Primary Neuroendocrine (Merkel Cell) Carcinoma
David Cassarino, MD, PhD
Key Facts
Terminology
Cutaneous neuroendocrine carcinoma
Clinical Issues
Highly aggressive tumors with greater metastatic potential than melanoma
Rare (approximately 470 cases/year in USA)
Typically occur in sun-damaged skin of elderly
More common in males
Radiotherapy is generally used
Microscopic Pathology
Highly atypical basaloid neoplasm composed of infiltrative cords, trabeculae, and sheet-like areas
Typically dermal-based, but may show epidermal (pagetoid) involvement in up to 20% of cases
Numerous mitoses and apoptotic bodies
Nuclear crush artifact and streaming may be seen, similar to small cell carcinomas
Basaloid cells with high N:C ratio, scant cytoplasm, large nuclei, granular to clear chromatin, and indistinct nucleoli
Ancillary Tests
Immunohistochemistry is important in confirming diagnosis and excluding metastatic carcinoma
MCC is typically positive for keratins, including CK20, with perinuclear dot-like staining
Top Differential Diagnoses
Basal cell carcinoma (BCC)
Metastatic small cell carcinoma (especially pulmonary origin)
Small cell melanoma
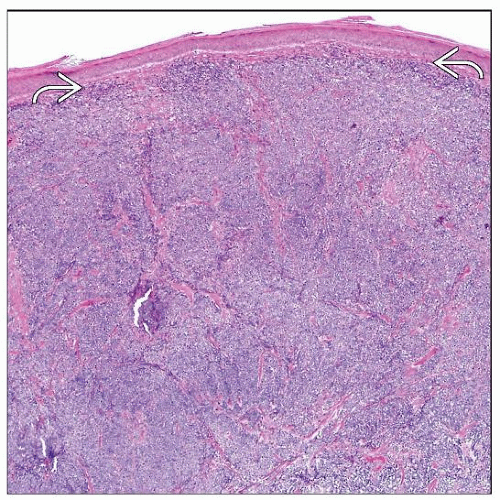 Low magnification of Merkel cell carcinoma shows diffuse dermal involvement by sheets and nodules of atypical basophilic cells. There is a thin grenz zone separating the tumor from the epidermis  . . |
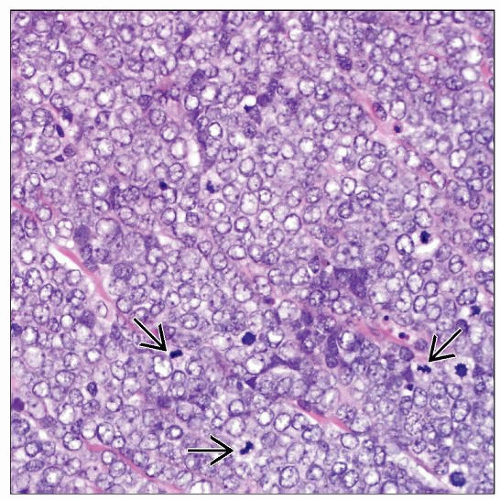 High magnification of MCC shows nuclear molding, hyperchromasia, and vesicular to granular-appearing chromatin. Numerous apoptotic and mitotic figures  are easily identified. are easily identified. |
TERMINOLOGY
Abbreviations
Merkel cell carcinoma (MCC) Synonyms
Cutaneous neuroendocrine carcinoma
Primary small cell carcinoma of skin
Trabecular carcinoma
Definitions
Malignant proliferation of cutaneous neuroendocrine cells
ETIOLOGY/PATHOGENESIS
Infectious Agents
Recent studies have shown strong link to infection with polyomavirus
Merkel cell polyoma virus infection is found in up to 90% of cases
Associated with immunosuppression
Organ transplant and HIV(+) patients have much higher incidence
Cell of Origin
Postulated to represent malignant transformation of cutaneous neuroendocrine (Merkel) cells or pluripotent stem cells, but this remains speculative
CLINICAL ISSUES
Epidemiology
Incidence
Rare
Approximately 470 cases/year in USA
Age
Typically in elderly patients (> 65 years old)
Gender
Male > female (2.5:1)
Ethnicity
Caucasians much more commonly affected than other races
Site
Sun-damaged skin
Usually head and neck or extremities
Presentation
Dermal nodular or plaque-like mass lesion
Rapidly enlarging dermal mass lesion
May be ulcerated &/or hemorrhagic
Natural History
Aggressive tumors with high incidence of local recurrence, lymph node and distant metastasis
Clinical staging should include imaging studies, especially chest and abdominal CT scans
Treatment
Surgical approaches
Complete and wide excision to ensure complete local removal
Consideration may be given to sentinel lymph node (SLN) biopsy
However, SLN positivity does not seem to be very sensitive for regional lymph node involvement, as many patients progress to distant metastases
Adjuvant therapy
Radiotherapy is generally used and may lead to remission in some cases
Chemotherapy is less effective and does not prolong overall survival
Prognosis
High incidence of recurrence (up to 30%) and metastasis (up to 75%)
Overall prognosis is poor
Death due to disease is high, even with treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


