Chapter 34 A focused history with a careful physical examination is essential for determining the cause of incontinence. Transient or reversible causes should be ruled out (Table 34-1). A bladder diary is a helpful diagnostic tool that reveals toileting habits, fluid intake, and leakage episodes. Urinalysis and postvoid residual are essential laboratory tests. Further evaluation by specialists may involve urodynamic and imaging tests. TABLE 34-1 Common Contributors to Transient Urinary Incontinence Anticholinergic medications used for urge incontinence include those in this chapter, tricyclic antidepressants (TCAs), and dicyclomine (Bentyl) (discussed in Chapter 29). • Brigham and Women’s Hospital: Urinary incontinence: guide to diagnosis and management (Available at www.guidelines.gov).
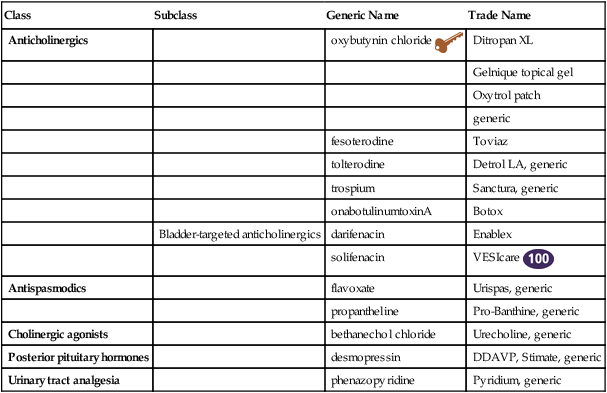
Agents for Urinary Incontinence and Urinary Analgesia
Class
Subclass
Generic Name
Trade Name
Anticholinergics
oxybutynin chloride 
Ditropan XL
Gelnique topical gel
Oxytrol patch
generic
fesoterodine
Toviaz
tolterodine
Detrol LA, generic
trospium
Sanctura, generic
onabotulinumtoxinA
Botox
Bladder-targeted anticholinergics
darifenacin
Enablex
solifenacin
VESIcare 
Antispasmodics
flavoxate
Urispas, generic
propantheline
Pro-Banthine, generic
Cholinergic agonists
bethanechol chloride
Urecholine, generic
Posterior pituitary hormones
desmopressin
DDAVP, Stimate, generic
Urinary tract analgesia
phenazopyridine
Pyridium, generic
Therapeutic Overview
Assessment
Cause
Comment
Delirium
Mental status changes; treat underlying medical condition.
Infection
Irritated detrusor muscle
Atrophic urethritis or vaginitis
May present as dysuria, dyspareunia, burning on urination, urgency, and incontinence; requires a pelvic examination. Treat with estrogen.
Pharmaceuticals
Side effect of numerous agents (e.g., diuretics, NSAIDs, antihypertensives)
Excessive urine output
Peripheral edema, hyperglycemia
Restricted mobility
Cognitive decline, physical weakness
Stool impaction
Requires rectal examination
Mechanism of Action
Anticholinergics
Treatment Principles
Standardized Guidelines
Evidence-Based Recommendations
Agents for Urinary Incontinence and Urinary Analgesia

 Top 100 drug;
Top 100 drug;  Key drug. Key drug because was first marketed for urinary incontinence and remains in popular use.
Key drug. Key drug because was first marketed for urinary incontinence and remains in popular use.


