Sarcoid Lymphadenopathy
Sa A. Wang, MD
Key Facts
Terminology
Multisystemic chronic granulomatous disease
Etiology/Pathogenesis
Unknown
Clinical Issues
Multisystem involvement
Therapy may not be required if asymptomatic
Prognosis depends on involvement of critical organs
Image Findings
Bilateral hilar lymphadenopathy, many with lung nodules, PET active
Microscopic Pathology
“Hard” granulomas without acute inflammation or necrosis
No specific cause identified
Foci of fibrosis can be associated with granulomas
Ancillary Tests
Serum angiotensin converting enzyme (ACE)
Bronchoalveolar lavage fluid for CD4:CD8 ratio
CD4:CD8 > 4:1
Impaired pulmonary function
Top Differential Diagnoses
Tuberculosis
Atypical mycobacteria
Fungal lymphadenitis
Diagnostic Checklist
Compatible clinical and radiographic manifestations
Biopsy shows granulomatous lymphadenitis without identifiable causative agents
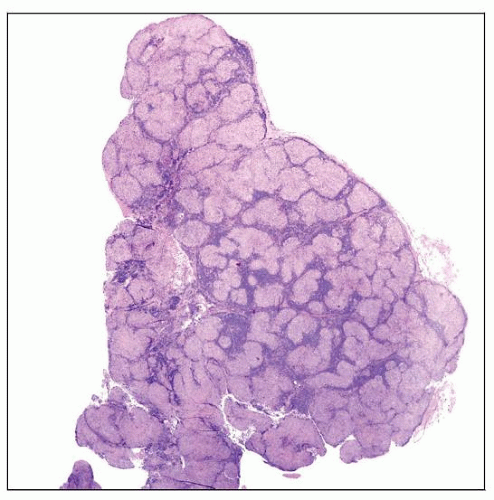 The lymph node parenchyma is substantially effaced by multiple granulomas. |
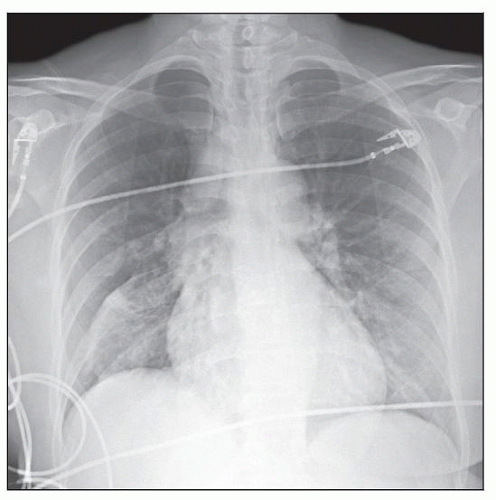 Chest radiograph shows bilateral enlarged hilar lymph nodes. Fine linear and reticular opacities are present in the perihilar lung parenchyma. |
TERMINOLOGY
Definitions
Multisystemic granulomatous disease of unknown etiology
Diagnosis of exclusion
ETIOLOGY/PATHOGENESIS
Exact Etiology and Pathogenesis Unknown
Occupational and environmental exposure
Inorganic particles, insecticides, and moldy environments
Probable role of genetics as shown by assessment of major histocompatibility complex
Positive association with HLA-A1, -B8, and -DR3
Negative association with HLA-B12 and -DR4
Possible role of infectious agents
Mycobacterium tuberculosis
Propionibacterium acnes
T-cell abnormalities
Increased CD4(+) T cells and CD4(+) and CD25(+) regulatory T- cells
Decreased CD1d-restricted natural killer cells
Oligoclonal TCR-αβ T-cell repertoire
Cytokines: Increased interferon-γ and interleukin-2
CLINICAL ISSUES
Epidemiology
Incidence
10-20 per 100,000 population
Age
All ages; peak 20-39 years
Gender
Female preponderance
Ethnicity
Lifetime risk in USA is 2.4% in African-Americans and 0.85% in Caucasians
More likely to be chronic and fatal in African-Americans
Presentation
Constitutional symptoms are common
Fatigue, malaise, fever, night sweats, and weight loss
Symptoms related to organ involvement
Lungs: Dyspnea and cough
Heart: Loss of ventricular function and sudden death
Eyes: Keratoconjunctivitis, uveitis, retinal vasculitis
Skin: Maculopapular eruptions, nodules, plaque-like lesions
Erythema nodosum
Painful, red, subcutaneous lesions on anterior surface of legs
Associated with sarcoidosis but not specific
Musculoskeletal: Arthritis
Kidneys and electrolytes: Abnormal calcium metabolism
Extrarenal production of calcitriol by activated macrophages
Nervous system: Central and peripheral nervous system can be affected
Hypothalamic hypopituitarism
Diabetes insipidus
Lymphocytic meningitis
Other organs: Symptoms directly related to organ involvement
Endocrine system, reproductive system, gastrointestinal tract
Lofgren syndrome: Occurs in subset of patients
Erythema nodosum, hilar lymphadenopathy, migratory polyarthralgias, and fever
In approximately 50% of cases, patients are asymptomatic when 1st diagnosed
Incidental detection by radiographic studies
Most children are asymptomatic
Laboratory Tests
Anemia, leukopenia, and thrombocytopenia
Uncommon but can be observed
Erythrocyte sedimentation rate is often increased
Hypercalciuria and hypercalcemia
Liver involvement results in increased serum alkaline phosphatase levels
Serum angiotensin converting enzyme (ACE) increased in 75% patients
D-dimer levels can be increased
Bronchoalveolar lavage
Flow cytometry immunophenotypic analysis
Increased lymphocyte percentage
Increased CD4:CD8 ratio
Decreased CD3(+), CD56(+) cytotoxic T cells
Kveim test, intradermal injection
Treatment
Indications for treatment
Most patients do not require therapy
Asymptomatic patients with low stage of disease have high rate of spontaneous remission
Indication for treatment of pulmonary sarcoidosis
Deteriorating lung function
Worsening symptoms
Progressive radiographic changes
Indications for treatment of extrapulmonary sarcoidosis
Ocular, neurologic, myocardial, or renal sarcoidosis or hypercalcemia need treatment to avoid consequences
Vision loss, impaired nervous system function, fatal arrhythmias, or renal damage
Treatment modalities
Oral or inhaled glucocorticoids
Other treatment modalities are largely experimental
Immunosuppressive and cytotoxic drugs: Methotrexate, cyclophosphamide, cyclosporin
TNF-α blockers: Infliximab, etanercept
Nonsteroidal anti-inflammatory agents
Heart and lung transplantation
Prognosis
Varies from patient to patient and depends on
Symptomatic vs. asymptomatic
Organ involvement and severity
Proper treatment received
IMAGE FINDINGS
Radiographic Findings
Chest radiograph for pulmonary staging; cannot assess disease activity or functional defects
Stage I: Bilateral hilar lymphadenopathy
Often accompanied by right paratracheal lymph node enlargement
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


