Sarcomatoid Carcinoma, Prostate
Gladell P. Paner, MD
Key Facts
Terminology
Malignant biphasic or monophasic neoplasm of prostate demonstrating epithelial and mesenchymal differentiation by LM/IHC
Rationale for considering SC and CS as single entity is due to similar clinicopathologic features and poor prognosis
Clinical Issues
Rare; only about 100 cases described in literature
Microscopic Pathology
Overall histology falls into 3 categories
Carcinoma admixed with sarcomatoid spindle cell component (most common)
Carcinoma admixed with sarcomatous component containing heterologous elements
Monophasic spindle cell tumor with immunohistochemical &/or electron microscopic evidence of epithelial differentiation
Acinar adenocarcinoma pattern most common
Sarcomatoid component frequently composed of hypercellular high-grade spindle cells (undifferentiated spindle cell sarcoma)
Heterologous elements present in 24% of cases, most commonly osteosarcoma
Carcinoma typically PSA/PAP(+)
Spindle cells at least focally (+) for at least 1 epithelial marker
Top Differential Diagnoses
Primary sarcomas of prostate
Pseudosarcomatous myofibroblastic proliferation of prostate
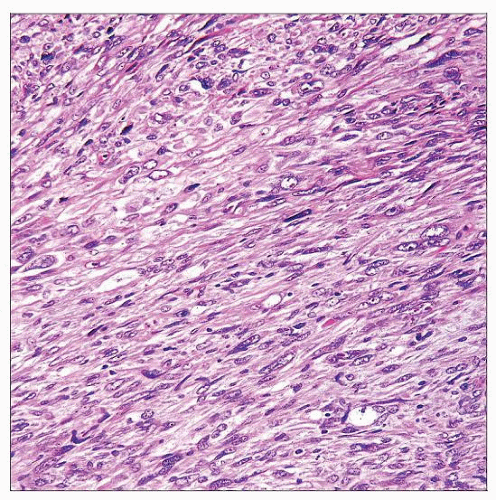 Monophasic malignant spindle cell tumor is shown involving the prostate. Other areas of this neoplasm showed typical high-grade adenocarcinoma of the prostate with acinar histology. |
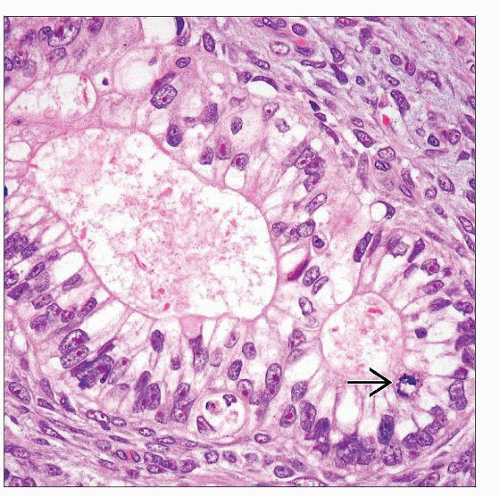 Acinar adenocarcinomatous component of SC shows prominent nucleoli, mitoses  , and absence of basal cell layer. Spindle cells surrounding the glands have malignant features. , and absence of basal cell layer. Spindle cells surrounding the glands have malignant features. |
TERMINOLOGY
Abbreviations
Sarcomatoid carcinoma (SC)
Carcinosarcoma (CS)
Definitions
Malignant biphasic or monophasic neoplasm of prostate, demonstrating epithelial and mesenchymal differentiation by light microscopy or immunohistochemistry
CS is employed by some authors for tumors with heterologous sarcomatous elements
Rationale for considering SC and CS as single entity is due to similar clinicopathologic features and poor prognosis
ETIOLOGY/PATHOGENESIS
Origin
Sarcomatoid dedifferentiation in prostatic carcinoma
High proportion of SCs have prior diagnosis of prostate adenocarcinoma
Focal immunohistochemical expression of PSA &/or PAP is demonstrated in spindle cells
Even with heterologous elements present, spindle cells often express keratin or p63 suggesting common origin with carcinomatous component
Loss-of-heterozygosity studies show that carcinomatous and sarcomatoid components are clonally related
Possible collision of epithelial and mesenchymal malignant tumors less accepted
Risk Factors
Prior diagnosis of prostate adenocarcinoma in almost 1/2 of cases
Radiotherapy &/or hormonal therapy for prostate carcinoma may play role in SC development
CLINICAL ISSUES
Epidemiology
Incidence
Rare
Only ˜ 100 cases described in literature
Age
Mean: 70 years, range: 43-91 years
Presentation
Majority present with obstructive urinary symptoms or metastatic disease
Uncommonly, tumors are detected in patients with elevated serum PSA level or palpable nodule on digital rectal examination (DRE)
Laboratory Tests
PSA serum level may be normal or elevated
Natural History
Prior history of prostate adenocarcinoma seen in 48-66%
Time interval from prostate adenocarcinoma to diagnosis of SC range from 6 months to 16 years (mean: 6.8 years)
About 1/3 of cases arises de novo with no prior history of prostate adenocarcinoma and radiation &/or hormonal therapy
Treatment
Current therapies, including multimodality approach, are ineffective, as tumor is high grade
Prognosis
Poor outcome
Aggressive clinical course characterized by local recurrences and metastasis
1 study reports 5-year cancer specific survival of 41% and 7-year survival of 14%
Another study reports actuarial risk of death at 1 year of 20% after diagnosis of SC
Systemic metastases in majority of patients are to lungs and bone
Other reported sites include brain, lymph node, liver, peritoneum, and skin
MACROSCOPIC FEATURES
General Features
Most tumors are encountered in transurethral resection of prostate (TURP) specimens for obstructive urinary symptoms
Large gray-white to yellow-tan with prominent necrosis, hemorrhage, and infiltrative growth
Tumors extend extraparenchymally into periprostatic soft tissues or adjacent organs, such as seminal vesicles and urinary bladder
MICROSCOPIC PATHOLOGY
Histologic Features
Carcinomatous and sarcomatoid components are intimately admixed
Overall histology falls into 3 categories
Carcinoma admixed with sarcomatoid spindle cell component (most common)
Carcinoma admixed with sarcomatous component containing heterologous elements
Monophasic spindle cell tumor with immunohistochemical &/or electron microscopic evidence of epithelial differentiation
Proportion of components vary, and sarcomatoid elements may range from 5-99% of tumor
Florid sarcomatoid overgrowth may be mistaken as pure sarcoma of prostate
Carcinomatous component
Variable and may be admixture of the following patterns
Acinar adenocarcinoma
Most frequent epithelial pattern
Often are high grade (Gleason score 8-10)
Typical patterns, such as glandular, cribriform, comedo, and solid, may be seen
Uncommon prostate adenocarcinoma pattern
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


