OBJECTIVES
1 Differentiate between conductive and sensorineural hearing loss and identify treatable causes
2 Compare and contrast the causes of otalgia, includng referred pain and lesions of the auricle, externa auditory canal, and middle ear.
3 Discuss the causes, diagnosis, treatment, and complications of acute and chronic otitis media with effusion. List indications for tympanocentesis, myringotomy, and tympanotomy tube placement
4 Classify tinnitus according to the etiology and specific type
5 Differentiate vestibular from nonvestibular causes of dizziness
6 Describe the common risk factors for and the appropriate workup of a patient with epistaxis
7 List the causes of nasal obstruction
8 List the indications for surgery in patients with acute sinusitis
9 Discuss the pathogenesis and medical treatment of chronic sinus disease
10 List the complications of sinusitis
11 Describe the more common congenital, inflammatory, and benign neoplastic disorders of the oral cavity and pharynx.
12 Identify malignant disorders of the oral cavity and pharynx, and discuss their treatment modalities
13 List the causes of hoarseness
14 Describe the classification and causes of stridor, and discuss the workup of a child with stridor
15 List the indications for cricothyrotomy and tracheostomy.
16 List the risk factors, workup, and three major treatment modalities of laryngeal cancer.
17 Describe the differential diagnosis, evaluation, and management of congenital, inflammatory, and neoplastic neck masses
Otolaryngology is the study of organ systems connected by the upper aerodigestive tract: the ear, vestibular system, cranial nerves, nose, paranasal sinuses, oral cavity, pharynx, larynx, esophagus, neck, and salivary and thyroid glands. These regions are critical for human interaction and communication, as well as functions rudimentary to sustain life (i.e., breathing and eating).
The disorders discussed in this chapter have a great impact on cost of health care and quality of life. More than 60% of all primary care visits for childhood illness and more than 50% of all adult primary care visits are for disorders of the ear, nose, and throat. Rhinosinusitis has the greatest financial impact to the economy of the United States through loss of job productivity and health care costs. The most common operation performed in the United States is placement of tympanic ventilation tubes.
THE EAR, THE VESTIBULAR SYSTEM, AND THE FACIAL NERVE
Anatomy
The ear is divided into the external, middle, and inner ear (Fig. 5-1). The external ear includes the auricle, which has a cartilaginous framework, and the external auditory canal, which is cartilaginous in one third of its lateral aspect and bony in two thirds of its medial aspect. The skin of the cartilaginous external canal contains hair follicles and the cerumen glands.

Figure 5-1 Cross section of the ear.
The middle ear is an air-containing space consisting of the eustachian tube, the tympanic membrane (ear drum), the middle ear cavity, the ossicular chain (malleus, incus, and stapes bones), the stapedius and tensor tympani muscles, and the mastoid sinuses (collections of air-containing sinusoids connecting to the middle ear cavity).
The inner ear consists of the cochlea, the semicircular canals, and the internal auditory canal. The inner ear is divided into the auditory and vestibular systems. These systems are composed of petrous bone, inside of which are tubular chambers that house delicate gelatinous and membranous structures submerged in fluid. Three types of sensory organ transducers are found in the inner ear: the organ of Corti (Fig. 5-2), located in the cochlea; the macula, located in the utricle and saccule; and the crista, located in the semicircular canals.

Figure 5-2 Cross section of the cochlea showing the organ of Corti.
The internal auditory canal, located on the posteromedial aspect of the temporal bone, houses cranial nerves VII (innervates the muscles of facial expression) and VIII (innervates the vestibular and cochlear portions of the inner ear). It also houses the nervus intermedius, which carries taste fibers from the tongue and parasympathetic secretomotor fibers from the brain stem to the sublingual, submandibular, and mucosal glands of the nose and palate and to the lacrimal glands. The facial nerve, lying just superior to the auditory portion of the eighth nerve in the internal auditory canal, runs from the pons in the brain stem through the middle ear cavity and the mastoid, innervating the stapedius, postauricular, and digastric muscles. It emerges from the stylomastoid foramen and goes through the parotid gland to innervate the muscles of facial expression (Fig. 5-3).

Figure 5-3 Anatomy of the facial nerve.
Physiology
The adnexal and ceruminous structures of the outer portion of the external auditory canal produce a waxy material that serves as a lubricant for the skin, a trap for foreign particles, and a protective barrier against microorganisms. Accumulation of cerumen or deformities of the ear canal may obstruct the canal to sound and can cause ineffective clearance of cerumen. Too little cerumen can cause irritation, inflammation, and infection of the canal.
The eardrum and the ossicular chain are responsible for conducting and amplifying the vibration of sound waves from the external auditory canal to the inner ear through the oval window.
Under normal conditions, the air-containing space of the middle ear is periodically inflated when swallowing or chewing; this momentarily opens the eustachian tube, which is normally closed, and allows equalization of negative pressure. The eustachian tube opens by the synergistic action of the tensor veli palatini (innervated by the third division of the fifth cranial nerve) and levator veli palatini (innervated by vagus) muscles. Under these normal conditions, the compliance and resonance of the tympanic membrane and the ossicles are optimal for conduction of sound waves to the stapes footplate. Failure of the middle ear space to remain properly inflated with air may result in the accumulation of secretory fluids (effusion), affecting compliance of the tympanic membrane and the ossicles; this change in compliance may result in a conductive hearing loss.
The inner ear houses three sensory organs (organ of Corti, macula, and crista) that contain hair cell transducers responsible for converting mechanical energy (vibratory, rotational, gravitational) into electrical energy.
Vibratory energy (sound pressure), producing movement of the stapes footplate, causes the propagation of complex waves traveling through the inner ear fluid in the cochlea, which in turn causes the basilar membrane to move up and down. The movement of the basilar membrane with respect to the overlying gelatinous tectorial membrane causes a shearing action, bending the stereocilia at the apical ends of the hair cells. This mechanical deformation triggers electrical energy in the form of nerve impulses emanating from the hair cells. This energy is transmitted to the central nervous system (CNS) through the auditory nerve, ultimately producing the sensation of sound. Each wave has an area of maximum displacement that correlates with the fundamental frequency of the sound that produced it. Hair cells are organized along the basilar membrane so that displacement by waves near the stapes (base of the cochlea) result in high-frequency perception, and waves at the other end (apex) result in low-frequency perception. The basilar membrane is thus said to have a tonotopic organization (Fig. 5-4).

Figure 5-4 Schematic representation of the cochlea unwound. The arrows represent the initial fluid shifts as the stapes vibrates. Notice the tonotopic organization of hair cells. High-frequency sounds stimulate the hair cells near the stapes. Low-frequency sounds stimulate hair cells near the apex or helicotrema.
Rotational acceleration of the head (i.e., turning the head) is interpreted by the semicircular canals, whereas linear acceleration (i.e., walking in a straight line) is perceived by the macula of the utricle and saccule. Hair cells are the basic element that transduces the mechanical forces to nerve action potentials in both systems, but their complex organization is different. Energy caused by rotation of the head produces shifts in the fluid of the semicircular canal; these fluid shifts jiggle the gelatinous-like cupulae (within which hair cell cilia are embedded). These jiggles cause a temporary deformation of the cilia, resulting in stimulation of the hair cells (Fig. 5-5). Energy from gravity or changes in linear acceleration produces movement of the utricular stone-like otoconia, resulting in temporary deformation of the cilia-like projections of the hair cells. These mechanical deformations trigger electrical energy in the form of nerve impulses emanating from the hair cells. This energy is transmitted through the superior and inferior vestibular nerves, ultimately producing the sensation of either rotation or acceleration.

Figure 5-5 Anatomy of the cristae. As the head rotates, fluid shifts within the semicircular canals in the opposite direction, displacing the cupula and stimulating the hair cells.
Vestibular input is but one of three systems (i.e., vestibular, ocular, proprioceptive) on which the body depends to maintain orientation in space. Under many circumstances one may be able to maintain relatively normal orientational function without simultaneous input from all three systems; however, denying visual input (eyes closed) or proprioceptive input (weightlessness) to vestibulopathic patients may significantly decrease a person’s ability to orient.
Vertigo is an interesting sensory phenomenon associated with the important relation between the input of the left and right vestibular systems into the CNS. If vestibular input is not symmetrical, it will result in discordant output, manifesting as vertigo, which is akin to a sensation of whirling in space. Vertigo is a hallucination of motion when objective motion does not exist. Because of the vestibular-ocular tracts, this fictitious motion produces a number of saccadic ocular tracking motions irrespective of visual input, referred to as nystagmus. This type of asymmetrical input may occur whenever an insult occurs to one rather than both inner ears. However, with time, the vestibular system, unlike the auditory system, is frequently able to compensate for asymmetrical input.
The facial nerve is the motor nerve for muscles of facial expression. When nerve dysfunction exists, paralysis of these muscles occurs; however, depending on the site of the paralyzing lesion, other subtle dysfunction may also be present, including loss of lacrimal secretions, contraction of the stapedial muscle, loss of submandibular or nasal secretions or both, loss of sensation in the floor of the mouth, and loss of gustation by the anterior tongue (Fig. 5-6).

Figure 5-6 Schematic diagram of the facial nerve. Notice how damage to the nerve at site A would result in loss of function distal to the lesion, but lacrimation and parotid salivation would be preserved.
If a facial nerve injury is severe, requiring significant regeneration, it is unlikely that normal anatomy will be reduplicated because certain nerve endings may not reinnervate the desired muscles. This aberrant reinnervation may cause very noticeable unintentional simultaneous contraction of multiple facial muscles (synkinesis) and mass movement during facial expression.
Physical Examination
Examination of the ear begins with observation of the auricle. The examiner looks at its shape and the condition of the skin and surrounding area.
The external auditory canal is examined by using an otoscope and the largest speculum that can fit in the ear. Pulling the pinna slightly away from the scalp makes the external canal straight and rigid for easier otoscope manipulation. The external auditory canal is observed for evidence of obstruction, otorrhea, or integumentary abnormality.
Cerumen should be carefully removed to allow adequate examination. A small amount of hard wax in the outer portion of the ear canal is best removed with a wire loop or a curette under direct vision through an otoscope. A large amount of soft wax is best removed by irrigation with warm water or peroxide if there is no perforation of the eardrum. Suctioning may also be used. Wax that is impacted against the tympanic membrane may need to be softened with peroxide drops or other over-the-counter, wax-dissolving agents (e.g., Debrox or Cerumenex) before irrigation or removal is attempted. Occasionally, the patient should be referred to an otolaryngologist for complete removal of the wax with special instruments under a microscope.
The tympanic membrane should be evaluated for deviation from its normal appearance of wax paper–like translucence (Fig. 5-7). In many ears, one can see portions of the ossicular chain (malleus, incus, stapes bones). The eardrum should be evaluated for thickness, opacification, inflammation, and abnormal deposits of materials (e.g., calcium). The presence of any unusually thin spots should be determined. Perforations larger than 1 mm are quite easily seen but are often mistaken for the retraction pocket commonly seen in the ears of patients with chronic dysfunction of the eustachian tube. The eardrum should also be observed for any evidence of middle ear fluid, which may cause a loss of translucency and a speckled light reflex on the eardrum, or may appear as air–fluid levels with bubbles in the middle air space. A pneumatic otoscope with a speculum large enough to completely occlude the ear canal is used to apply negative and positive pressure to the tympanic membrane to determine its freedom of movement, thus evaluating middle ear compliance.

Figure 5-7 The tympanic membrane landmarks.
During the course of the history and physical examination, the patient’s hearing can be grossly assessed by determining whether the patient is able to understand normal conversational speech, which is at 55 decibels (dB) and involves frequencies from 500 to 3,000 Hertz (Hz).
In addition to a standard cranial nerve examination, patients with vestibular complaints should undergo further neurologic examination. The patient is observed for spontaneous or induced nystagmus with position changes. Because disorientation complaints may result from dysfunction of vestibular, ocular, or proprioceptive systems, Romberg testing attempts to “sort out” the cause by removing ocular influence. The Romberg test involves measuring a patient’s ability to remain oriented in a standing position with eyes closed. Cerebellar testing (finger to nose, alternating hand test) is also helpful.
Evaluation
Hearing Loss
Although mixed hearing losses exist, the most common hearing losses are fairly pure (i.e., either conductive or sensorineural). Making this distinction and determining whether both ears are symmetrically affected are very important in simplifying the differential diagnosis. Table 5-1 categorizes some of the causes of hearing loss as they relate to the inner, middle, or outer ear.

As the term conductive hearing loss suggests, patients with this loss have inadequate means of properly conducting sound to the inner ear. This could be produced by any disorder related to the external auditory canal (occlusion), tympanic membrane (large perforation), middle ear space (effusion), or ossicles (disruption). This defect produces a loss of amplification, which may be described as “the volume being turned down too low.” The patient with bilateral conductive hearing loss may actually hear better in the presence of background noise, such as at large social gatherings, because people with normal hearing must characteristically “turn up the volume” of their conversation in an effort to overcome the high volume of background noise generated by all of the competing conversations.
In contrast, however, the most common complaint of the patient with bilateral sensorineural hearing loss is difficulty hearing and understanding in large gatherings. Patients with sensorineural hearing loss generally have a distaste for loud music and loud conversation, which add further distortion and discomfort to their already ailing ears. Unilateral hearing loss commonly implies a local cause rather than a diffuse, systemic cause. The clinician must always be concerned about asymmetrical disease in symmetrical organs (i.e., the clinician should wonder if a lesion or neoplasm is responsible).
Tuning fork tests help the clinician differentiate between conductive and sensorineural hearing loss. These tests are most helpful when the hearing loss type is pure (conductive or sensorineural, not mixed) and unilateral. The Weber test is performed with a vibrating 512-Hz tuning fork, placed centrally on the forehead or on the maxillary teeth. The patient is asked whether the sound is heard better in one ear or in the center of the head. If the patient hears the sound better in one ear, either a greater sensorineural hearing loss exists in the contralateral ear or a conductive loss is present in the ipsilateral ear. A conductive loss masks background sounds, resulting in enhanced body and skull sounds. With the Rinne test, the patient is asked to determine whether the tuning fork is heard louder when it is placed on the mastoid bone or when it is held approximately 2 cm from the external canal. A patient with normal hearing or with sensorineural hearing loss will hear the tuning fork better when it is placed adjacent to the ear canal. A patient with a significant conductive loss will hear the tuning fork better when it is placed on the mastoid bone, because air-conducted sounds are masked and skull sounds are enhanced.
Pure tone audiometry qualifies hearing loss according to frequencies, allocating and measuring the amount of loss according to sensorineural and conductive mechanisms. It does not assess speech recognition or discrimination. Pure tone audiometry is performed by presenting a series of variable-intensity tone pips (“beeps”) via earphones at six or more frequencies (250, 500, 1,000, 2,000, 4,000, and 8,000 Hz), to which the patient volunteers a response. The threshold is the lowest intensity of stimulus that the patient is able to hear. The zero-dB line on the audiogram is considered normal, and the patient’s hearing levels are recorded as dB above or below the zero-dB point along each of the six frequencies.
A hearing threshold of 0 to 20 dB represents normal hearing; 25 to 40 dB, a mild loss; 40 to 70 dB, a moderate loss; 70 to 90 dB, a severe loss; and greater than 90 dB, a profound loss. Sensorineural hearing loss is determined by obtaining bone conduction thresholds. The tone pips (“beeps”) are delivered to the cochlea by placing a soundgenerating device on the mastoid bone. This, in effect, bypasses the external and middle ear, thus giving a set of bone-conduction scores at each frequency for each ear. Conductive hearing loss thresholds are measured by first delivering the “beeps” through the air via earphones. Sound stimuli delivered in this way must traverse the outer, middle, and inner ear to be heard, thus giving a set of air-conducted scores for each ear. These air-conducted scores are then compared to bone-conducted scores (see above). If the scores match, no conductive hearing loss exists; if the air scores are worse than the bone scores (resulting in an “air–bone gap”), a conductive hearing loss equaling the size of the air–bone gap is present (Fig. 5-8).

Figure 5-8 Examples of pure-tone audiograms of the left ear only. A, Normal hearing (normal air scores = normal bone scores). B, Conductive hearing loss (abnormal air scores and normal bone scores, indicating an air-bone gap). C, Sensorineural hearing loss (abnormal air scores = abnormal bone scores). D, Mixed or combined sensorineural and conductive hearing loss (abnormal air scores are worse than abnormal bone scores, indicating a conductive hearing loss [note air-bone gap] superimposed on a sensorineural hearing loss). Lower limits of normal hearing are about 20 dB.
The speech reception threshold probably correlates best with one of the most important communication skills: understanding spoken words. This test measures how loud the tester must speak to be understood by the patient. The speech discrimination evaluation, however, requires the patient to discern certain phonetically balanced words from other words (e.g., live, dog, love, girl, bath, dead, boy, die, ball, ride). This ability should be nearly perfect for people with normal hearing and for those with conductive hearing loss. Pathology of the cochlea, the auditory nerve, or the CNS, however, causes perceptual distortion and thus impairment in speech discrimination.
With electrophysiologic audiometry, the audiologist must interpret an involuntary or reflexive physiologic response. One of the most useful electrophysiologic tests, the brain stem auditory evoked response (BAER) test, also known as the auditory brain stem response (ABR) test, measures the electroencephalographic responses to sound stimuli. Another useful electrophysiologic test is the evoked otoacoustic emissions (EOAE) test. EOAEs are sounds emitted by the cochlea in response to acoustic stimulation. The hearing of neonates, young children, and patients who are comatose, mentally retarded, or otherwise unreliable is assessed with these techniques, because no volitional response is required.
Tympanometry measures the function of the eardrum with a multichannel probe (containing a speaker, a microphone, and a transducer) that fits into the ear canal. The transducer produces pressure changes from 400 mm H2O of negative pressure to 200 mm H2O of positive pressure, while the speaker delivers low-frequency sound. The microphone senses the amount of sound energy reflected and records it on a tracing. Based on the configuration of the tympanogram, inferences can be made about the function of the middle ear, the presence or absence of fluid, and the presence of a perforation (Fig. 5-9).

Figure 5-9 Typical patterns obtained with tympanometry. A, Peak efficiency occurs with no pressure manipulation. B, Often referred to as a flat tympanogram; peak efficiency is not realized at any tympanic position, suggesting fluid in the middle ear (effusion), perforation of the tympanic membrane, or occlusion of the external ear canal. C, Peak efficiency occurs only when the position of the tympanic membrane is manipulated outward, suggesting that its resting position is retracted, as would be seen with negative pressure in the middle ear space caused by poor aeration.
Otalgia
Most causes of earache are easy to identify; however, because of the complex sensory innervation of the ear and the temporal bone, pain from many other sources may be referred to the ear and mistaken for ear pathology. In addition to the obvious examination of the ear, the upper aerodigestive tract should be examined because pain at this site is frequently referred to the ear. Queries about exacerbating factors may be helpful. Increased otalgia on chewing, a history of temporomandibular joint (TMJ) trauma, or recent dental work points to the myofascial structures of the TMJ. Tenderness in these areas may be confirmatory in the absence of other physical findings (Table 5-2).

Tinnitus
Tinnitus is “ringing” or some other perceived noise in the ears. It usually occurs in the absence of an objective acoustic stimulus from the outside environment. The very nature of the sound is key to making a diagnosis. Pulsatile tinnitus is usually vascular in origin. Cochlear injury produces a continuous noise that may vary in intensity with background noise or the time of day. Unilateral tinnitus infers pathology of the cochlear end-organ or its nerve, whereas bilateral tinnitus may be from a systemic toxicity or binaural injury. When the onset is acute, other signs of labyrinthine injury (e.g., vertigo, hearing loss, or facial weakness) should be sought. Patients with tinnitus need immediate attention because they may have a pathology that is reversible with early treatment (Table 5-3). Unfortunately, no medications have as yet proved effective in treating tinnitus.

Otorrhea
Drainage from the ear can be of many different consistencies. Thin, watery, yellow-to-clear fluid may be nothing more than bath water mixing with cerumen if the examination reveals normal ear structures. However, when trauma has occurred, a cerebrospinal fluid (CSF) fistula must be considered. A mucoid and purulent discharge from the ear implies infection. Carefully cleaning the ear may reveal a long-standing perforation, an acutely inflamed tympanic membrane and middle ear, or evidence of squamous debris and retraction consistent with otitis media. Bloody discharge may be part of an infectious process, but trauma and neoplasm must also be considered. High-resolution computed tomography (CT) scans of the temporal bone will provide evidence of bony destruction; however, the usefulness of these scans is limited because the discharge will appear with the same density as soft-tissue defects (e.g., polyp, cholesteatoma, tumor).
Vertigo
Dizziness is a common symptom but is usually not otologic in origin. Spinning or whirling vertigo, on the other hand, such as is felt immediately after being spun around or with the nausea of motion sickness, should be distinguished from “light-headedness.” Cardiac history, symptoms or findings of orthostatic hypotension, changes in blood pressure medications, or past history of cerebrovascular accident may point to decreased blood flow in the vertebrobasilar system. Complete neurologic examination may point to other CNS findings, especially those of cerebellar pathology. The presentations of these conditions may be identical to those of labyrinthine pathologies (Table 5-4).

Electronystagmography (ENG) takes advantage of the predictable saccadic eye movements (nystagmus) that accompany various types of stimulation of the semicircular canal. Periorbital electrodes are used to precisely sense and record nystagmus; cooling, warming, and head rotation techniques are used to stimulate the semicircular canals. The quantitated nystagmic response can thus be used to measure the integrity of the vestibular system.
Platform posturography alters a patient’s visual and proprioceptive feedback to isolate the vestibular system’s singular impact on the patient’s orientation abilities. In this test, the patient is harnessed inside a chamber that systematically eliminates visual feedback, thus altering the patient’s visual surroundings and proprioceptive feedback by eliminating platform stability.
Clinical Presentation, Diagnosis, and Treatment
Congenital Anomalies
During embryologic development, six small hillocks of cartilage (which arise from the first and second branchial arch) eventually fuse to form the pinna. Failure to complete proper embryologic development results in formation of cysts or sinus tracts in the pinna and the preauricular area. If these tracts become recurrently infected, they can be easily resected. More significant anomalies of the first branchial cleft and pouch may lead to marked deformities or absence of the auricle, the external auditory canal, and the middle or inner ear structures. The most important interventions are early audiometric assessment and early placement of hearing aids, preferably within the first year of life. Later, the series of surgical reconstructions of the pinna, the external ear canal, and perhaps the middle ear can begin.
Ear Trauma
Auricular hematoma is caused by a blunt shearing injury that separates the auricular cartilage from the perichondrium, creating a space in which blood and fluid can collect. This collection of fluid eventually forms scar tissue and results in a “cauliflower ear” deformity. This fluid must be evacuated and the skin must be compressed to the cartilage for several days to prevent its reaccumulation.
Frostbite and burns of the ear produce injury that is not fully manifested until days later. It is important to debride eschar conservatively, to keep all exposed cartilage moisturized, to avoid pressure on affected areas, and to control infection topically.
Perforations may develop from previous otitis media. Approximately 90% of traumatic tympanic perforations heal uneventfully. Those that do not heal spontaneously are usually large or have edges curled in such a way that regrowth will not occur. If healing is not evidenced within several months, a tympanoplasty using a temporalis fascia graft is indicated to close the perforation. This procedure is more successful in the absence of recurring otitis media.
Fractures of the base of the skull may traverse the temporal bone and damage the vestibular or auditory mechanisms or both. Classically, two types of fractures are described, depending on location of the fracture in relation to the petrous portion of the temporal bone (Table 5-5): longitudinal and transverse. Longitudinal fractures are far more common, resulting in about 85% of all temporal bone fractures (Fig. 5-10). Physical findings may include hemotympanum, otorrhea containing CSF and blood, hearing loss, and nystagmus. Rarely, a fracture may affect the cochlea or the facial nerve. Balance disturbances and varying degrees of hearing loss may be observed. Ossicular disruptions may need surgical repair. Significant sensorineural hearing loss rarely recovers, but the vestibular system can compensate over a period of months.


Figure 5-10 Classification of temporal bone fractures. Dotted lines represent the axis of the petrous portion of the temporal bone. Fracture A depicts a longitudinal fracture, whereas Fracture B represents a transverse fracture.
Otitis Externa
The skin of the auricle and the external auditory canal is subject to most of the common dermatologic diseases and to some that are unique to the external ear. The most common infectious disease is otitis externa, which can be localized or diffuse. Localized otitis externa (folliculitis of the external auditory canal) may be caused by trauma (commonly from a fingernail or a hairpin). It produces pain out of proportion to findings on physical examination, which may range from a small red spot to a fluctuant swelling. The patient will complain of extreme pain when the ear is moved or the area is touched. Treatment involves antistaphylococcal antibiotics, drainage, or both.
The term otitis externa usually refers to a diffuse process that involves the entire external auditory canal. It is also known as swimmer’s ear because moisture remaining in the external canal after swimming or showering may lead to this infection. Trauma to the delicate skin of the canal or exposure to purulent middle ear discharge through a perforation may initiate otitis externa. The most common causative agent is Pseudomonas, but Klebsiella, Streptococcus, and Staphylococcus are also frequently implicated. Fungus may appear, but usually as a secondary growth on desquamated epithelium. Findings range from minimal inflammation and tenderness to complete closure of the ear canal, with surrounding cellulitis and adenopathy.
Management involves removing debris from the external auditory canal so that topical ear solutions effective against Pseudomonas, Staphylococcus, Candida, and Aspergillus may reach the site of the infection. If the ear canal is so swollen that ear drops cannot be instilled, a small wick is placed into the external auditory canal. With the wick in place, the patient is instructed to use ear drops 2 to 4 times daily for several days. During the course of management, debris should be frequently removed from the patient’s ear canal. If there is marked cellulitis or inflammation involving the auricle and the tissues around the ear, systemic antibiotics and steroids are generally effective. Some patients may require hospitalization for treatment with intravenous antibiotics. Pain is a very significant part of the complex of symptoms and narcotic analgesia is often required.
Necrotizing otitis externa, once called malignant otitis externa, is an osteomyelitis of the temporal bone and skull base. The most common offending organism is Pseudomonas aeruginosa, but Proteus and Klebsiella may also be involved. Mortality is high. Patients at risk are those with simple otitis externa who have diabetes or those whose immune system is compromised. The patient develops persistent inflammation of the external auditory canal, persistent pain, and granulation tissue in the ear canal, often with exposed bone and cranial nerve involvement. This infection does not respond to topical therapy. Aggressive treatment with topical and systemic antibiotics over several months is mandatory. Surgical debridement may be helpful in very early cases. To prevent this condition, patients not responding to routine treatment of otitis externa must be referred early to the otolaryngologist.
Foreign bodies in the external ear canal are unfortunately all too common among preschool children. Fortunately, foreign bodies in the ear do not usually represent an emergency unless the object is caustic. However, all such foreign bodies, whether a soon-to-swell popcorn kernel, a bean, a toy bead, or a trinket, are somewhat difficult to remove. Children will usually allow physicians only one good try; if the attempt is unsuccessful, general anesthesia will almost certainly be required. In the meantime, the use of ear drops containing corticosteroids is prudent.
Otitis Media
Most of the infectious or inflammatory disease processes involving the middle ear space result from dysfunction of the eustachian tube. When the eustachian tube does not open frequently enough to allow equalization between the pressure in the middle ear and that of the atmosphere, a vacuum is created, and oxygen and nitrogen are absorbed into the mucous membranes of the middle ear and the mastoid air cell systems. The consequence is either increased capillary permeability and glandular activity with resultant middle ear effusion, or retraction of the tympanic membrane with possible adherence to the ossicles and the medial wall of the middle ear space. If infectious agents are present, the transudate forms an ideal culture medium, leading to otitis media.
Acute otitis media (AOM) is the most common infection for which antibacterial agents are prescribed for children in the United States. It is defined by a history of acute onset, the presence of middle-ear effusion, and signs and symptoms of middle-ear inflammation. By their second birthday, 75% percent of all children will have had at least three episodes of acute otitis media. The organisms that most commonly cause acute otitis media are Streptococcus pneumoniae, Moraxella catarrhalis, and Haemophilus influenzae. A typical history is onset of pain in one or both ears associated with behavioral changes, including crying, and often occurring in conjunction with an upper respiratory tract infection. Rarely, signs of meningeal irritation are present. Examination shows the eardrum to be red or opaque and possibly bulging, with a loss of normal landmarks secondary to an inflamed and often fluid-filled middle ear. Occasionally, infection results in a rupture of the tympanic membrane before a physician examines the child.
In 2004, the American Academy of Pediatrics (AAP) published updated guidelines for the management of AOM in an attempt to prevent unnecessary use of antibiotics, which can lead to bacterial resistance. If symptoms are not severe or diagnosis is unclear, initial observation only should be performed. The patients should be reevaluated in 48 to 72 hours. If antibiotics are used, then high-dose amoxicillin (90 mg/kg/day) should be used first. Azithromycin, clarithromycin, or erythromycin can be used if a penicillin allergy is present. After therapy is initiated, the pain usually resolves within 3 days and normal eustachian tube function usually returns in 2 weeks. If infection persists after 3 days of antibiotic therapy, then the antibacterial agent should be changed (high-dose amoxicillin–clavulanate). If this fails, a 3-day course of parenteral ceftriaxone should be used. Patients should be followed until the middle ear space is clear, because approximately 10% of children will have persistent effusions for more than 10 to 12 weeks. Some patients might develop recurrent AOM, which is characterized by recurrent episodes of infection despite multiple rounds of antibiotics. Patients who experience six episodes of AOM in a 6-month period are considered candidates for tympanostomy tube placement. This allows direct access to the middle ear space so that topical antibacterial drops may be administered.
Untreated acute otitis media can progress to acute mastoiditis, meningitis, brain abscess, facial nerve paralysis, and labyrinthitis. Drainage was standard therapy in the preantibiotic era; however, tympanocentesis is now infrequently indicated (Table 5-6). The procedure allows the infection to drain as well as material to be obtained for culture.

Otitis media with effusion (OME) is the second most common middle ear disease, with an estimated 2.2 million diagnoses annually in the United States. OME refers to fluid in the middle ear without signs or symptoms of an infection. Tympanometry is useful in its diagnosis. OME may occur spontaneously because of poor eustachian tube function or as an inflammatory response following AOM. The eustachian tubes of children are smaller and more horizontal in orientation than those of adults, thus restricting their ability to open. The function of the eustachian tube is impaired by edema of nasopharyngeal or eustachian tube mucosa caused by infection, allergy, tonsilloadenoidal hypertrophy, nasopharyngeal neoplasm, or cleft palate. Risk factors for OME are listed in Table 5-7.

The AAP also published updated guidelines for the management of OME in 2004. It is a self-limiting disease and initial observation only is recommended unless hearing loss or speech deficit is suspected. Antibiotics, antihistamines, decongestants, and steroids have been shown to have no benefit. Seventy-five to 90% of cases resolve on their own by 3 months. If the eustachian tube does not begin to function, the persistent effusion may create a significant hearing loss. This type of hearing loss can result in language delay and possibly in a learning disability. If fluid persists for more than 3 months despite treatment, myringotomy with placement of middle ear ventilation tubes should be considered. Ventilation tubes allow the middle ear to aerate, reducing the accumulation of fluid and restoring normal conductive hearing. An incision is made in the tympanic membrane and a tube is placed within the incision to maintain this controlled tympanic membrane perforation.
Some patients with chronic dysfunction of the eustachian tube will experience chronic otitis media associated with a nonhealing, chronically inflamed, draining perforation of the tympanic membrane. The middle ear and mastoid mucosa also will be involved and over time may be associated with all of the destructive complications seen in acute otitis media. Treatment is surgical, usually consisting of a combination of tympanoplasty (repair of the ear drum) and mastoidectomy (opening the multiple mastoid air cells into one space).
Cholesteatoma
Cholesteatoma is a skin-lined, keratin-producing middle ear cyst that probably originates from a diseased tympanic membrane. Cholesteatoma tends to develop in a setting of chronic dysfunction of the eustachian tube and chronic negative pressure in the middle ear, resulting in chronic retraction of the tympanic membrane. This retraction produces a cystic, keratin-producing “pocket” of tympanic membrane. These fluid pockets are frequently infected and produce a foul otorrhea. Osteolytic enzymes in the basement membrane of the cholesteatoma produce osteonecrosis. The ossicular chain, the facial nerve, the cochlea, the semicircular canals, and the skull base may be infected and destroyed by this process. A patient with cholesteatoma commonly has chronic and recurrent infections with hearing loss. Facial nerve paralysis, vertigo, or intracranial abscesses may be seen. The pocket of whitish, cheese-like squamous debris inside the cyst may be seen, and the middle ear mucosa is inflamed and often edematous and polypoid, even protruding through a perforation. Surgical excision is necessary and may include a mastoidectomy and removal of the involved ossicles to prevent complications.
Otosclerosis is a spontaneous abnormality of the middle ear and occasionally the inner ear. This abnormality is most common in young adults, and it causes an acquired hearing loss. A small focus of spongy vascular bone involves a part or all of the stapes footplate. The result is fixation of the stapes footplate, with a conductive hearing loss. If the cochlea becomes involved, an additional sensorineural hearing loss is produced. Otosclerosis occurs among both men and women, has a genetic predisposition, and may accelerate during pregnancy. A hearing aid may be used to amplify sound for affected patients. Most patients, however, prefer surgical replacement of the fixed stapes footplate by a prosthesis. Infrequent complications include complete loss of hearing in the involved ear or severe postoperative dizziness.
Sensorineural Hearing Loss
Hearing loss affects 1 in 2,000 infants and may be either genetic (usually with a recessive mode of inheritance), developmental (anomalies affecting the temporal bone and the cochleovestibular apparatus), infectious in utero (cyto-megalovirus, rubella, syphilis, herpes, toxoplasmosis), or associated with other perinatal factors (meningitis, severe jaundice, prematurity, hypoxia, ototoxic drugs). Early identification is imperative and rehabilitation through language interventions, hearing aids, cochlear implants, or other assistive listening devices may maximize the child’s communication skills.
Acquired hearing losses may result from aging, noise exposure, exposure to ototoxicants, and disease processes of the ear and the CNS. Presbycusis, or the hearing loss of aging, results from degeneration of the cochlea. By the age of 80, 75% of people are affected. Exposure to noise in excess of 90 dB, especially if prolonged, may injure the cochlear hair cells, causing a localized loss in the mid- to high-frequency level of 3,000, 4,000, and 6,000 Hz. This loss may be caused by a sudden loud noise, such as a gunshot blast, or by prolonged exposure to industrial or recreational noise, such as factory noise or loud music. Patients should be counseled on the use of noise protection during such activities. Damage to cochlear and vestibular hair cells by toxic levels of aminoglycosides has been well described. Other medications that can cause cochlear dysfunction are cisplatin, vancomycin, loop diuretics, and antimalarial agents. Erythromycin and aspirin can cause a reversible sensorineural hearing loss. Patients will frequently complain of tinnitus and trouble hearing in the presence of background noise. Wearing hearing aids or assistive listening devices and optimizing the listening environment are usually helpful.
Vestibular Pathology
When the vestibular system is disrupted, problems ranging from imbalance to disabling vertigo are produced. As with sensorineural hearing loss, the causes vary.
Vestibular neuritis (previously incorrectly called viral labyrinthitis) is probably a viral inflammation involving the vestibular nerve or the vestibular neuroepithelium. The condition is characterized by the acute onset of severe vertigo, which lasts for a few days and gradually resolves over several weeks. It may be preceded by a viral upper respiratory tract condition. Treatment is supportive and symptomatic, consisting of bed rest and drugs that suppress vertigo (e.g., meclizine).
Like the cochlea, the vestibular apparatus is subject to the degenerative process of aging. Patients with such disequilibrium are elderly and somewhat frail; they usually show evidence of sensorineural hearing loss (presbycusis) and complain of vertigo induced by changing positions. These patients should be advised to move carefully and slowly; some labyrinthine sedation (e.g., meclizine, diazepam) may be prescribed.
Benign positional vertigo is an acute and rather severe vertigo lasting only a few minutes. The vertigo is reproduced by specific positioning of the head. The condition is believed to be caused by particulate matter in the endolymph of one of the semicircular canals. The episodes will subside after several months. Severe persistent disease may respond to head positioning maneuvers or vestibular destructive procedures.
Ménière’s disease, or endolymphatic hydrops, causes episodic hearing loss, incapacitating vertigo lasting for several hours, tinnitus, and a sensation of aural fullness. This disease is usually unilateral and is associated with bulging or rupture of Reissner’s membrane (Fig. 5-2) and mixing of endolymphatic fluid with perilymphatic fluid; this mixture is toxic to vestibular and cochlear hair cells. Medical treatment consists of a low-salt diet, diuretics, and, under certain circumstances, allergy therapy. Surgical decompression of the endolymphatic sac or destruction of the nerves of the inner ear or vestibule is reserved for incapacitating vertiginous symptoms that do not respond to medical treatment.
Diseases of the Facial Nerve
Pathology in many different locations affects the functioning of the facial nerve because of its long circuitous course (see Fig. 5-6). In general, the prognosis for recovery of facial nerve function is good if the paralysis is incomplete or caused by reversible infection or inflammation. The prognosis is frequently poor if the paralysis is long-standing or caused by cancer or trauma of the temporal bone. See Table 5-8 for a listing of diagnoses.
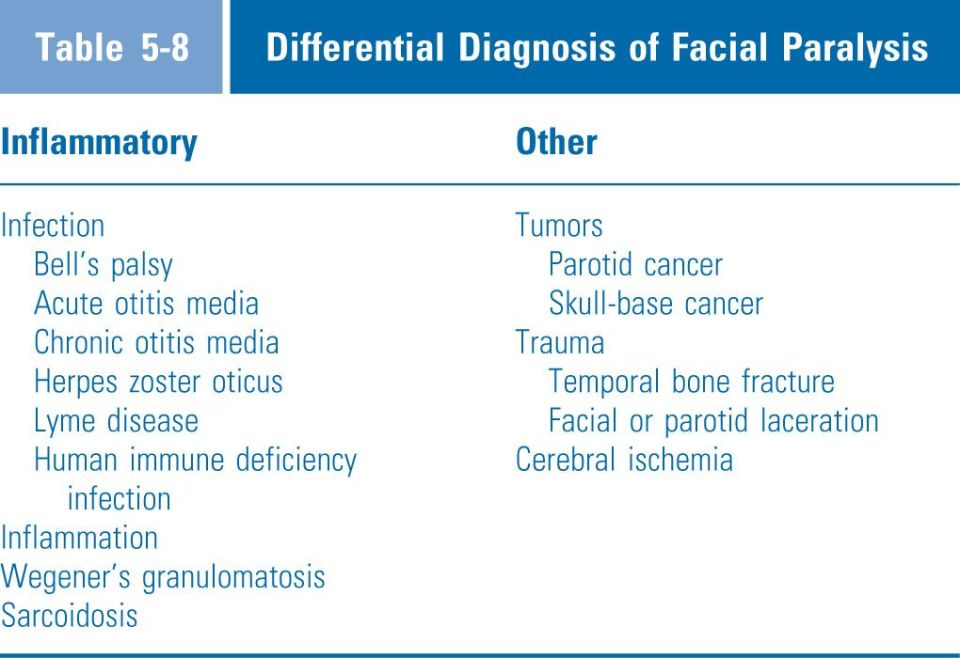
The most common process producing paralysis is idiopathic or Bell’s palsy. Viral infection of the nerve with herpes simplex is supported by polymerase chain reaction analysis. The paresis develops in a matter of hours and may progress to complete paralysis, often with associated mastoid pain, over a period of several days. Most cases resolve spontaneously, but treatment with corticosteroids and acyclovir is recommended. Persistent paralysis warrants imaging studies to rule out the presence of a tumor.
Other infectious or inflammatory diseases known to be associated with facial paralysis include acute otitis media, chronic otitis media, herpes zoster oticus, Lyme disease, HIV infection, sarcoidosis, and Wegener’s granulomatosis. Treatment is generally medical and should be directed at the underlying disorder. Facial paralysis caused by otitis media should be treated with wide myringotomy and with topical and systemic antibiotics.
Supranuclear lesions of the facial nerve, such as are seen in cerebrovascular ischemia, will frequently spare dysfunction of the upper facial nerve branches to the forehead because these branches are connected to both crossed and uncrossed corticobulbar fibers.
Penetrating and blunt injuries involving the side of the face, the ear, or the temporal bone may affect the facial nerve. When the main trunk or one of the branches of the nerve is involved, paralysis of the muscles supplied by that portion of the nerve may be seen. Transection of the nerve should be treated by reanastomosis or nerve grafting.
Facial paralysis significantly affects appearance; however, the most serious side effect is an ipsilateral exposure keratitis caused by inability to close the upper eyelid. If ignored, this keratitis may lead to corneal scarring and marked impairment of vision. To protect the eye, the application of artificial tears, ointment, and tape (to keep the eye closed while sleeping) is recommended. A tarsorrhaphy or the implantation of a gold weight in the upper eyelid to allow better coverage of the cornea may be required.
Otolologic Neoplasms
Because the skin of the external ear receives as much exposure to ultraviolet light as skin on any other area of the body, it is subject to the usual ultraviolet-light–induced skin neoplasms. Actinic keratosis is the most common such condition. Benign neoplasms unique to the external auditory canal are osteomas and exostoses. Exostoses present as smooth, hard nodules, usually occurring multiply and bilaterally. Osteomas are single and unilateral. If either of these produces marked obstruction or prevents the ear from cleaning itself naturally, surgical excision is indicated. Of the malignant lesions, squamous cell and basal cell carcinomas, as well as malignant melanomas, are the most common. Surgical excision is usually the best treatment, although radiation therapy may also be useful.
Neoplasms of the middle ear and the mastoid are extremely rare. Glomus tympanicum is a very vascular paraganglioma of the middle ear. It is histologically similar to glomus tumors of the carotid body, the vagus, and the jugular bulb. Patients classically complain of unilateral pulsatile tinnitus (Table 5-3) and hearing loss. A reddish tumor mass may be visible beneath an otherwise normal, translucent eardrum. Surgical excision is the best treatment.
Neoplasms of the inner ear are an unusual but important cause of unilateral sensorineural hearing loss. The most common tumor, acoustic neuroma, is a benign intracranial tumor of the eighth cranial nerve. The peripheral tissues in the CNS usually accommodate slow tumor expansion, giving rise to early ear symptoms and late central symptoms. As would be expected with a lesion of the eighth nerve, the hallmark symptom is unilateral sensorineural hearing loss with poor word discrimination, usually accompanied by tinnitus. Late symptoms are severe vertigo, facial nerve paralysis, and ataxia. Magnetic resonance imaging (MRI) is diagnostic, and surgical excision or stereotactic radiosurgery are the treatments of choice.
NOSE AND PARANASAL SINUSES
Anatomy
The external dorsal structures of the nose are formed by a bony and cartilaginous framework covered externally by skin and facial muscles. The upper one third, or bony vault, of the nose consists of the paired nasal bones supported by the frontal process of the maxilla and the nasal process of the frontal bone. The cartilaginous framework consists of the upper lateral cartilages, which are fused to the septal cartilage medially and the lower lateral (alar) cartilages (Fig. 5-11).

Figure 5-11 Anatomy of the nasal vault.
The nasal cavity extends from the anterior nares to the posterior choanae and is divided by the nasal septum into two chambers. The nasal valve, located in the anterior nasal cavity, is composed of the inferior turbinate erectile tissue, the septum, and the upper lateral cartilages. This is often the narrowest area of the adult upper airway. Common causes of nasal obstruction occur here, such as a deviated septum or enlarged turbinates due to allergies. The roof of the nose is formed by the cribriform plate of the ethmoid bone. The lateral wall of the nasal cavity is configured by three overhanging scroll-like bones. These turbinates subdivide the lateral nasal wall into a corresponding meatus or opening. Drainage from the nasolacrimal duct passes into the nose through the inferior meatus. The anterior ethmoid, maxillary, and frontal sinuses open into the middle meatus (Fig. 5-12). The region containing the anterior ethmoid sinus and the middle meatus is known as the osteomeatal complex. Obstruction here is a common cause for sinus congestion as the maxillary, anterior ethmoid, and frontal sinuses can all be affected. The posterior ethmoid cells drain into the superior meatus, and the sphenoid sinus opens into the sphenoethmoid recess, which is located immediately above and behind the superior turbinate.

Figure 5-12 The anterior ethmoid sinus–middle meatus region (osteomeatal complex) in the coronal projection. On the patient’s right, the middle meatus (four stars) receives drainage from the ethmoid bulla (B) and other anterior cells. Secretions from the frontal sinus (F) must pass through the ethmoidal regions, and maxillary sinus (M) secretions must pass through the ostium and the infundibulum (A) before reaching the middle meatus. The situation after functional endoscopic ethmoidectomy is shown on the patient’s left. The uncinate process (U) has been removed, the anterior ethmoid cells opened, and the natural ostium of the maxillary sinus widened. The middle turbinate (C) is left intact. Also shown is the inferior turbinate (D).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


