Chapter 21 Before making an incision, either laparoscopic or open, it is important to understand the relationship between surface anatomy and the abdominal anatomy (Fig. 21-1, A). Understanding the location of the most difficult part of the anatomy or most tethered portion of the colon will assist in appropriately placing an incision. Also, in the morbidly obese patient, surface anatomy, such as the location of the umbilicus, may be greatly altered. The umbilicus may reach down to the pubis and overlie a large pannus, which may distort normal relationships with internal anatomy. Although the right colon is typically tethered by the ileocolic artery, lateral attachments, and the middle colic artery, the inferior portion of the right colon and ileum will be very mobile after the surgery is performed. Attachments to the middle colic and lesser sac are typically the most tethered portion of the operation. In addition, appropriate isolation and evaluation of adequate blood flow of the middle colic vessels is often the most difficult part of the case (Fig. 21-1, B). For this reason, laparoscopic extraction incisions are usually made over the middle colic arteries.
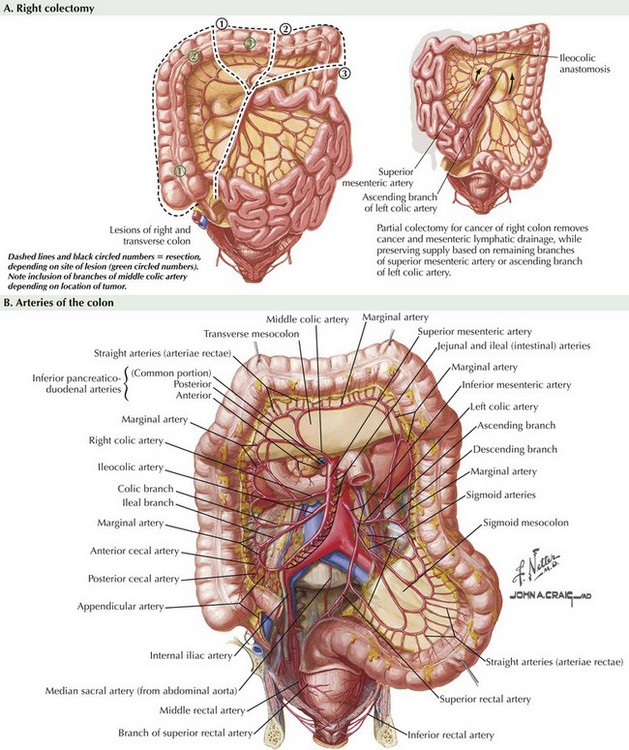
Right Colectomy

Superficial Anatomy and Topographic Landmarks
Basicmedical Key
Fastest Basicmedical Insight Engine