Physiology of the Digestive System
LANGUAGE OF SCIENCE
 Before reading the chapter, say each of these terms out loud. This will help you avoid stumbling over them as you read.
Before reading the chapter, say each of these terms out loud. This will help you avoid stumbling over them as you read.
[absorp- swallow, -tion process]
[bili- bile, -rub- red, -in substance]
[cephal- head, -ic relating to]
[chole- bile, -cyst- bladder, -kin- move, –in substance]
[chylo- juice (chyle), -micro- small, -on particle]
[chymo- juice, -tryps- pound, -in substance]
[digest– break down, -tion process]
[de- remove, -feca- waste (feces), -tion process]
[deglut- swallow, -tion process]
[digest- break down, -tion process]
[e- out, -limen- threshold, -ation process]
[e- out, -muls- milk, -i- combining form, -fy process]
[enter- intestine, -ic relating to]
[entero- intestine, -gastr- stomach, -ic relating to, re- back or again, -flex bend]
[entero- intestine, -kin- movement, -ase enzyme]
gastric inhibitory peptide (GIP)
(GAS-trik in-HIB-i-tor-ee PEP-tyde)
[gastr– stomach, –ic relating to, inhibit– restrain, –ory relating to, pept– digest, –ide chemical]
[gastr- stomach, -ic relating to]
[gastr- stomach, -ic relating to]
[gastr- stomach, -in substance]
[hydro- water, -lysis loosening]
[in- within, -gest- carry, -tion process]
[intestin- intestine, -al relating to]
[intestin- intestine, -al relating to]
[intr- inside or within, -insic beside]
[mastica- chew, -tion process]
[digest- break down, -tion process]
[migra– wander, –at- process, motor move, complex embrace]
[mot- move, –il– relating to, -in substance]
[mot- move, –il– relating to, -ity state]
[nucle- nut or kernel (nucleic acid), -ase enzyme]
[pan- all, -creat- flesh, -ic relating to]
[pariet- wall, -al relating to]
[peps- digestion, -in substance]
[peps- digestion, -in substance, -o- combining form, -gen produce]
[pept- digestion, -ide chemical, -ase enzyme]
[peri- around, -stalsis contraction]
[pro- first, -en- in, -zyme ferment]
[pro- in front, -pul- drive, -sion process]
[retro- backward, -pul- drive, -sion process]
[secret- separate, -in substance]
[secret- separate, -tion process]
[segment- cut section, -ation process]
[sod- soda, -ium chemical ending, co- with, -trans- across, -port carry]
[tryps- pound, -in substance, -o- combining form, -gen produce]
[zym- ferment (enzyme), -o- combining form, -gen- produce -ic relating to]
LANGUAGE OF MEDICINE
OVERVIEW OF DIGESTIVE FUNCTION
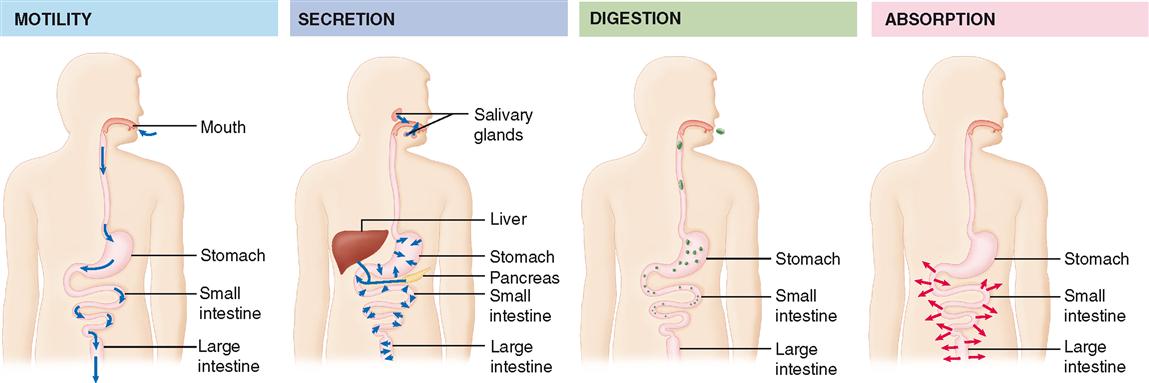
To accomplish the function of making nutrients available to each cell of the body, the digestive system uses various mechanisms (Table 29-1). For example, complex foods must first be taken in—a process called ingestion. Then, complex nutrients are broken down into simpler nutrients in the process that gives this system its name: digestion. To physically break large chunks of food into smaller bits and to move it along the tract, movement (or motility) of the gastrointestinal (GI) wall is required. Chemical digestion—that is, breakdown of large molecules into small molecules—requires secretion of digestive enzymes into the lumen of the GI tract. After being digested, nutrients are ready for the process of absorption, or movement through the GI mucosa into the internal environment. The material that is not absorbed must then be excreted to make room for more material—a process known as elimination. Of course, all these activities must be coordinated, which we have already learned is the process of regulation. Some of the major digestive processes are summarized in Figure 29-1. Digestive regulation is introduced in Box 29-1.
TABLE 29-1
Primary Mechanisms of the Digestive System
| MECHANISM | DESCRIPTION |
| Ingestion | Process of taking food into the mouth, starting it on its journey through the digestive tract |
| Digestion | A group of processes that break complex nutrients into simpler ones, thus facilitating their absorption; mechanical digestion physically breaks large chunks into small bits; chemical digestion breaks molecules apart |
| Motility | Movement by the muscular components of the digestive tube, including processes of mechanical digestion; examples include peristalsis and segmentation |
| Secretion | Release of digestive juices (containing enzymes, acids, bases, mucus, bile, or other products that facilitate digestion); some digestive organs also secrete endocrine hormones that regulate digestion or metabolism of nutrients |
| Absorption | Movement of digested nutrients through the gastrointestinal (GI) mucosa and into the internal environment |
| Elimination | Excretion of the residues of the digestive process (feces) from the rectum, through the anus; defecation |
| Regulation | Coordination of digestive activity (motility, secretion, etc.) |
Box 29-1
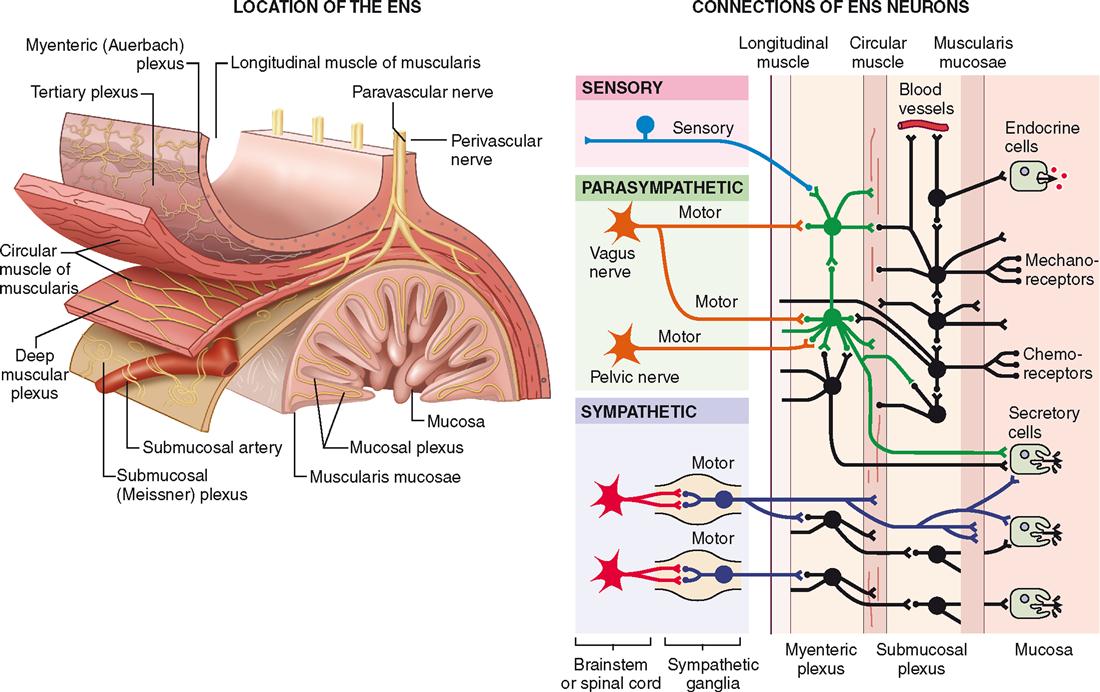
As we discussed in Chapter 28, the gastrointestinal (GI) wall includes an intramural plexus of nerve pathways. This complex arrangement of neurons is made up largely of the submucosal plexus (of Meissner) and the myenteric plexus (of Auerbach). Figure 28-2 on p. 863 clarifies the locations of these two structures and also shows that they are connected not only to each other but also to the CNS (central nervous system) and the GI muscles and mucous membrane. All of these structures work together in a coordinated system called the enteric nervous system (ENS).
The ENS is often called a “mini brain” or “second brain” because it includes afferent neurons, interneurons, and efferent neurons that independently operate their own nervous reflexes. Thus the ENS can act as “its own brain” in many ways. However, the ENS is certainly influenced by the CNS—as you can see in the diagram here. Because it operates as an involuntary, autonomic system, many physiologists consider the ENS to be another division of the autonomic nervous system (ANS). As the diagram shows, there is certainly communication between the ENS and the various divisions of the ANS.
Operation of the ENS, like the brain, seems to involve the storage and retrieval of memories and the establishment of repeating patterns of response.
Of course, this “second brain” has a complete set of different neurotransmitters that help carry out the complex functions of coordinating enteric reflexes. The list of major ENS neurotransmitters includes some familiar names: acetylcholine (ACh), enkephalins, substance P, serotonin, and nitric oxide (NO). Also on the list is an important peptide neurotransmitter, vasoactive intestinal peptide (VIP). Like other peptide neurotransmitters, VIP helps modulate neuron function—in this case, involving inhibition of intestinal smooth muscle or stimulation of intestinal secretions.
The ENS also helps establish a nervous-immune connection (neuroimmune function). For example, neurotransmitters from the ANS and from the ENS can stimulate mast cells in the wall of the GI tract to release histamine and other regulatory molecules. Histamine, for example, stimulates acid secretion in the stomach, besides having the immune functions previously discussed (see Chapter 24).
As we shall see throughout this chapter, the ENS works with other divisions of the nervous system, with the endocrine system, and with local regulatory mechanisms to achieve the coordination of incredibly complex, finely tuned mechanisms of motility (movement), secretion, digestion, and other functions.
Note that Figure 29-1 also illustrates that from a functional perspective, the lumen of the alimentary canal is really a tubelike extension of the external environment that goes right through the middle of the body. Thus digested materials are not truly “part of the body” until they’ve been absorbed into the internal environment.
After we have explored the various mechanisms of the digestive process in this chapter, we will be ready for Chapter 30, which discusses the assimilation of nutrients after they have been absorbed.
DIGESTION
After food is ingested (taken into the mouth), the process of digestion begins immediately. Digestion is the overall name for all the processes that chemically and mechanically break complex foods into simpler nutrients that can be easily absorbed. We begin our discussion with a brief overview of mechanical digestion and then move on to a discussion of chemical digestion.
Mechanical Digestion
Mechanical digestion consists of all movement (motility) of the digestive tract that brings about the following:



MASTICATION
Mechanical digestion begins in the mouth when the particle size of ingested food material is reduced by chewing movements, or mastication. The tongue, cheeks, and lips play an important role in keeping food material between the cutting or grinding surfaces of the teeth when a person is biting off or chewing food. In addition to reducing particle size, chewing movements serve to mix food with saliva in preparation for swallowing.
DEGLUTITION
The process of swallowing, or deglutition, involves three main steps, or stages, that may be divided into the formation and then movement of a food bolus from the mouth to the stomach (Figure 29-2):
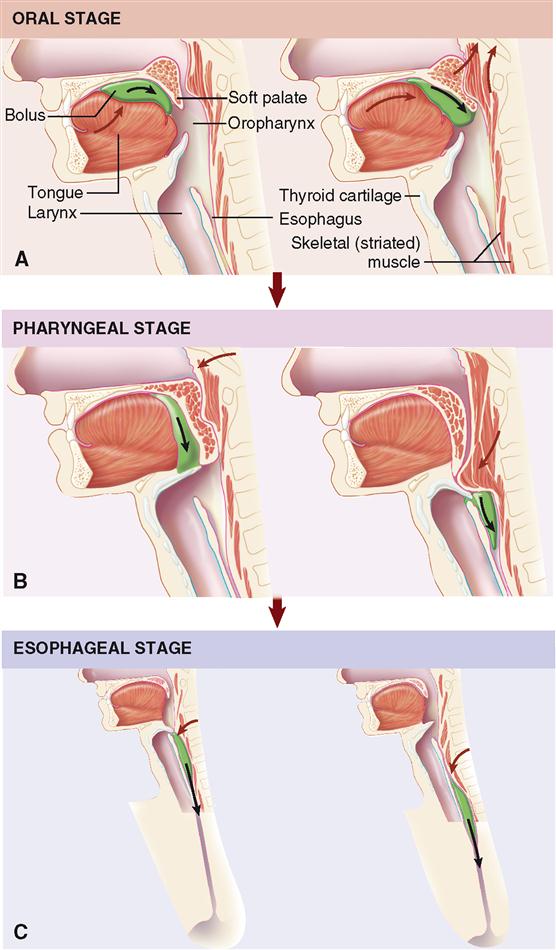
The first step, which is voluntary and under control of the cerebral cortex, involves the formation of a food bolus that is to be swallowed by means of a depression or groove in the middle of the tongue. During the oral stage, the bolus is pressed against the palate by the tongue and then moved back into the oropharynx. The pharyngeal and esophageal stages, both involuntary, consist of movement of food from the pharynx into the esophagus and, finally, into the stomach.
To propel food from the pharynx into the esophagus, three openings must be blocked: mouth, nasopharynx, and larynx. Continued elevation of the tongue seals off the mouth. The soft palate, including the uvula, is elevated and tensed, causing the nasopharynx to be closed off. Food is prevented from entering the larynx by muscle action that causes the epiglottis to block this opening. The mechanism involves raising of the larynx, a process easily noted by palpation of the thyroid cartilage during swallowing. As a result, the bolus slips over the back of the epiglottis to enter the laryngopharynx. Contractions of the pharynx and esophagus compress the bolus into and through the esophageal tube. These steps are involuntary and under control of the deglutition center in the medulla. The presence of a bolus stimulates sensory receptors in the mouth and pharynx, thus initiating reflex pharyngeal contractions. Consequently, anesthesia of sensory nerves from the mucosa of the mouth and pharynx by a drug such as procaine makes swallowing difficult or impossible.
Swallowing is a complex process requiring the coordination of many muscles and other structures in the head and neck. The process must not only occur smoothly but also take place rapidly because respiration is inhibited for the 1 to 3 seconds required for food to clear the pharynx during each swallowing.
PERISTALSIS AND SEGMENTATION
After food enters the lower portion of the esophagus, smooth muscle tissue in the wall of the GI tract takes on primary responsibility for its movement (Box 29-2). The motility produced by smooth muscle is of two main types: peristalsis and segmentation.
Box 29-2
Smooth Muscle Function in the GI Tract
Smooth muscle tissue in the wall of the gastrointestinal (GI) tract differs from other types of muscle tissue in a number of important ways. For example, smooth muscle is slow compared to skeletal muscle. Because the sliding of myofilaments proceeds at a much slower pace than in skeletal muscle, smooth muscle often exhibits a prolonged contraction phase. Because the same amount of energy is used for slow contraction as for fast contraction, GI muscle can sustain tension for long periods without fatigue—exactly what is needed for the long process of digestion.
Another unique functional characteristic of smooth muscle is its ability to maintain basal tone. The basal tone is a continuous state of minimal contraction. Continuous tension is maintained in cells that have enough calcium ions free in the sarcoplasm to generate the contraction response. The force of contraction can increase above the basal tone by way of the effects of an action potential, which causes rapid influx of extracellular calcium.
Gastrointestinal sphincter muscles, as you recall from the previous chapter, are ringlike formations of smooth muscle in the GI wall that act as gateways or valves that regulate movement of chyme from one part of the tract to the next part. Sphincter muscles generally have a higher basal tone than does surrounding smooth muscle—thus constricting the lumen and “keeping the gate closed.” Usually, stimuli in a section preceding the sphincter trigger a decrease in basal tone to allow material to pass through. Some of these reflexes are discussed later in this chapter.
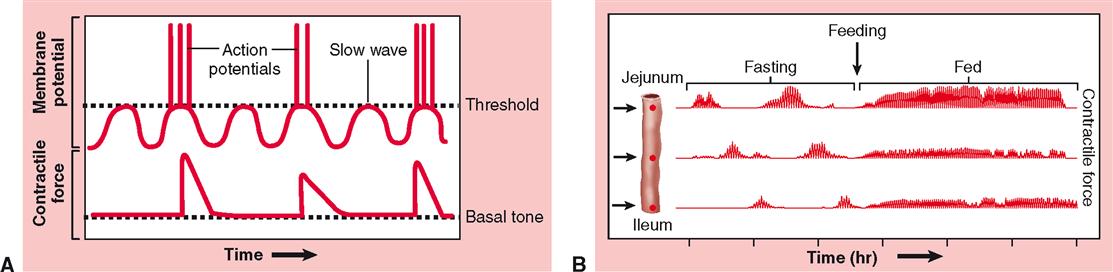
Most of the smooth muscles in the GI wall are electrically coupled by gap junctions—so-called single-unit muscles. Such electrical coupling allows for intrinsic control of smooth muscle contraction, as in cardiac muscle. Smooth muscle fibers exhibit an intrinsic, rhythmic fluctuation in membrane voltage that is sometimes called basic electrical rhythm (BER). As part A of the figure shows, the peaks of these slow waves sometimes reach the threshold potential—thus triggering bursts of action potentials. Because the fibers are electrically coupled, action potentials generated in one fiber spread rapidly to many surrounding fibers. This phenomenon is called pacemaker activity (as we have already seen in the heart with cardiac muscle fibers). Part A of the figure shows the effect of pacemaker activity on the force generated in a local area of the GI muscle. Between action potentials, the muscle cells exhibit the basal tone—but when stimulated by pacemaker potentials, the contractile force increases dramatically. The end result of pacemaker activity is a rather rhythmic increase and decrease in smooth muscle tension.
In part B of the figure, you can see that the small intestine shows an unusual pattern of this rhythmic pacemaker activity during the fasting state. In the fasting state, the electrical rhythm (and therefore the rhythm of contraction) is relatively quiet, except for a coordinated wave of motor activity every 1½ to 2 hours. Each wave of rhythmic contractions is called a migrating motor complex (MMC). One function of the MMC is thought to be that of clearing out any remaining material, such as larger, indigestible particles, bile and other secretions, bacteria, and sloughed off epithelial cells. The MMC pattern is largely triggered by the hormone motilin released from endocrine cells in the duodenum.
Once material enters a segment of the digestive tract, the slow basic rhythm of contraction changes to the rapid rhythms of segmentation (mixing actions) and peristalsis (progressive movement).
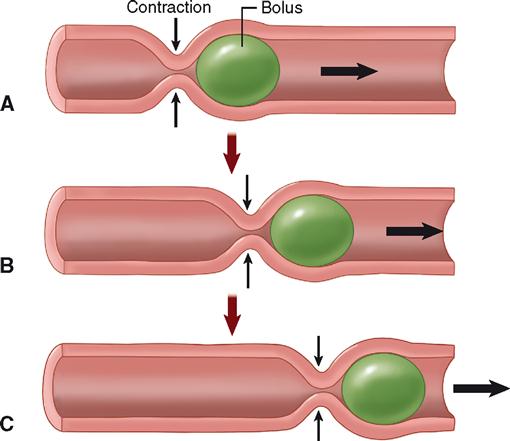
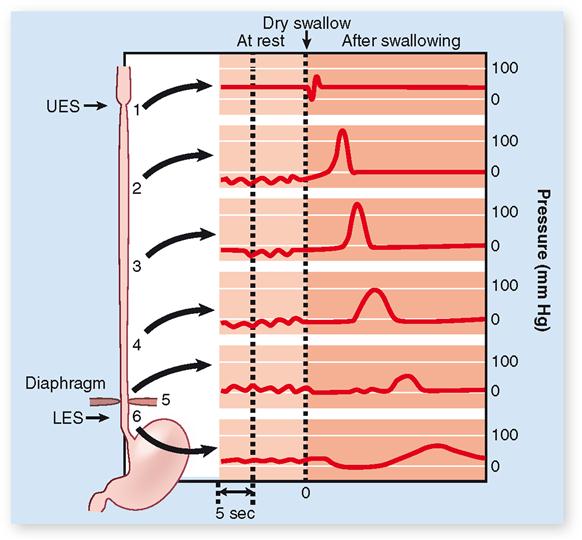
Peristalsis is often described as a wavelike ripple of the muscle layer of a hollow organ. The diagram in Figure 29-3 shows step by step how peristalsis occurs. A bolus stretches the GI wall, triggering a reflex contraction of circular muscle that pushes the bolus forward. This, in turn, triggers a reflex contraction in that location, pushing the bolus even farther. This process continues as long as the stretch reflex is activated by the presence of food. Peristalsis is a progressive kind of motility, that is, a type of motion that produces forward movement of ingested material along the GI tract. Figure 29-4 shows the effects of peristaltic contractions in the esophagus during deglutition.
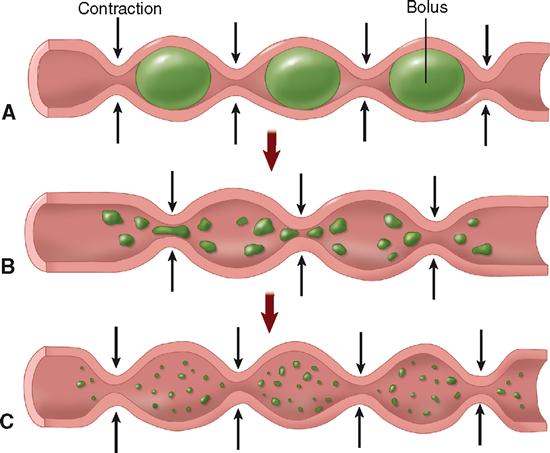
Segmentation can be described simply as mixing movement. Segmentation occurs when digestive reflexes cause a forward and backward movement within a single region, or segment, of the GI tract (Figure 29-5). Such movement helps mechanically break down food particles, mixes food and digestive juices thoroughly, and brings digested food in contact with intestinal mucosa to facilitate absorption.
Peristalsis and segmentation can occur in an alternating sequence. When this happens, food is churned and mixed as it slowly progresses along the GI tract.
REGULATION OF MOTILITY
Gastric Motility
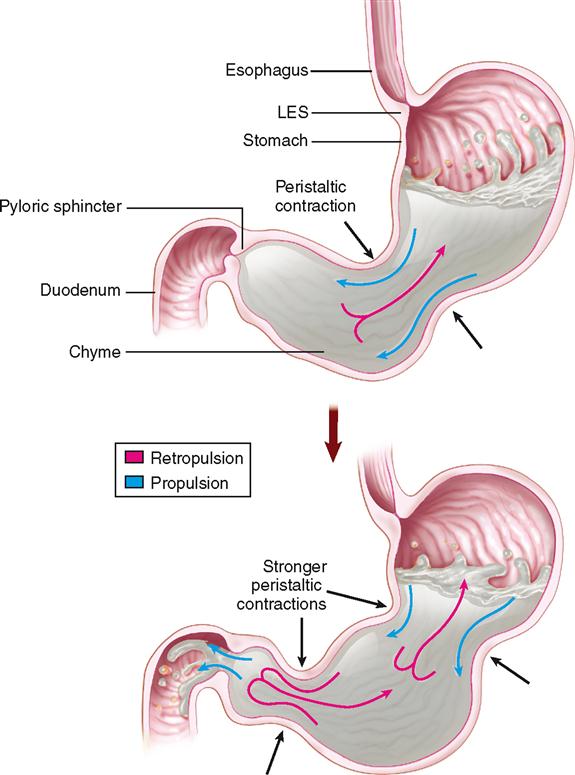
The process of emptying the stomach takes about 2 to 6 hours after a meal, depending on the amount and content of the meal. During its “storage time” in the stomach, food is churned with gastric juices to form a thick, milky material known as chyme, which is ejected about every 20 seconds into the duodenum. As you can see in Figure 29-6, while chyme is in the stomach, it is continually being pushed toward the pyloric sphincter by waves of peristaltic contractions—a process called propulsion. Because the pyloric sphincter remains closed most of the time, the chyme is forced to move backward—a process called retropulsion. Thus, because the chyme is temporarily “trapped,” peristalsis creates a sort of “back-and-forth” movement that helps mix the chyme and gastric juice. Eventually, the contraction force of the pyloric sphincter decreases, allowing a little of the chyme to pass through to the duodenum.
Because the volume of the stomach is large and that of the duodenum is small, gastric emptying must be regulated to prevent overburdening of the duodenum. Such control occurs by way of two principal mechanisms—one hormonal and one nervous. Fats and other nutrients in the duodenum stimulate the intestinal mucosa to release a hormone called gastric inhibitory peptide (GIP) into the bloodstream. When it reaches the stomach wall via the circulation, GIP has an inhibitory effect on gastric muscle, decreasing its peristalsis and thus slowing passage of food into the duodenum. Nervous control results from receptors in the duodenal mucosa that are sensitive to the presence of acid and to distention. Sensory and motor fibers in the vagus nerve then cause a reflex inhibition of gastric peristalsis. This nervous mechanism is known as the enterogastric reflex.
Box 29-3 discusses one important application of concepts of gastric motility.
Box 29-3
 SPORTS and FITNESS
SPORTS and FITNESSExercise and Fluid Uptake
Replacement of fluids lost through sweating during exercise is essential for maintaining homeostasis. Nearly everyone increases the intake of fluids during and after exercise. The main limitation to efficient fluid replacement is how quickly fluid can be absorbed rather than how much a person drinks. Very little water is absorbed until it reaches the intestines, where it is absorbed almost immediately. Thus the rate of gastric emptying into the intestine is critical.
Large volumes of fluid leave the stomach and enter the intestines more rapidly than small volumes do. However, having large volumes in the stomach may be uncomfortable during exercise. Cool fluids (8° to 13° C [46° to 55° F]) empty more quickly than warm fluids. Fluids with a high solute concentration empty slowly and may cause nausea or stomach cramps. Thus large amounts of cool, dilute, or isotonic fluids are best for replacing fluids quickly during exercise.
INTESTINAL MOTILITY
Intestinal motility includes both peristaltic contractions and segmentation. Segmentation in the duodenum and upper jejunum mixes the incoming chyme with digestive juices from the pancreas, liver, and intestinal mucosa. This mixing action also allows the products of digestion to contact the intestinal mucosa, where they can be absorbed into the internal environment. Peristalsis continues as the chyme nears the end of the jejunum—moving the food through the rest of the small intestine and into the large intestine. After leaving the stomach, chyme normally takes about 5 hours to pass all the way through the small intestine.
Several mechanisms are involved in the control of intestinal motility. Peristalsis is regulated in part by the intrinsic stretch reflexes already described. It is also thought to be stimulated by the hormone cholecystokinin (CCK), which is secreted by endocrine cells of the intestinal mucosa when chyme is present.
A list of definitions of the different processes involved in mechanical digestion, along with the organs that accomplish them, is presented in Table 29-2.
TABLE 29-2
Processes of Mechanical Digestion
| ORGAN | MECHANICAL PROCESS | NATURE OF PROCESS |
| Mouth (teeth and tongue) | Mastication | Chewing movements—reduce size of food particles and mix them with saliva |
| Deglutition | Swallowing—movement of food from mouth to stomach | |
| Pharynx | Deglutition | See description above |
| Esophagus | Deglutition | See description above |
| Peristalsis | Rippling movements that squeeze food downward in digestive tract; a constricted ring forms first in one section, then the next, and so on, causing waves of contraction to spread along entire canal | |
| Stomach | Churning |



