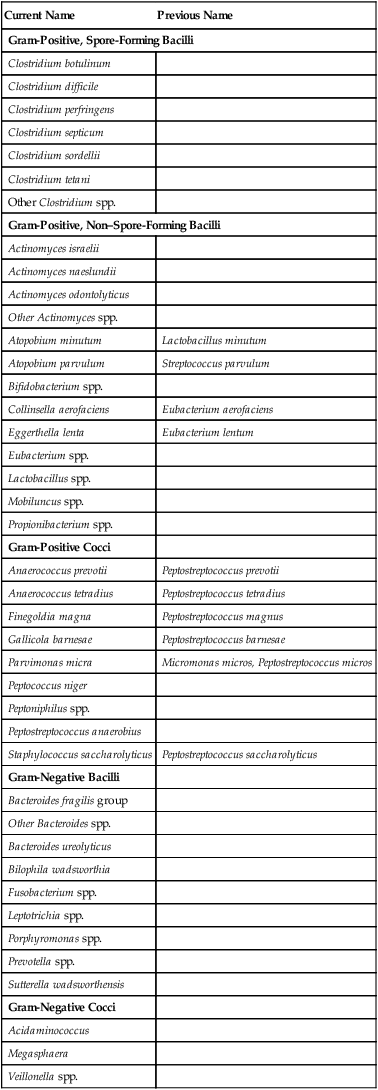
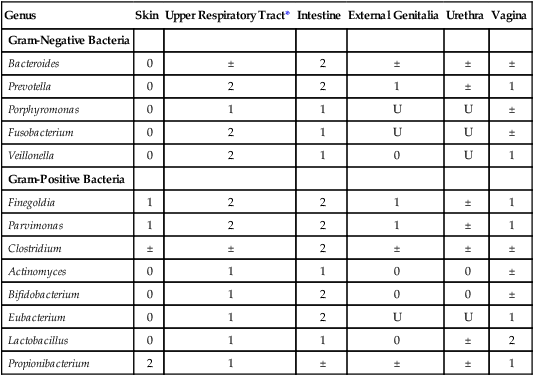
Chapter 42 1. For each group of organisms listed, provide the general characteristics, including Gram stain reactions, colonial morphology, growth requirements (media, oxygen requirement, temperature), laboratory identification, and clinical significance. 2. Differentiate normal anaerobic bacteria from pathogenic bacteria isolated from clinical specimens. 3. Describe the pathogenesis and virulence factors associated with the Clostridium species C. perfringens, C. botulinum, C. difficile, and C. septicum. 4. Define and discuss the pathogenesis for anaerobic cellulitis, gas gangrene, clostridial gastroenteritis, pseudomembranous enterocolitis, botulism, actinomycosis, bacterial vaginosis, and enteritis necroticans. 5. Differentiate the three forms of botulism (food poisoning, wound botulism, and infant botulism). 6. Compare paralysis associated with botulism with tetanus. 7. Explain the procedure for spore isolation and growth using the ethyl alcohol shock procedure. 8. List the appropriate specimen collection, transport, and storage conditions for the recovery of anaerobic organisms. 9. Explain aerotolerance testing, including how to perform the test, what media is used, and the reason or reasons the media is important. 10. Identify the special potency antibiotics and explain the typical resistance patterns used to identify the various anaerobic groups (e.g., gram-positive cocci, gram-negative cocci). 11. Correlate disease signs and symptoms with laboratory data to identify the etiologic agent of infection. As previously described in Chapter 41, the organisms in this chapter predominantly do not grow in the presence of oxygen. Most of the anaerobic bacteria that cause infections in humans are also part of our normal flora. The ecology of these organisms is such that various species and genera exhibit preferences for the body sites they inhabit (endogenous anaerobes) (Table 42-1). Other pathogenic anaerobes (e.g., Clostridium botulinum and Clostridium tetani) are soil and environmental inhabitants (exogenous anaerobes) and are not considered part of the normal human flora. TABLE 42-1 Incidence of Anaerobes as Normal Flora of Humans U, Unknown; 0, not found or rare; ±, irregular; 1, usually present; 2, present in large numbers. *Includes nasal passages, nasopharynx, oropharynx, and tonsils. Modified from Summanen PE, Baron EJ, Citron DM et al: Wadsworth anaerobic bacteriology manual, ed 5, Belmont, Calif, 1993, Star. The ways in which anaerobic infections are acquired are summarized in Table 42-2. Person-to-person nosocomial spread of Clostridium difficile among hospitalized patients presents an enormous clinical and infection control dilemma; however, most anaerobic infections occur when a patient’s normal flora gains access to a sterile site as a result of disruption of some anatomic barrier. TABLE 42-2 Acquisition of Anaerobic Infections and Diseases The types of infections and diseases in humans caused by anaerobic bacteria span a wide spectrum. Certain species, such as C. botulinum and C. tetani, produce some of the most potent toxins known. In contrast, specific virulence factors for the organisms commonly encountered in infections (e.g., B. fragilis group, C. difficile) are not well understood (Table 42-3). TABLE 42-3 Pathogenesis and Spectrum of Disease for Anaerobic Bacteria The clostridia are the endospore-forming, obligately anaerobic (or aerotolerant), catalase-negative, gram-positive bacilli (Figure 42-1). The rods are pleomorphic and may be arranged in pairs or short chains. If spores are not present on Gram stain, the ethanol shock spore or heat shock spore test can separate this group from the non–spore-forming anaerobic bacilli (see Procedure 42-1 on the Evolve site). Some strains of C. perfringens, C. ramosum, and C. clostridioforme may not produce spores or survive a spore test, so it is important to recognize these organisms using other characteristics. Some clostridia typically stain gram negative, although they are susceptible to vancomycin on the disk test. Several species of clostridia grow aerobically (C. tertium, C. carnis, C. histolyticum, and occasional strains of C. perfringens), but they produce spores only under anaerobic conditions. C. perfringens may appear weakly catalase positive.
Overview of Anaerobic Organisms
Epidemiology
Genus
Skin
Upper Respiratory Tract*
Intestine
External Genitalia
Urethra
Vagina
Gram-Negative Bacteria
Bacteroides
0
±
2
±
±
±
Prevotella
0
2
2
1
±
1
Porphyromonas
0
1
1
U
U
±
Fusobacterium
0
2
1
U
U
±
Veillonella
0
2
1
0
U
1
Gram-Positive Bacteria
Finegoldia
1
2
2
1
±
1
Parvimonas
1
2
2
1
±
1
Clostridium
±
±
2
±
±
±
Actinomyces
0
1
1
0
0
±
Bifidobacterium
0
1
2
0
0
±
Eubacterium
0
1
2
U
U
1
Lactobacillus
0
1
1
0
±
2
Propionibacterium
2
1
±
±
±
1
Mode of Acquisition
Examples
Endogenous strains of normal flora gain access to normally sterile sites, usually as result of one or more predisposing factors that compromise normal anatomic barriers (e.g., surgery or accidental trauma) or alter other host defense mechanisms (e.g., malignancy, diabetes, burns, immunosuppressive therapy, aspiration)
Wide variety of infections involving several anatomic locations, including bacteremia, head and neck infections, dental and orofacial infections, pneumonia and other infections of the thoracic cavity, intraabdominal and obstetric and gynecologic infections, bite wound and other soft tissue infections, and gangrene (i.e., clostridial myonecrosis). Organisms most commonly encountered in these infections include Bacteroides fragilis group, Prevotella spp., Porphyromonas spp., Fusobacterium nucleatum, Peptostreptococcus spp., and Clostridium perfringens.
Contamination of existing wound or puncture by objects contaminated with toxigenic Clostridium spp.
Tetanus (Clostridium tetani), gas gangrene (Clostridium perfringens and, less commonly, C. septicum, C. novyi, and others)
Ingestion of preformed toxins in vegetable- or meat-based foods
Botulism (Clostridium botulinum) and other clostridial food poisonings (C. perfringens)
Colonization of gastrointestinal tract with potent toxin-producing organism
Infant botulism (C. botulinum)
Person-to-person spread
Nosocomial spread of Clostridium difficile–induced diarrhea and pseudomembranous colitis; bite wound infections caused by a variety of anaerobic species
Pathogenesis and Spectrum of Disease
Organism
Virulence Factors
Spectrum of Disease and Infections
Clostridium perfringens
Produces several exotoxins; alpha-toxin, the most important, mediates destruction of host cell membranes; enterotoxin inserts and disrupts membranes of mucosal cells
Beta-toxin—cytotoxin
Gas gangrene (myonecrosis): Life-threatening, toxin-mediated destruction of muscle and other tissues after traumatic introduction of the organism.
Food poisoning: Caused by release of the toxin after ingestion of large numbers of the organism. Usually self-limiting and benign; manifested by abdominal cramps, diarrhea, and vomiting.
Enteritis necroticans (necrotizing enteritis; NEC): Life-threatening infection that causes ischemic necrosis of the jejunum. Often associated with immunocompromised patients (e.g., those with diabetes, alcohol-induced liver disease, or neutropenia). NEC, a gastrointestinal disease that causes bowel necrosis and inflammation, affects low-birth-weight, premature infants.
Clostridium sordellii
Produces a variety of bacterial proteases, phospholipases
Produces up to seven exotoxins, including lethal toxin (LT), hemorrhagic toxin (HT), and enterotoxins A, B, and C
Gas gangrene of the uterus as a result of abortion, normal delivery, or cesarean section.
Patient presents with little or no fever, lack of purulent discharge, hypotension, peripheral edema, and an increased white blood cell (WBC) count. Infection is typically fatal, and death is rapid.
Clostridium tetani
Produces tetanospasmin (TeNT), a neurotoxic exotoxin that disrupts nerve impulses to muscles
Tetanus (commonly known as lockjaw). Organism establishes a wound infection and elaborates TeNT, a potent toxin that mediates generalized muscle spasms. If the disease goes untreated, spasms continue to be triggered by even minor stimuli, leading to exhaustion and, eventually, respiratory failure.
Clostridium botulinum
Produces an extremely potent neurotoxin (BoNT)
Foodborne botulism: Results from ingestion of preformed toxin in nonacidic vegetable or mushroom foodstuffs. Absorption of the toxin leads to nearly complete flaccid (rag doll) paralysis of respiratory and other essential muscle groups.
Infant botulism: Occurs when the organism elaborates the toxin after it has colonized the gastrointestinal tract of infants (i.e., infant botulism).
Wound botulism: Occurs when C. botulinum produces the toxin from an infected wound site
Clostridium difficile
Produces toxin A (TcdA), an enterotoxin, and toxin B (TcdB), a cytotoxin
Both toxin A and toxin B are classified as large clostridial cytotoxins
The toxins glycosylate guanosine triphosphate (GTP) signaling proteins, leading to a breakdown of the cellular cytotoxin and cell death
Organism requires diminution of normal gut flora by the activity of various antimicrobial agents to become established in the gut of hospitalized patients. Once established, elaboration of one or more toxins results in antibiotic-associated diarrhea or potentially life-threatening inflammation of the colon. When the surface of the inflamed bowel is overlaid with a “pseudomembrane” composed of necrotic debris, white blood cells, and fibrin, the disease is referred to as pseudomembranous colitis.
Only strains producing toxin A or toxin B (or both) cause infections.
Actinomyces spp., including A. israelii, A. meyeri, A. naeslundii, and A. odontolyticus
No well-characterized virulence factors. Infections usually require disruption of protective mucosal surface of the oral cavity, respiratory tract, gastrointestinal tract, and/or female genitourinary tract
Usually involved in mixed oral or cervicofacial, thoracic, pelvic, and abdominal infections caused by patient’s endogenous strains.
Certain species (A. viscosus and A. naeslundii) also involved in periodontal disease and dental caries.
Identified in a variety of soft tissue infections, including perianal, groin, ancillary, breast, and periaural abscesses.
Propionibacterium spp.
No definitive virulence factors known
Associated with inflammatory process in acne.
Identified in systemic opportunistic infections, including endocarditis, central nervous system (CNS) infections, osteomyelitis, and arthritis.
As part of normal skin flora, the organism is considered the most common anaerobic contaminant of blood cultures and is often ignored.
Atopobium spp.
No definitive virulence factors known
Isolated from various infections in the genital tract, including bacterial vaginosis.
Considered normal flora of the female genital tract.
Bifidobacterium spp.
No definitive virulence factors known
Not commonly found in clinical specimens. Usually encountered in mixed infections of the pelvis or abdomen.
Eggerthella spp.
No definitive virulence factors known
Recovered from a variety of infections including intraabdominal and periabdominal infections.
Eubacterium spp.
No definitive virulence factors known
Usually associated with mixed infections of the oral cavity, abdomen, pelvis, or genitourinary tract.
Lactobacillus spp.
No definitive virulence factors known
Associated with advanced dental caries. Organism has also been identified in endocarditis and bacteremia.
Mobiluncus spp.
No definitive virulence factors known
Organisms are found in the vagina and have been associated with bacterial vaginosis, but their precise role in gynecologic infections is unclear. Rarely encountered in infections outside the female genital tract.
Bacteroides fragilis group, other Bacteroides spp., including B. gracilis and B. ureolyticus Prevotella spp. Porphyromonas spp.
Fusobacterium nucleatum and other Fusobacterium spp.
Anaerobic, gram-negative bacilli that produce capsules, endotoxin, and succinic acid, which inhibit phagocytosis, and various enzymes that mediate tissue damage.
Most infections still require some breach of mucosal integrity that allows the organisms to gain access to deeper tissues
Organisms most commonly encountered in anaerobic infections.
Infections are often mixed with infections caused by other anaerobic and facultative anaerobic organisms.
Infections occur throughout the body, usually as localized or enclosed abscesses, and may involve the cranium, periodontium, thorax, peritoneum, liver, and female genital tract.
May also cause bacteremia, aspiration pneumonia, septic arthritis, chronic sinusitis, decubitus ulcers, and other soft tissue infections.
The hallmark of most but not all infections is the production of a foul odor.
In general, infections caused by B. fragilis group occur below the diaphragm; pigmented Prevotella spp., Porphyromonas spp., and F. nucleatum generally are involved in head and neck and pleuropulmonary infections.
Finegoldia magna
Parvimonas micra
No definitive virulence factors known
P. micra has been shown to produce a variety of enzymes capable of tissue destruction, including collagenase, hemolysin, and elastase.
Most often found mixed with other anaerobic and facultatively anaerobic bacteria in cutaneous, respiratory, oral, or female pelvic infections.
Peptostreptococcus anaerobius
No definitive virulence factors known
Most often isolated from polymicrobic infections, including abscesses.
Veillonella spp.
No definitive virulence factors known
May be involved in mixed infections.
Organisms have been isolated in increasingly serious infections, including meningitis, osteomyelitis, endocarditis, bacteremia, and prosthetic infections.
Gram-Positive, Spore-Forming Bacilli

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Overview of Anaerobic Organisms