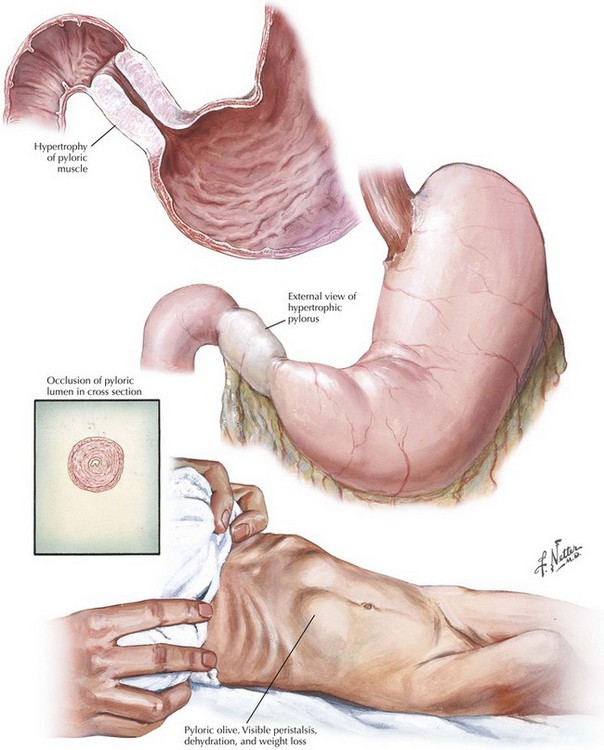
Chapter 10 A diagnosis of pyloric stenosis depends on both patient history and physical examination. Most patients will initially be seen with progressive, nonbilious projectile vomiting at 2 to 8 weeks of age. Patients may show signs of metabolic alkalosis, dehydration, and malnutrition, depending on duration of symptoms. On examination, visible peristaltic waves at the epigastrium and a palpable mass in the left upper quadrant may be present when the abdominal wall is relaxed. The mass is typically olive shaped, smooth, hard, and about 1 to 2 cm in size (Fig. 10-1). The hypertrophied pylorus can also be appreciated using ultrasonography or an upper gastrointestinal (GI) contrast study. The ultrasonographic criteria for pyloric stenosis include an elongated pyloric channel (14 to 20 mm), an enlarged pyloric diameter (>12 mm), and a thickened muscle wall (>3 mm) (Fig. 10-2, A). A contrast study will demonstrate a distended stomach with a narrowed and elongated pyloric channel. These findings are often referred to as the “string” sign or “double track” sign. Upper GI studies can also show “shoulders” at the proximal end of the pylorus, indicating the hypertrophied muscle bulging into the gastric lumen, and a pyloric “beak” at the pyloric entrance to the antrum (Fig. 10-2, B).
Pyloromyotomy for Pyloric Stenosis
Clinical Presentation and Diagnosis of Pyloric Stenosis
Preoperative Imaging of Pyloric Stenosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine