolescents to commit to never ride with a driver who has been drinking or using other drugs and also asks parents to promise to provide transportation home without any questions if their child is in need. The clinician should explain that the intention of the document is to ensure that the adolescent always has safe transport home and not to avoid conversation between parents and their children. Parents should be encouraged both to praise their children for avoiding riding with an intoxicated driver and to explore the events of such an evening at a later time—when neither the adolescent nor the parent is intoxicated or angry—with open-ended questions, such as “How did you end up in this situation?” and “How can you avoid this situation in the future?” Rob is encouraged to take the contract home to discuss with his parents. You ask him to make a follow-up appointment to discuss how it went.
Medium Risk: +Use/−Car/CRAFFT Negative
Marcus is an 18-year-old who presents to the office after injuring his ankle during football practice. You decide to screen him for substance use. He reports that he has gotten high on marijuana on several occasions, but not at the time of this injury. He has never used any other drugs and his CRAFFT score is 1; he will sometimes use to relax or fit in with his friends. Adolescents who report alcohol or other drug use but screen negative (i.e., 0 or 1 on the CRAFFT) are at relatively low risk for meeting the criteria for a substance use disorder. These teens should receive brief advice to stop using, such as “My advice is for you to stop using alcohol or drugs at all, because they pose a serious risk to your health.” The clinician should also give specific information related to the health effects of the drug that the teen is using. Any knowledge of the patient’s health concerns can be used to target the information. For example, an overweight adolescent who is drinking alcohol might benefit from information regarding the calorie content of beer or mixed drinks. Adolescents who participate in sports will frequently report decreased use of marijuana during the sports season and can be educated about the specific effects of marijuana on the lungs. A sample of brief advice statements is presented in Table 103-1. The clinician should challenge the patient to a time-limited trial of abstinence (e.g., 1 week to 3 months) and ask him or her to come for a return visit to discuss how it went.
High Risk: CRAFFT 2 or Above
Katie is a 16-year-old girl who comes in for her annual physical exam. On screening, she reports that she drinks alcohol and uses marijuana every few weeks or so but has never used any other drugs. She gives positive answers to the Relax, Family, and Trouble questions, so her CRAFFT score = 3. Adolescents who screen positive (i.e., CRAFFT score of 2 or more) are at high risk of having a substance use disorder and need further assessment. Clinicians who screen adolescents for substance use should be prepared to perform a limited assessment in order to triage referrals for these patients. A brief assessment should begin with assessing the patient for acute risk of harm to themselves or others. These may include consuming potentially lethal amounts of alcohol (e.g., more than 10 drinks per occasion) or driving while intoxicated. Clinicians may need to break confidentiality if there is ongoing acute danger. If there is time during the visit, the clinician should perform a more detailed interview of the patient, paying particular attention to family issues such as divorce or parental separation, domestic violence and abuse, and family members’ substance use. Referrals to individual and/or family therapy should be considered to treat these and other underlying problems that are likely contributors to the substance use. For patients who are not drug dependent, it may be appropriate to make a statement such as “Your CRAFFT score indicates that you are at high risk. I am very worried about you. I’d like you to make an appointment for next week so we can continue to discuss this.” Ask the patient to agree to no alcohol or drug use until the return visit, but clarify this statement with “Even if you do use, I would still like for you to follow up next week. We can discuss why it was so difficult for you to abstain.”
Strategies for Interviewing Adolescents
For any patient, a nonjudgmental, empathetic interviewing style that accepts the patient’s point of view encourages more information sharing than an interrogative style. The interviewer should use open-ended questions to begin the conversation, with an emphasis on the pattern of drug use over time, including whether drug use has increased in quantity or frequency, whether the teen has made attempts at discontinuing drug use, and why and whether attempts have been successful. Information about the pattern of drug use and associated problems is more important in making a diagnosis of a substance-related disorder than the absolute quantity or frequency. At times, cues from the clinician may help the adolescent make connections between drug use and consequences. For example, statements such as “It seems that your grades started to fall at the same time that you started using more marijuana” may help the adolescent associate the two occurrences. A well-conducted history has therapeutic value as it encourages the adolescent to consider the consequences of drug use that she or he has already experienced.
Substance Use History
Substance of Choice
The substance use history should start with the substance of choice. The clinician should begin with an open-ended question, such as “Tell me about your history of alcohol use.” Cue adolescents to discuss general trends in their substance use (“Has your use been increasing over time?”), and get an estimate of the current level of use (“About how often do you use now?”). For alcohol, ask adolescents how many drinks it takes to get drunk, as a high tolerance for alcohol consumption without feeling drunk may be a signal that the adolescent is genetically susceptible to developing alcohol use disorders, particularly if the family history is positive for alcoholism (27). Also, ask whether they have ever had a blackout (“Have you ever drunk so much alcohol that you could not remember anything, even though you were walking and talking?”) as these events indicate significant alcohol intake but may not be considered problematic by some adolescents.
The clinician should ask whether adolescents have had any problems related to their use of substances. Many teens do not connect problems they have experienced with substance use, and cueing by the clinician may be helpful. If the teen denies experiencing problems, the clinician should ask specifically about tension with parents, school problems, decrease in grades or sports performance, suspensions or expulsions from school or sports teams, physical fights, arguments with friends while intoxicated, medical problems (i.e., overdose or getting sick), unwanted sexual contact, or legal problems/arrests. Stating questions such as “Some kids say that they feel they could have done better in school if they were not using marijuana. Have you ever felt that way?” may help to draw a connection between substance use and its consequences in a nonthreatening manner. The clinician should also ask patients whether they have ever tried to quit, and if so, why. Adolescents’ reasons for previous quitting attempts provide insight into perceived negative consequences of substance abuse and can be very helpful in personalizing advice.
Review of Other Substances
After completing the history for the substance of choice, the clinician should review whether the adolescent has used other substances. If the substance of choice is not alcohol or marijuana, the clinician should ask detailed questions (as earlier) about these substances, as it is unusual for an adolescent to have used other illicit drugs without ever using alcohol or marijuana. However, recently, it has become common for teens to misuse prescription (such as narcotics, benzodiazepines, or stimulants) or over-the-counter medications without previous history of alcohol or marijuana use (28). Clinicians should also ask adolescents whether they have used any other substances to get high, whether they have been a regular user, and whether they have had problems related to use.
Collateral History
At times, substance use by an adolescent will present to a clinician as a report by a parent, from a school, or from another adult. In these cases, the clinician should take a careful collateral history.
If a parent suspects drug use but the child denies using substances, the clinician should have the parent carefully list his or her observations. Substance use often presents with nonspecific complaints, such as staying out late, moodiness, breaking house rules, drop in grades, loss of interest in hobbies, or developing a new group of friends, and these symptoms should always be investigated further, particularly if more than one is present. Lying, stealing, appearing intoxicated, or possessing drugs or paraphernalia are more specific signs of drug use and should raise suspicion whenever present. In some cases, parents will report having caught their child using alcohol or other drugs. In these circumstances, the clinician should ask how the parent approached the child and the child’s response. Parent responses to these questions demonstrate the family’s attitudes toward drug use and may provide an opportunity for guidance.
As part of a collateral history, the clinician should also ask the parents their impression of the frequency of substance use. Adolescents work hard to hide drug use from their parents and, as a result, parents almost always significantly underestimate the frequency of their child’s drug use (29). Nonetheless, parents’ observations and impressions provide a useful piece of clinical information. In addition, the clinician should also ask whether the parents have concerns about other drugs. Occasionally, the parents will report prescriptions disappearing from the medicine cabinet or finding needles or other paraphernalia in the house. Any such reports should be further explored with the adolescent.
If consent is properly obtained, it is often useful to get additional history from patients’ significant others, siblings or other extended family, teachers and other school administrators, and any mental health providers who may already be involved with the adolescent.
Physical Exam
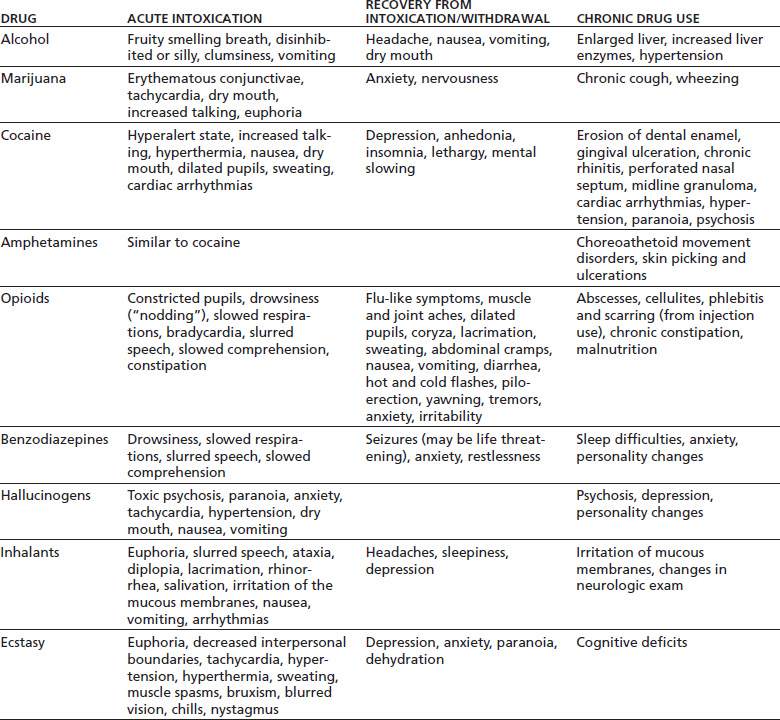
Adolescents who have a positive screen for high-risk substance use should have a physical exam to look for signs of acute intoxication or chronic drug use. Signs of chronic drug use are rare in teens but should be both discussed with the adolescent and recorded in the chart if present. A list of several signs associated with acute intoxication, withdrawal, and chronic drug use is presented in Table 103-2.
TABLE 103-2 SIGNS OF DRUG INTOXICATION, RECOVERY FROM INTOXICATION, AND CHRONIC USE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


