Isolated form rarely progresses to systemic form, but systemic form may develop up to 1 year later
• Liver and gallbladder rarely involved in vasculitides other than PAN
Churg-Strauss syndrome
Rheumatoid arthritis
Henoch-Schönlein purpura
Lupus
Clinical Issues
• Common presenting complaints include fever, abdominal pain
Signs/symptoms can mimic acute acalculous cholecystitis
• Laboratory findings usually reflect severe systemic inflammation
Elevated ESR, CRP, WBC count
• Treatment includes combination of steroids and immunosuppressive agents
Microscopic
• Hallmark lesion of PAN is fibrinoid necrosis and destructive inflammation involving medium-sized arteries
Initially involves media, with destruction of elastic laminae and smooth muscle
Only segment of wall may be affected
As healing occurs, bead-like nodular aneurysm (nodose) may form
– Admixture of early and late lesions is common
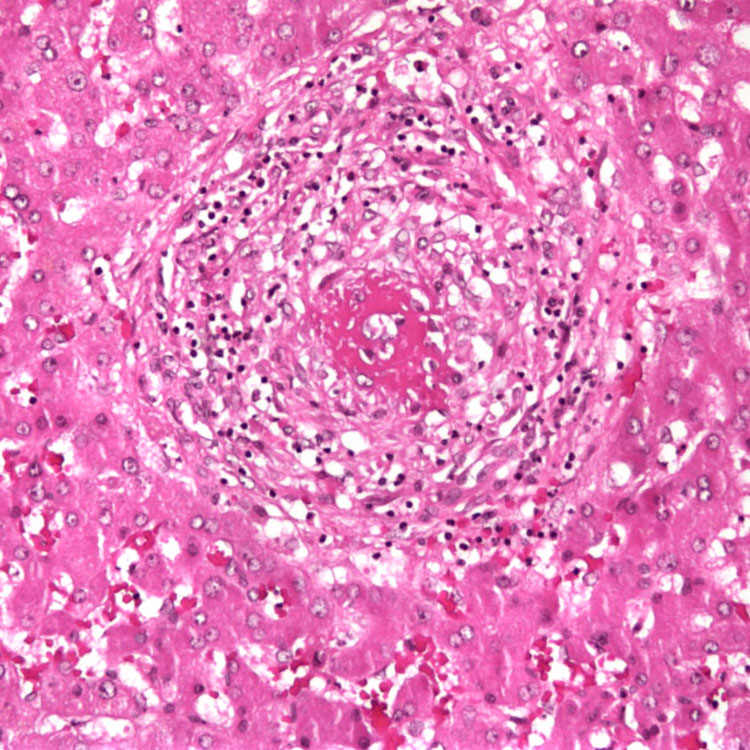
Fibrinoid Necrosis and Inflammation of Vessel Wall This lesion from the gallbladder shows fibrinoid necrosis and destructive inflammation of the vessel wall. The lumen is almost obliterated.
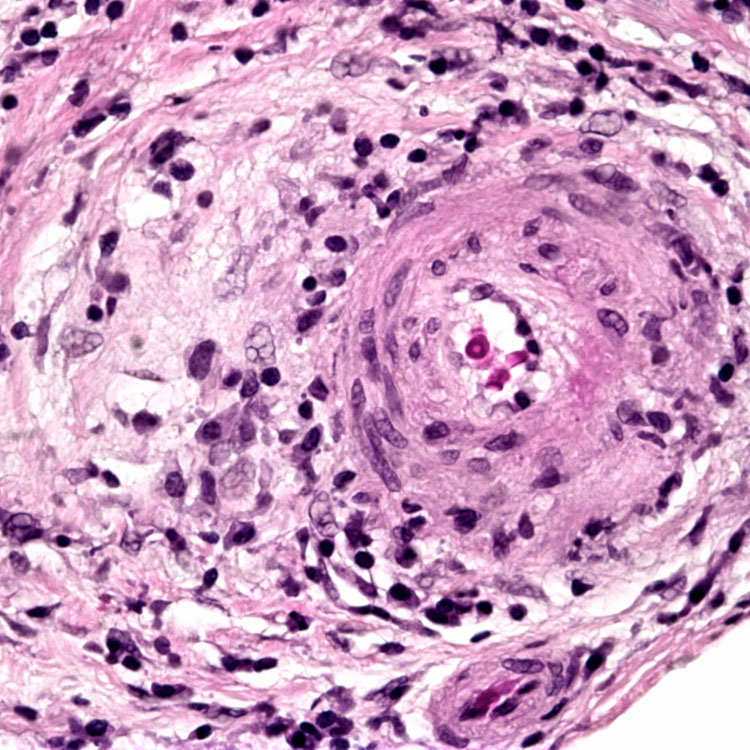
Fibrinoid Necrosis Fibrinoid necrosis is seen within the wall of a medium-sized artery in the liver. This lesion is the hallmark of polyarteritis nodosa. Note the marked luminal compromise.
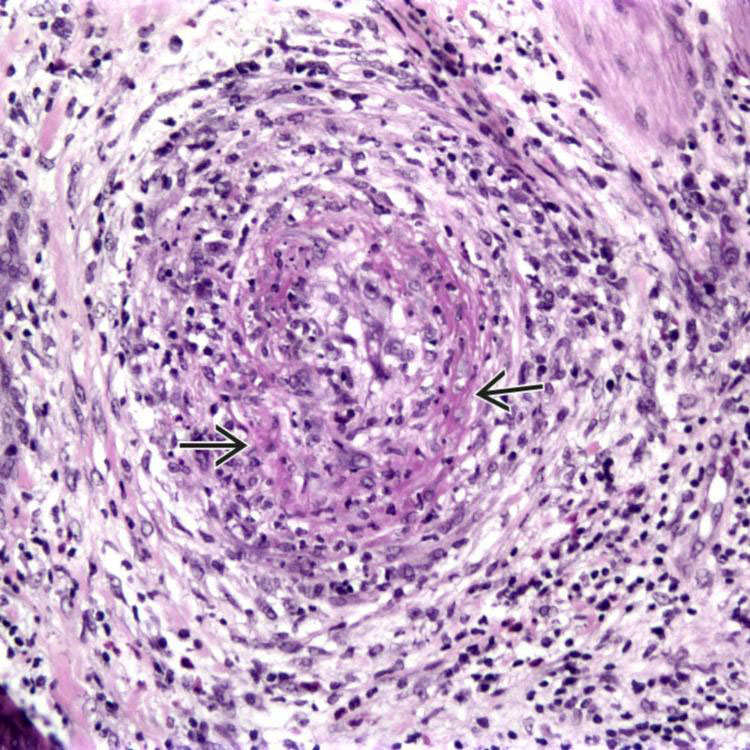
Inflammatory Destruction of Vessel Wall A medium-sized artery in the liver shows fibrinoid necrosis and inflammatory destruction of the vessel wall.
Vessel With Scarring Older lesions in polyarteritis nodosa show resolution of the necrosis and scarring of the vessel wall, sometimes with luminal compromise.
TERMINOLOGY
Abbreviations
• Polyarteritis nodosa (PAN)
Definitions
• Involvement of liver &/or gallbladder by vasculitis (inflammation of blood vessels)
ETIOLOGY/PATHOGENESIS
Liver
• Involved in > 40% of cases
Frequently associated with hepatitis B
Gallbladder
• Involved in 2 distinct settings
Isolated involvement (monoarterial or localized form)
Only gold members can continue reading. Log In or Register to continue









 and destructive inflammation of the vessel wall. The lumen is almost obliterated.
and destructive inflammation of the vessel wall. The lumen is almost obliterated.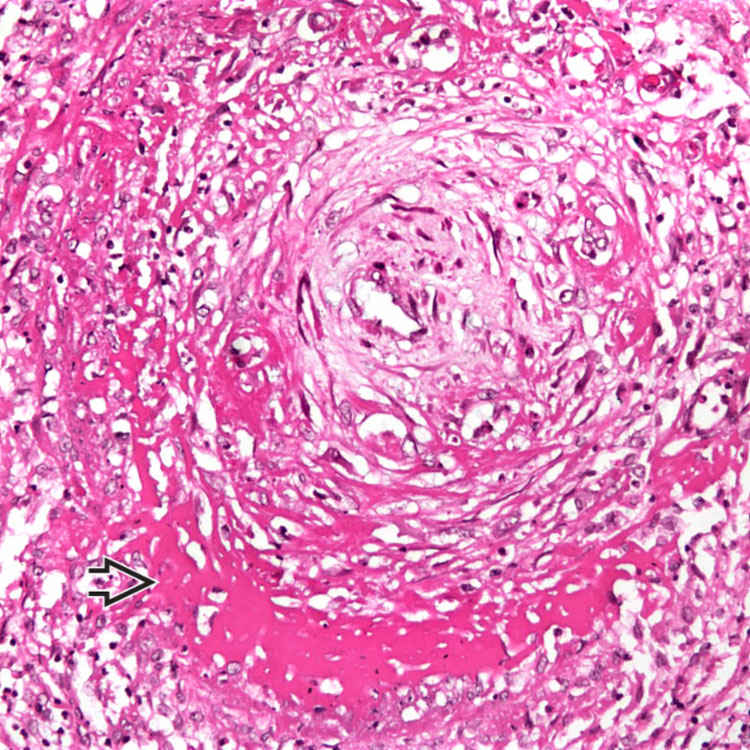
 is seen within the wall of a medium-sized artery in the liver. This lesion is the hallmark of polyarteritis nodosa. Note the marked luminal compromise.
is seen within the wall of a medium-sized artery in the liver. This lesion is the hallmark of polyarteritis nodosa. Note the marked luminal compromise.