Central Nervous System
LANGUAGE OF SCIENCE
 Before reading the chapter, say each of these terms out loud. This will help you avoid stumbling over them as you read.
Before reading the chapter, say each of these terms out loud. This will help you avoid stumbling over them as you read.
[amygdal- almond, -oid like] pl., nuclei
(an-TEER-ee-or KOR-ti-koh-spy-nal)
[ante- front, -er- more, -or quality, cortic- bark, -spin- backbone, -al relating to, tract- trail]
(an-TEER-ee-or SPY-no-tha-lam-ik)
[ante- front, -er- more, -or quality, spino- backbone, -thalam- inner chamber, -ic relating to]
[arbor tree, vitae of life] pl., arbores vitae
[bas- foundation, -al relating to, nucle- nut or kernel] sing., nucleus
[bio- life, -o- combining form, –log- words (study of), -ical relating to]
[caud- tail, equina of a horse] pl., caudae equinae
[caud- tail, -ate of or like, nucleus nut or kernel] pl., nuclei
central sulcus (Rolando fissure)
(SUL-kus [FISH-ur of roh-LAHN-doh])
[sulcus trench, Luigi Rolando Italian physician] pl., sulci
[cereb- brain, -ellum small thing] pl., cerebella or cerebellums
[cerebr- brain, -al relating to, hemi- half, -sphere globe]
[cerebr- brain, -al relating to, ped- foot, -uncl- little]
(seh-ree-broh-SPY-nal FLOO-id)
[cerebr- brain, -spin- backbone, -al relating to]
[cerebrum brain] pl., cerebra or cerebrums
[chorio- skin, -oid like, plexus network] pl., plexi or plexuses
[con- together, -nect- bind, -ome complete set]
[conus cone, medulla middle] pl., coni medullares
[con- together, -volut- roll, -tion process]
(KOHR-pohr-ah kwod-ri-JEM-i-nah)
[corpora bodies, quadri- fourfold, –gemina twin]
[corpus body, callosum callous] pl., corpora callosa
[dent– tooth, -ate of or like, nucleus nut or kernel] pl., nuclei
[descend- move downward, tract- trail]
[di- between, -en- within, -cephalon head] pl., diencephala or diencephalons
[epi- upon, -dura- hard, -al relating to]
[epi- upon, -thalamus inner chamber] pl., epithalami
[extra- outside, -pyramid- pyramid, -al relating to, tract- trail]
[falx sickle, cerebelli of the cerebellum (small brain)] pl., falces cerebelli
[falx sickle, cerebri of the cerebrum] pl., falces cerebri
(fah-SIK-yoo-lus KYOO-nee-ay-tus)
[fasci- bundles, -iculus little, cuneatus wedgelike] pl., fasciculi
(fah-SIK-yoo-lus GRAH-sil-iss)
[fasci- bundles, -iculus little, gracilis thin] pl., fasciculi
[filum thread, termin- boundary, -al relating to] pl., fila terminales
[front- forehead, -al relating to]
[funi- rope, -icul- little] pl., funiculi
[hypo- under or below, –thalamus inner chamber] pl., hypothalami
(SAIR-eh-bell-ar peh-DUNG-kuls)
[infer- lower, -or quality, colli- hill, -iculus small] sing., colliculus
[infundibulum funnel] pl., infundibula
[intern- inside, -al relating to, caps- box, -ula little]
(LAT-er-al kohr-ti-koh-SPY-nal)
[later- side, -al relating to, cortico- bark, -spin- backbone, -al relating to, tract- trail]
lateral fissure (Sylvius fissure)
[FISH–ur of SIL–vi–us] [later- side, -al relating to, Franciscus Sylvius German medical professor]
(LAT-er-al spy-notha-LAM-ik trakt)
[lent- lentil (lens), –form shape, nucleus nut or kernel] pl., nuclei
[longitud- length, -al relating to]
[medulla middle, oblongata oblong] pl., medullae oblongatae
[mela- black, -ton- tone, -in substance]
[mening membrane] sing., meninx
(SAIR-eh-bell-ar peh-DUNG-kul)
[cerebell- cerebellum (small brain), -ar relating to, ped- foot, -uncl little]
[occipit- back of head, -al relating to]
[opti- vision, -ic relating to, chiasma crossed lines] pl., chiasmata, chiasms, or chiasmas
[pariet- wall, -al relating to]
(pah-RYE-eh-toh-ok-SIP-i-tal SUL-kus)
[parieto- wall, -occipit- back of head, -al relating to, sulcus trench] pl., sulci
[pine- pine, -al relating to, gland acorn]
[pyrami- pyramid, -al relating to, tract- trail]
reticular activating system (RAS)
[ret- net, -ic– relating to, -ul- little, -ar characterized by]
[ret- net, -ic– relating to, -ul- little, -ar characterized by]
[ret- net, -ic– relating to, -ul- little, -spin- backbone, -al relating to, tract- trail]
[rubro- red, – spin- backbone, -al relating to, tract- trail]
[spin- backbone, -al relating to]
[spin- backbone, -al relating to, tract- trail]
[spino- backbone, -cerebell– cerebellum (small brain), -ar relating to, tract- trail]
[spino- backbone, -tect- roof, -al relating to, tract- trail]
[spino- backbone, -thalam- inner chamber, -ic relating to]
[sub- beneath, -arachn- spider, -oid like]
[sub- beneath, –dura- hard or tough, -al relating to]
(SAIR-eh-bell-ar peh-DUNG-kuls)
[super- over or above, -or quality, colli- hill, -iculus small] sing., colliculus
[tecto- roof, -spin- backbone, -al relating to, tract- trail]
[tempor- temple of head, -al relating to]
(ten-TOR-ee-um sair-eh-BEL-lee)
[tentorium tent, cerebelli of the cerebellum (small brain)] pl., tentoria cerebelli
[thalamus inner chamber] pl., thalami
[ventr- belly, –al relating to]
[vestibul- entrance hall, -spino- backbone, -al relating to, tract- trail]
LANGUAGE OF MEDICINE
acquired immune deficiency syndrome (AIDS)
(ah-KWYERD IM-yoon deh-FISH-en-see SIN-drohm)
[syn- together, -drome running or (race)course]
[Alois Alzheimer German neurologist]
[cerebr- brain, -al relating to, palsy paralysis (para- beyond, –lysis loosening)]
[cerebr- brain, –al relating to, plastic- moldable, -ity state]
cerebrovascular accident (CVA)
[cerebr- brain, –vas– vessel, cul- little, -ar relating to]
[de- off, -mens- mind, -ia condition of]
(eh-lek-troh-en-SEF-ah-loh-gram)
[electro- electricity, -en- within, -cephal- head, -gram drawing]
(eh-lek-troh-en-SEF-ah-log-rah-fee)
[electro- electricity, -en- inside, -cephal head, -graph- draw, -y activity]
[George S. Huntington American physician]
[hydro- water, -cephalus head]
[mening- membrane, -itis inflammation]
[para- beside, -plegia stroke]
[James Parkinson English physician]
[quadri- fourfold, -plegia stroke]
rapid eye movement (REM) sleep
[spast- pull, -ic relating to, para- beyond, –lysis loosening]
transcutaneous electrical nerve stimulation (TENS) unit
[trans- across, -cutan- skin, –ous relating to]
variant Creutzfeldt-Jakob disease (vCJD)
[Hans G. Creutzfeldt German neurologist, Alfons M. Jakob German neurologist]
Recall from Chapter 13 that the nervous system is said to be composed of two major divisions: the central nervous system (CNS) and the peripheral nervous system (PNS). The reason for designating two distinct divisions is to make the study of the nervous system easier. In this chapter, we discuss the part of the nervous system that lies at the center of the regulatory process: the central nervous system. Comprising both the brain and the spinal cord, the central nervous system is the principal integrator of sensory input and motor output. Thus the central nervous system is capable of evaluating incoming information and formulating responses to changes that threaten our homeostatic balance.
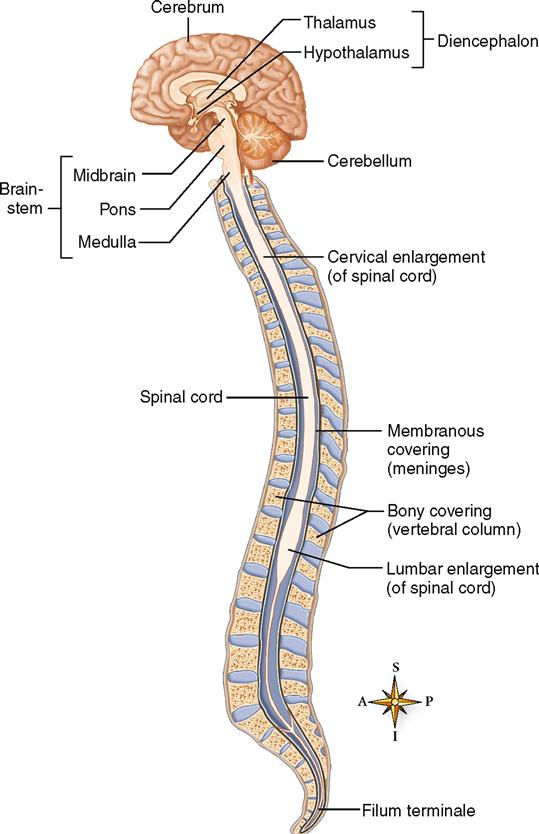
This chapter begins with a description of the protective coverings of the brain and spinal cord. After that, we briefly discuss the watery cerebrospinal fluid (CSF) and the spaces in which it is found. We then outline the overall structure and function of the major organs of the central nervous system, beginning at the bottom with the spinal cord; this is the simplest and least complex part of the CNS. Then our focus moves upward to the more complex brain, beginning first with the narrow brainstem (Figure 14-1) and the roughly spherical cerebellum attached to its dorsal surface. Again shifting our attention upward, we describe the structure and function of the diencephalon and then move on to a discussion of the cerebrum. As we move up the central nervous system, the complexity of both structure and function increases. The spinal cord mediates simple reflexes, whereas the brainstem and diencephalon are involved in the regulation of the more complex maintenance functions, such as regulation of heart rate and breathing. The cerebral hemispheres, which together form the largest part of the brain, perform complex integrative functions such as conscious thought, learning, memory, language, and problem solving. We end the chapter with a discussion of the somatic sensory pathways and the somatic motor pathways. This prepares us for Chapter 15, which covers the peripheral nervous system, Chapter 16, which covers autonomic regulation of vital functions, and Chapter 17, which covers the sense organs.
COVERINGS OF THE BRAIN AND SPINAL CORD
Because the brain and spinal cord are both delicate and vital, nature has provided them with two protective coverings. The outer covering consists of bone: cranial bones encase the brain; vertebrae encase the spinal cord. The inner covering consists of membranes known as meninges. Three distinct layers compose the meninges:
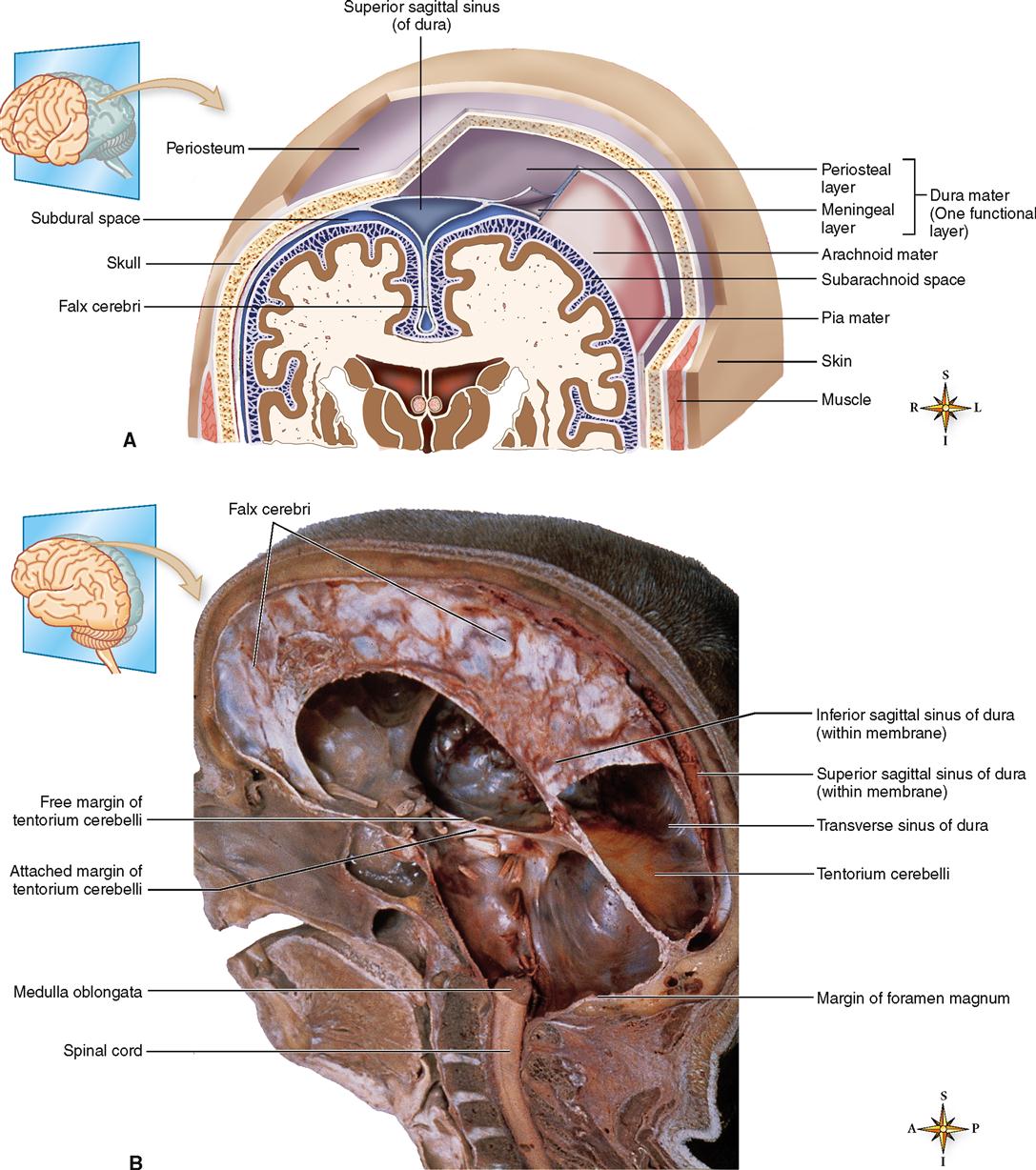
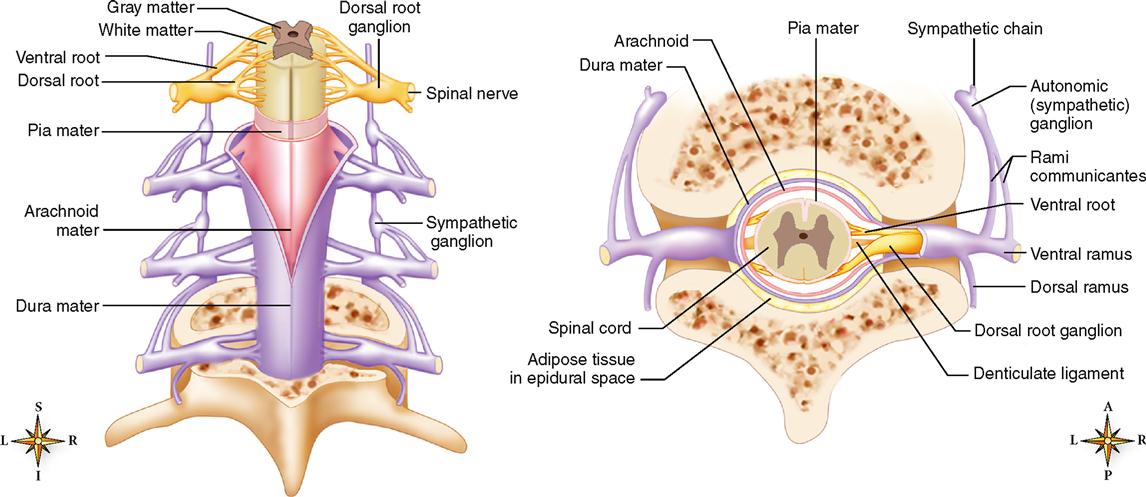
Observe their respective locations in Figures 14-2 and 14-3. The dura mater, made of strong white fibrous tissue, serves as the outer layer of the meninges and also as the inner periosteum of the cranial bones. The arachnoid mater, a delicate, spiderweb-like layer, lies between the dura mater and the pia mater, or innermost layer of the meninges. The transparent pia mater adheres to the outer surface of the brain and spinal cord and contains blood vessels.
The dura mater has three important inward extensions:
1. Falx cerebri. The falx cerebri projects downward into the longitudinal fissure to form a kind of partition between the two cerebral hemispheres. The Latin word falx means “sickle” and refers to the curving sickle shape of this partition as it extends from the roof of the cranial cavity (see Figure 14-2, B).
Figure 14-2 shows a large space within the dura, where the falx cerebri begins to descend between the left and right cerebral hemispheres. This space, called the superior sagittal sinus, is one of several dural sinuses. Dural sinuses function as venous reservoirs, collecting blood from brain tissues for the return trip to the heart.
A number of spaces lie between and around the meninges (see Figure 14-2). Three of these spaces are the following:
The meninges of the cord (see Figure 14-3) continue on down inside the spinal cavity for some distance below the end of the spinal cord. The pia mater forms a slender filament known as the filum terminale (see Figure 14-1). At the level of the third segment of the sacrum, the filum terminale blends with the dura mater to form a fibrous cord that disappears in the periosteum of the coccyx.
Infections of the meninges are discussed in Box 14-1.
 HEALTH matters
HEALTH mattersCEREBROSPINAL FLUID
In addition to its bony and membranous coverings, nature has further protected the brain and spinal cord against injury by providing a cushion of fluid both around the organs and within them. This fluid is the cerebrospinal fluid (CSF). The CSF does more than simply provide a supportive, protective cushion, however. It is also a reservoir of circulating fluid that, along with blood, the brain monitors for changes in the internal environment. For example, changes in the carbon dioxide (CO2) content of CSF trigger homeostatic responses in the respiratory control centers of the brainstem that help regulate the overall CO2 content and pH of the body.
Fluid Spaces
Cerebrospinal fluid is found in the subarachnoid space around the brain and spinal cord and within the cavities and canals of the brain and spinal cord.
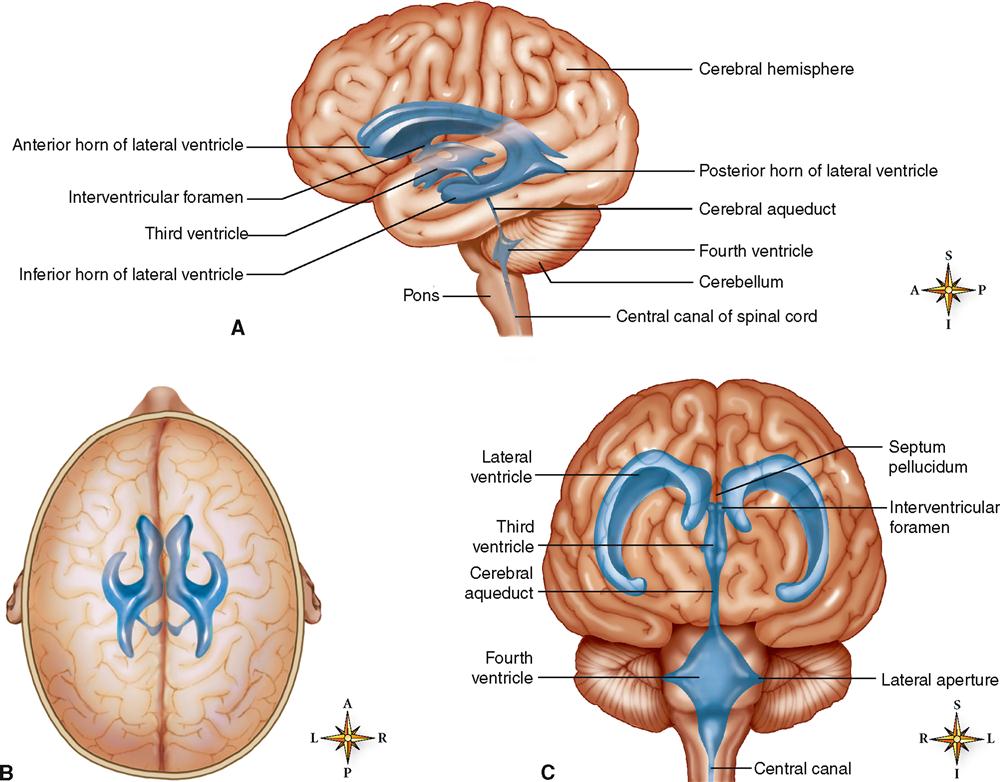
The four large, fluid-filled spaces within the brain are called ventricles. Two of them, the lateral (or first and second) ventricles, are located one in each hemisphere of the cerebrum. As you can see in Figure 14-4, the third ventricle is little more than a thin, vertical pocket of fluid below and medial to the lateral ventricles. The fourth ventricle is a tiny, diamond-shaped space where the cerebellum attaches to the back of the brainstem. Actually, the fourth ventricle is simply a slight expansion of the central canal extending up from the spinal cord.
Formation and Circulation of Cerebrospinal Fluid
Formation of CSF occurs mainly by separation of fluid from blood in the choroid plexuses. Choroid plexuses are networks of capillaries that project from the pia mater into the lateral ventricles and into the roofs of the third and fourth ventricles. Each choroid plexus is covered with a sheet of a special type of ependymal (glial) cell that releases the CSF into the fluid spaces. From each lateral ventricle the fluid seeps through an opening, the interventricular foramen (of Monro), into the third ventricle, then through a narrow channel, the cerebral aqueduct (of Sylvius), into the fourth ventricle (Figure 14-5). Some of the fluid moves from the fourth ventricle directly into the central canal of the cord. Some of it moves out of the fourth ventricle through openings in its roof, two lateral foramina (of Luschka) and one median foramen (of Magendie). These openings allow CSF to move into the cisterna magna, a space behind the medulla that is continuous with the subarachnoid space around the brain and cord. The fluid circulates in the subarachnoid space and then is absorbed into venous blood through the arachnoid villi (fingerlike projections of the arachnoid mater into the brain’s venous sinuses). Briefly, here is the circulation route of cerebrospinal fluid: it is formed as fluid is separated from blood in the choroid plexuses, then it flows into the ventricles of the brain, circulates through the ventricles and into the central canal and subarachnoid spaces, and is then absorbed back into blood.

The amount of CSF in the average adult is about 140 ml (about 23 ml in the ventricles and 117 ml in the subarachnoid space of brain and cord). Box 14-2 explains the diagnostic value of testing a patient’s cerebrospinal fluid.
Box 14-2
 DIAGNOSTIC study
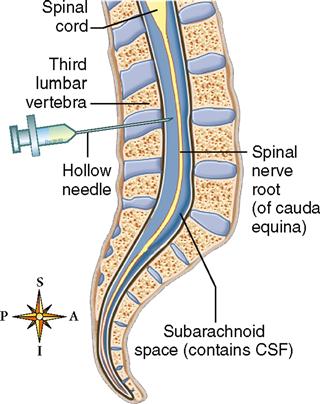
DIAGNOSTIC studyLumbar Puncture
The meninges extends beyond the cord, which provides a convenient location for performing lumbar punctures without danger of injuring the spinal cord. A lumbar puncture is a withdrawal of some of the cerebrospinal fluid (CSF) from the subarachnoid space in the lumbar region of the vertebral column. The physician inserts a needle just above or below the fourth lumbar vertebra, knowing that the spinal cord ends 2 or more centimeters (about an inch) above that level (Figure 1). The fourth lumbar vertebra can be easily located because it lies on a line with the iliac crest. Placing a patient on his or her side with the knees and chest drawn together to arch the back separates the vertebrae sufficiently to create a space in which the needle can be inserted. As the needle enters the CSF, the thin nerve roots roll off the tip of the needle—thus allowing collection of CSF without damaging nerve tissue.
Cerebrospinal fluid removed through a lumbar puncture can be tested for the presence of blood cells, bacteria, or other abnormal characteristics that may indicate an injury or infection, such as meningitis (Figure 2). A sensor called a manometer is sometimes attached to the needle to determine the pressure of the CSF within the subarachnoid space. The lumbar puncture can also be used to introduce diagnostic agents, such as radiopaque dyes for x-ray photography, into the subarachnoid space.

When the circulation of cerebrospinal fluid (CSF) is blocked, there can be dramatic effects on the structure of the brain. An example is hydrocephalus, a condition in which the CSF produces abnormal fluid pressure in the brain. A brief description of hydrocephalus and how it can be treated, along with some dramatic clinical images, can be found in Hydrocephalus online at A&P Connect.

SPINAL CORD
Structure of the Spinal Cord
The spinal cord lies within the spinal cavity, extending from the foramen magnum to the lower border of the first lumbar vertebra (Figure 14-6), a distance of about 45 cm (18 inches) in the average body. The spinal cord does not completely fill the spinal cavity—which also contains the meninges, CSF, a cushion of adipose tissue, and blood vessels.
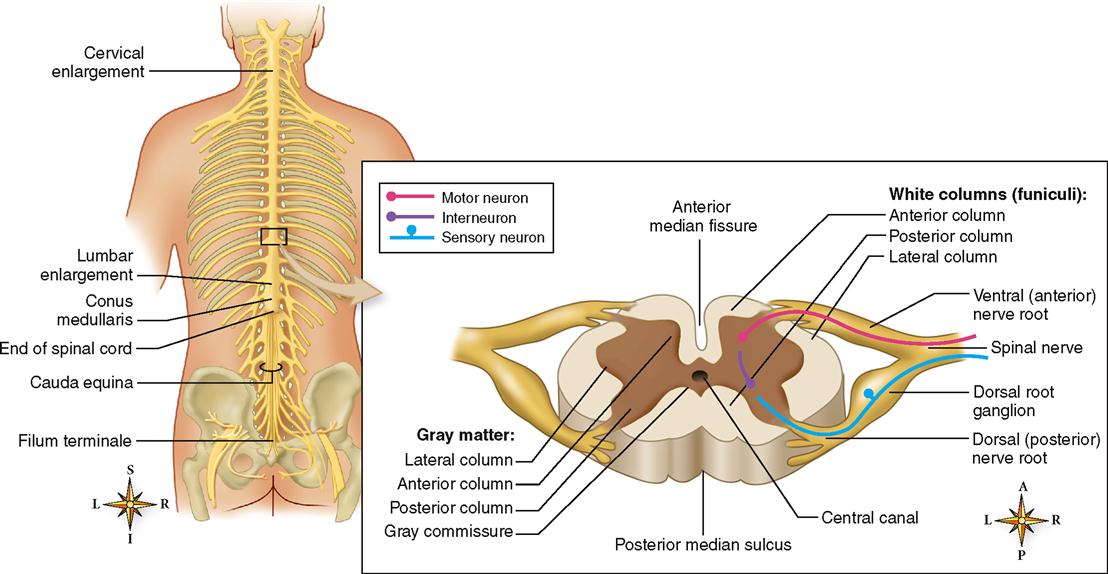
The spinal cord is an oval-shaped cylinder that tapers slightly as it descends and has two bulges, one in the cervical region and the other in the lumbar region (see Figure 14-6). Two deep grooves, the anterior median fissure and the posterior median sulcus, just miss dividing the cord into separate symmetrical halves. The anterior fissure is the deeper and the wider of the two grooves—a useful factor to remember when you examine spinal cord diagrams. It enables you to tell at a glance which part of the cord is anterior and which is posterior.
Two bundles of nerve fibers called nerve roots project from each side of the spinal cord (see Figure 14-6). Fibers comprising the dorsal (posterior) nerve root carry sensory information into the spinal cord. Cell bodies of these unipolar, sensory neurons make up a small region of gray matter in the dorsal nerve root called the dorsal (posterior) root ganglion. Fibers of the ventral (anterior) nerve root carry motor information out of the spinal cord. Cell bodies of these multipolar, motor neurons are in the gray matter that composes the inner core of the spinal cord. Numerous interneurons are also located in the gray matter core of the spinal cord. On each side of the spinal cord, the dorsal and ventral nerve roots join together to form a single mixed nerve called, simply, a spinal nerve. Spinal nerves, components of the peripheral nervous system, are considered in more detail in the next chapter.
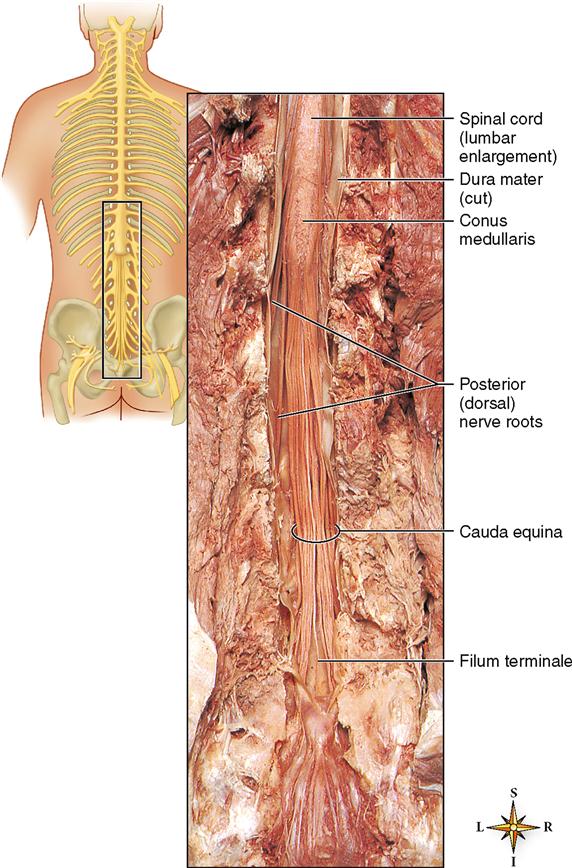
The spinal cord ends at vertebra L1 in a tapered cone called the conus medullaris. As you can see in Figure 14-7, many nerve roots extending from the conus medullaris form a sort of “horse tail” of spinal nerve roots called the cauda equina. Within the cauda equina the long cordlike filum terminale is formed from the spinal meninges.
Although the gray matter core of the spinal cord looks like a flat letter H in transverse sections of the cord, it actually has three dimensions, because the gray matter extends the length of the cord. The H-shaped rod of gray matter is made up of anterior, lateral, and posterior gray columns. When viewed in a cross section, as in Figure 14-6, the columns forming the H appear to spread out like animal horns—and thus are also called anterior, posterior, and lateral gray horns. The left and right gray columns are joined in the middle by a band called the gray commissure. It is through the gray commissure that the central canal carries CSF through the spinal cord. The gray columns consist predominantly of cell bodies of interneurons and motor neurons.
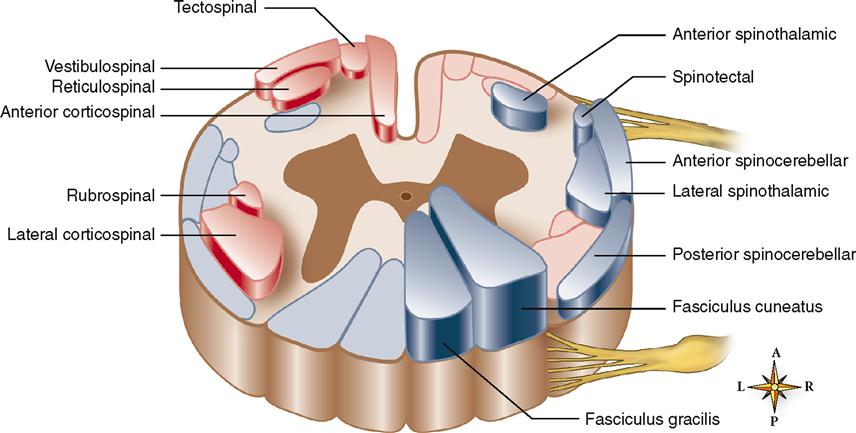
White matter surrounding the gray matter is subdivided in each half of the cord into three white columns or funiculi: the anterior, posterior, and lateral white columns. Each white column, or funiculus, consists of a large bundle of nerve fibers (axons) divided into smaller bundles called spinal tracts, shown in Figure 14-8. The names of most spinal cord tracts indicate the white column in which the tract is located, the structure in which the axons that make up the tract originate, and the structure in which they terminate. For example, the lateral corticospinal tract is located in the lateral white column of the cord. The axons that compose it originate from neuron cell bodies in the spinal cortex (of the cerebrum) and terminate in the spinal cord. The anterior spinothalamic tract lies in the anterior white column. The axons that compose it originate from neuron cell bodies in the spinal cord and terminate in a portion of the brain called the thalamus.
You may wish to refer to the atlas that accompanies this book, where you will find detailed photographs of a human spinal cord. How many structures can you identify in the atlas by sight?
Functions of the Spinal Cord
The spinal cord performs two general functions. Briefly, it provides conduction routes to and from the brain and serves as the integrator, or reflex center, for all spinal reflexes.
Spinal cord tracts provide conduction paths to and from the brain. Ascending tracts conduct sensory impulses up the cord to the brain. Descending tracts conduct motor impulses down the cord from the brain. Bundles of axons compose all tracts.
Tracts are both structural and functional organizations of the nerve fibers of the spinal cord. They are structural organizations in that all the axons of any one tract originate from neuron cell bodies located in the same area of the central nervous system, and all the axons terminate in a single structure elsewhere in the central nervous system. For example, all the fibers of the spinothalamic tract are axons originating from neuron cell bodies located in the spinal cord and terminating in the thalamus. Tracts are functional organizations in that all the axons that compose one tract serve one general function. For instance, fibers of the spinothalamic tracts serve a sensory function. They transmit impulses that produce the sensations of crude touch, pain, and temperature.
Because so many different tracts make up the white columns of the cord, we mention only a few of the more important ones. Locate each tract in Figure 14-8. Consult Tables 14-1 and 14-2 for a brief summary of these tracts.
TABLE 14-1
Major Ascending Tracts of Spinal Cord
| NAME | FUNCTION | LOCATION | ORIGIN* | TERMINATION† |
| Lateral spinothalamic | Pain, temperature, and crude touch on opposite side | Lateral white columns | Posterior gray column on opposite side | Thalamus |
| Anterior spinothalamic | Crude touch and pressure | Anterior white columns | Posterior gray column on opposite side | Thalamus |
| Fasciculi gracilis and cuneatus | Discriminating touch and pressure sensations, including vibration, stereognosis, and two-point discrimination; also conscious kinesthesia | Posterior white columns | Spinal ganglia on same side | Medulla |
| Anterior and posterior spinocerebellar | Unconscious kinesthesia | Lateral white columns | Anterior or posterior gray column | Cerebellum |
| Spinotectal | Touch related to visual reflexes | Lateral white columns | Posterior gray columns | Superior colliculus (midbrain) |
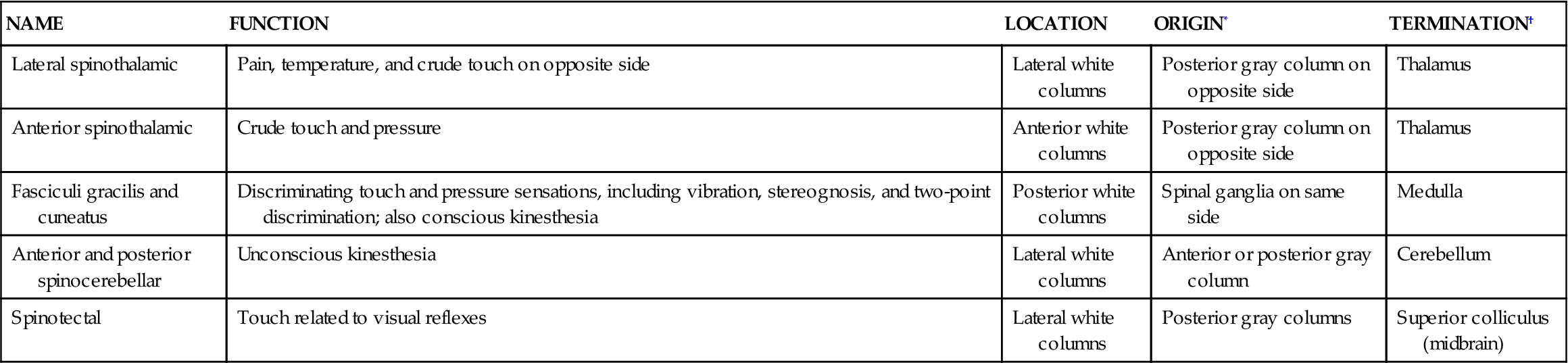
*Location of cell bodies of neurons from which axons of tract arise.
TABLE 14-2
Major Descending Tracts of Spinal Cord
| NAME | FUNCTION | LOCATION | ORIGIN* | TERMINATION† |
| Lateral corticospinal (or crossed pyramidal) | Voluntary movement, contraction of individual or small groups of muscles, particularly those moving hands, fingers, feet, and toes of opposite side | Lateral white columns | Motor areas or cerebral cortex of opposite side from tract location in cord | Lateral or anterior gray columns |
| Anterior corticospinal (direct pyramidal) | Same as lateral corticospinal except mainly muscles of same side | Anterior white columns | Motor cortex but on same side as location in cord | Lateral or anterior gray columns |
| Reticulospinal | Maintain posture during movement | Anterior white columns | Reticular formation (midbrain, pons, medulla) | Anterior gray columns |
| Rubrospinal | Coordination of body movement and posture | Lateral white columns | Red nucleus (of midbrain) | Anterior gray columns |
| Tectospinal | Head and neck movement during visual reflexes | Anterior white columns | Superior colliculus (midbrain) | Medulla and anterior gray columns |
| Vestibulospinal | Coordination of posture/balance | Anterior white columns | Vestibular nucleus (pons, medulla) | Anterior gray columns |
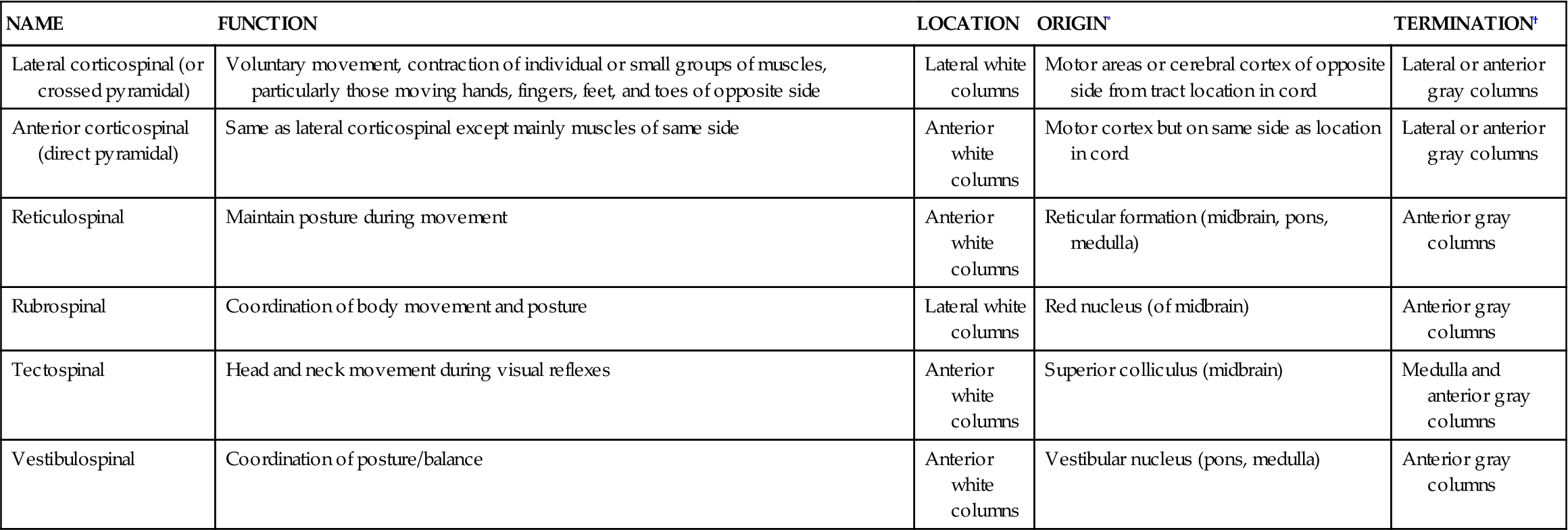
*Location of cell bodies of neurons from which axons of tract arise.
Five important ascending, or sensory, tracts and their functions, stated very briefly, are as follows:
1. Lateral spinothalamic tracts: crude touch, pain, and temperature
2. Anterior spinothalamic tracts: crude touch and pressure
4. Spinocerebellar tracts: subconscious kinesthesia
Further discussion of the sensory neural pathways may be found on pp. 506–507.
Six important descending, or motor, tracts and their functions described in brief are as follows:
2. Anterior corticospinal tracts: same as preceding except mainly muscles of same side of body
3. Reticulospinal tracts: help maintain posture during skeletal muscle movements
4. Rubrospinal tracts: transmit impulses that coordinate body movements and maintenance of posture
5. Tectospinal tracts: head and neck movement related to visual reflexes
6. Vestibulospinal tracts: coordination of posture and balance
Further discussion of motor neural pathways may be found on pp. 490–491.
The spinal cord also serves as the reflex center for all spinal reflexes. The term reflex center means the center of a reflex arc or the place in the arc where incoming sensory impulses become outgoing motor impulses. They are structures that switch impulses from afferent to efferent neurons. In two-neuron arcs, reflex centers are merely synapses between neurons. In all other arcs, reflex centers consist of interneurons interposed between afferent and efferent neurons. Spinal reflex centers are located in the gray matter of the cord.
Reflex centers can act as pain control areas. Pain control areas can inhibit the pain information heading toward the conscious processing centers of the brain. Identifying pain control areas and how they work has lead to the development of transcutaneous electrical nerve stimulation (TENS) units and other therapies to reduce pain. To learn more about this check out Pain Control Areas online at A&P Connect.

BRAIN
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


