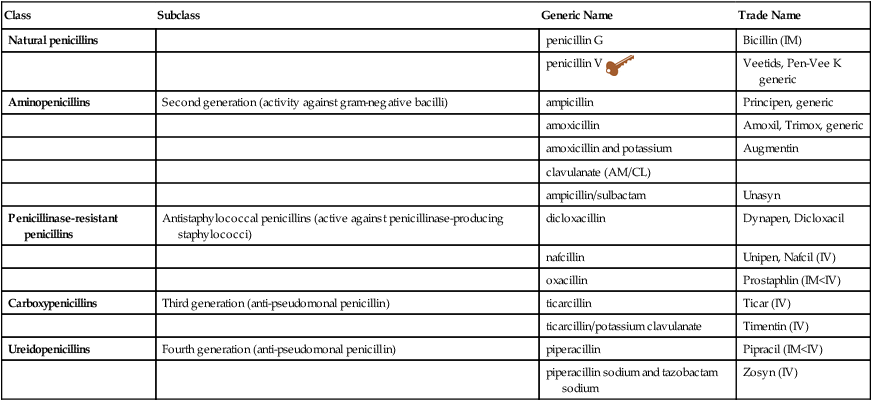
Chapter 59 INDICATIONS See Table 59-1 for specific indications. TABLE 59-1 Penicillin Indications With Dosage and Administration Recommendations
Penicillins
Class
Subclass
Generic Name
Trade Name
Natural penicillins
penicillin G
Bicillin (IM)
penicillin V 
Veetids, Pen-Vee K generic
Aminopenicillins
Second generation (activity against gram-negative bacilli)
ampicillin
Principen, generic
amoxicillin
Amoxil, Trimox, generic
amoxicillin and potassium
Augmentin
clavulanate (AM/CL)
ampicillin/sulbactam
Unasyn
Penicillinase-resistant penicillins
Antistaphylococcal penicillins (active against penicillinase-producing staphylococci)
dicloxacillin
Dynapen, Dicloxacil
nafcillin
Unipen, Nafcil (IV)
oxacillin
Prostaphlin (IM<IV)
Carboxypenicillins
Third generation (anti-pseudomonal penicillin)
ticarcillin
Ticar (IV)
ticarcillin/potassium clavulanate
Timentin (IV)
Ureidopenicillins
Fourth generation (anti-pseudomonal penicillin)
piperacillin
Pipracil (IM<IV)
piperacillin sodium and tazobactam sodium
Zosyn (IV)
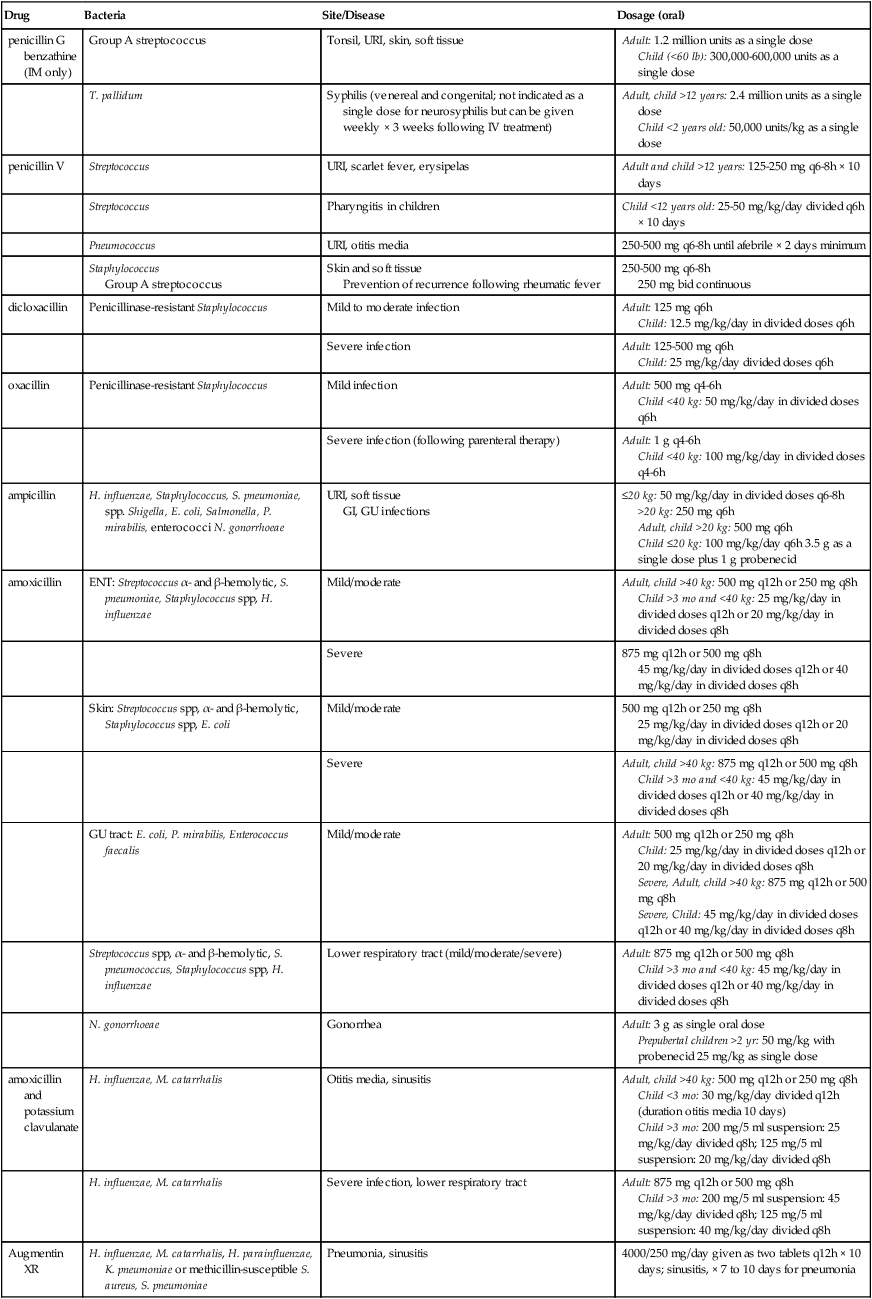
Drug
Bacteria
Site/Disease
Dosage (oral)
penicillin G benzathine (IM only)
Group A streptococcus
Tonsil, URI, skin, soft tissue
Adult: 1.2 million units as a single dose
Child (<60 lb): 300,000-600,000 units as a single dose
T. pallidum
Syphilis (venereal and congenital; not indicated as a single dose for neurosyphilis but can be given weekly × 3 weeks following IV treatment)
Adult, child >12 years: 2.4 million units as a single dose
Child <2 years old: 50,000 units/kg as a single dose
penicillin V
Streptococcus
URI, scarlet fever, erysipelas
Adult and child >12 years: 125-250 mg q6-8h × 10 days
Streptococcus
Pharyngitis in children
Child <12 years old: 25-50 mg/kg/day divided q6h × 10 days
Pneumococcus
URI, otitis media
250-500 mg q6-8h until afebrile × 2 days minimum
Staphylococcus
Group A streptococcus
Skin and soft tissue
Prevention of recurrence following rheumatic fever
250-500 mg q6-8h
250 mg bid continuous
dicloxacillin
Penicillinase-resistant Staphylococcus
Mild to moderate infection
Adult: 125 mg q6h
Child: 12.5 mg/kg/day in divided doses q6h
Severe infection
Adult: 125-500 mg q6h
Child: 25 mg/kg/day divided doses q6h
oxacillin
Penicillinase-resistant Staphylococcus
Mild infection
Adult: 500 mg q4-6h
Child <40 kg: 50 mg/kg/day in divided doses q6h
Severe infection (following parenteral therapy)
Adult: 1 g q4-6h
Child <40 kg: 100 mg/kg/day in divided doses q4-6h
ampicillin
H. influenzae, Staphylococcus, S. pneumoniae, spp. Shigella, E. coli, Salmonella, P. mirabilis, enterococci N. gonorrhoeae
URI, soft tissue
GI, GU infections
≤20 kg: 50 mg/kg/day in divided doses q6-8h
>20 kg: 250 mg q6h
Adult, child >20 kg: 500 mg q6h
Child ≤20 kg: 100 mg/kg/day q6h 3.5 g as a single dose plus 1 g probenecid
amoxicillin
ENT: Streptococcus α- and β-hemolytic, S. pneumoniae, Staphylococcus spp, H. influenzae
Mild/moderate
Adult, child >40 kg: 500 mg q12h or 250 mg q8h
Child >3 mo and <40 kg: 25 mg/kg/day in divided doses q12h or 20 mg/kg/day in divided doses q8h
Severe
875 mg q12h or 500 mg q8h
45 mg/kg/day in divided doses q12h or 40 mg/kg/day in divided doses q8h
Skin: Streptococcus spp, α- and β-hemolytic, Staphylococcus spp, E. coli
Mild/moderate
500 mg q12h or 250 mg q8h
25 mg/kg/day in divided doses q12h or 20 mg/kg/day in divided doses q8h
Severe
Adult, child >40 kg: 875 mg q12h or 500 mg q8h
Child >3 mo and <40 kg: 45 mg/kg/day in divided doses q12h or 40 mg/kg/day in divided doses q8h
GU tract: E. coli, P. mirabilis, Enterococcus faecalis
Mild/moderate
Adult: 500 mg q12h or 250 mg q8h
Child: 25 mg/kg/day in divided doses q12h or 20 mg/kg/day in divided doses q8h
Severe, Adult, child >40 kg: 875 mg q12h or 500 mg q8h
Severe, Child: 45 mg/kg/day in divided doses q12h or 40 mg/kg/day in divided doses q8h
Streptococcus spp, α- and β-hemolytic, S. pneumococcus, Staphylococcus spp, H. influenzae
Lower respiratory tract (mild/moderate/severe)
Adult: 875 mg q12h or 500 mg q8h
Child >3 mo and <40 kg: 45 mg/kg/day in divided doses q12h or 40 mg/kg/day in divided doses q8h
N. gonorrhoeae
Gonorrhea
Adult: 3 g as single oral dose
Prepubertal children >2 yr: 50 mg/kg with probenecid 25 mg/kg as single dose
amoxicillin and potassium clavulanate
H. influenzae, M. catarrhalis
Otitis media, sinusitis
Adult, child >40 kg: 500 mg q12h or 250 mg q8h
Child <3 mo: 30 mg/kg/day divided q12h (duration otitis media 10 days)
Child >3 mo: 200 mg/5 ml suspension: 25 mg/kg/day divided q8h; 125 mg/5 ml suspension: 20 mg/kg/day divided q8h
H. influenzae, M. catarrhalis
Severe infection, lower respiratory tract
Adult: 875 mg q12h or 500 mg q8h
Child >3 mo: 200 mg/5 ml suspension: 45 mg/kg/day divided q8h; 125 mg/5 ml suspension: 40 mg/kg/day divided q8h
Augmentin XR
H. influenzae, M. catarrhalis, H. parainfluenzae, K. pneumoniae or methicillin-susceptible S. aureus, S. pneumoniae
Pneumonia, sinusitis
4000/250 mg/day given as two tablets q12h × 10 days; sinusitis, × 7 to 10 days for pneumonia
Therapeutic Overview
Allergy
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

 Key drug.
Key drug.
Full access? Get Clinical Tree


