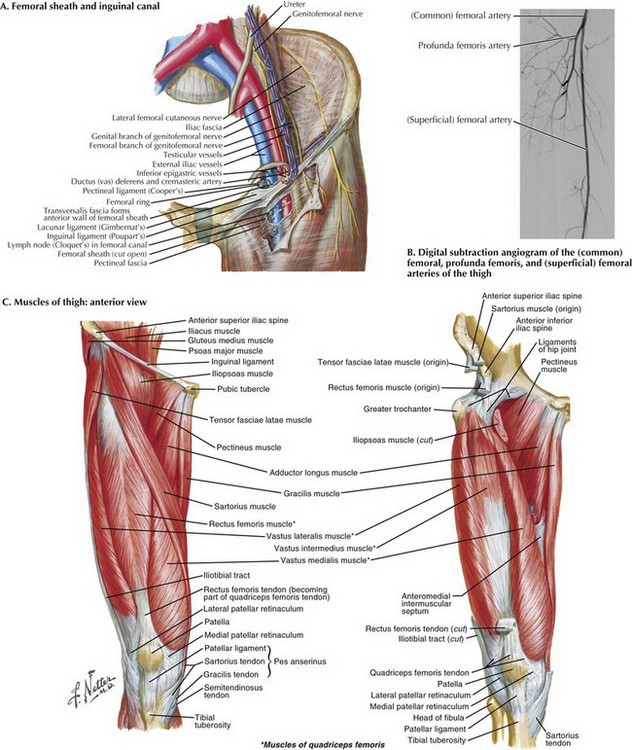
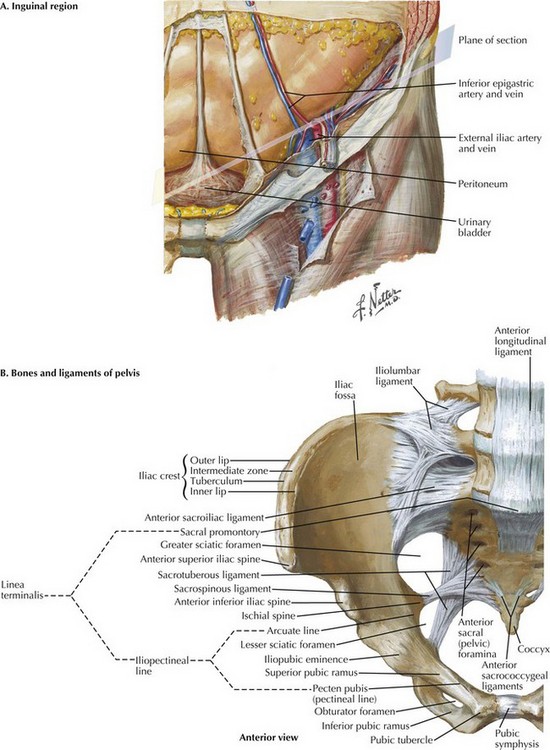
Chapter 36 The femoral artery is an extension of the external iliac artery and by convention begins at the inguinal ligament. The first segment of the femoral artery and the femoral vein are enclosed within the femoral sheath and separated by a fiber septum (Fig. 36-1, A). The femoral sheath is a dense, fibrous band primarily consisting of two layers of fascia; the posterior aspect is a continuation of the fascia covering the pectineus muscle, and the anterior aspect is an extension of the transversalis fascia. As the femoral artery moves obliquely over the pectineus muscle, it divides into two branches, the profunda femoris and superficial femoral (Fig. 36-1, B). The superficial femoral artery exits the femoral triangle into the subsartorial (Hunter’s) canal, crosses above the adductor longus muscle, and runs beneath the sartorius muscle (Fig. 36-1, C). As it moves distally, the superficial femoral artery decreases in caliber, eventually forming the popliteal artery. The most common approach allowing complete exposure of the common femoral artery and its branches is the vertical incision. The incision starts approximately at the midpoint of the inguinal ligament (Fig. 36-2, A). The patient is placed in the supine position. Location of the femoral pulse will guide the incision. Starting the incision directly over the pulse, 2 to 3 cm above the inguinal ligament, the surgeon continues the incision 4 to 8 cm distally toward the tip of the femoral triangle. In some cases, the patient’s pulse may not be palpable because of extensive calcification. If no pulse can be palpated, anatomic landmarks are identified: the pubic tubercle and anterior iliac spine (Fig. 36-2, B). The incision should be made at the midpoint between these two structures.
Saphenofemoral Exposure

Femoral Anatomy
Exposure of Femoral Artery
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine