Acquired nonclonal myelodysplasia (NMD) is undoubtedly underrecognized. It closely mimics constitutional hematopoietic disorders and clonal myelodysplastic syndromes and may easily be mistaken for them. NMD is frequently reversible with time and appropriate therapy. A wide array of underlying conditions is associated with NMD (Table 16.1 and Figs. 16.1, 16.2and 16.3).
Age is directly associated with an increase in dyserythropoiesis and dysgranulopoiesis, as individuals get older (1).
Aromatic hydrocarbons include benzene, toluene, xylene, and ethylbenzene. These substances are primarily found in a work environment. Benzene causes a unique type of dysplasia characterized by marked dyserythropoiesis, eosinophilic dysplasia, and abnormal cytoplasmic granulation in neutrophil precursors (2). Other effects of benzene include anemia, leukopenia, aplastic anemia, clonal T-cell expansion, hemophagocytosis, stromal degeneration, and marrow hypoplasia.
Cigarette smoking is associated with dyserythropoiesis and a slight increase in bone marrow blasts (see Fig. 16.1) (3). Other hematopoietic changes include erythrocytosis, neutrophilia, increased immature granulocytes, and histiocytic hemophagocytosis.
Erythroid hyperplasia and ineffective erythropoiesis are relatively common causes of dyserythropoiesis. Examples of underlying disorders include thalassemia and hemolytic anemia.
Arsenic intoxication causes myelodysplastic changes proportionate to the amount and duration of ingestion (4, 5, 6, 7, 8, 9, 10). In arsenic poisoning, the peripheral blood may show anemia with coarse basophilic stippling and macro-ovalocytes, leukopenia, granulocytopenia, eosinophilia, and reticulocytopenia. The bone marrow is hypercellular with megaloblastic change, trilineal myelodysplasia, and increased karyorrhexis.
Lead poisoning can be acquired from folk medications, illegal whiskey, and environmental contamination (11). The peripheral blood shows anemia with coarse basophilic stippling, reticulocytosis, and karyorrhectic nucleated red blood cells. The bone marrow shows erythroid hyperplasia, marked dyserythropoiesis, and increased karyorrhexis.
Carcinoma has been associated with acquired myelokathexis (12). The differential diagnosis includes constitutional myelokathexis (see Chapter 4) and myelodysplastic syndrome with myelokathexis (13).
Copper deficiency, whether primary or secondary to zinc excess, causes anemia with anisocytosis and abnormal red blood cell morphology, consistent with sideroblastic anemia (14). Neutropenia is also found. The bone marrow shows hypocellularity, dyshematopoiesis with ringed sideroblasts, erythroid and granulocytic precursors containing cytoplasmic vacuoles, and osteoporosis. Neurologic impairment resembling that seen in vitamin B12 deficiency may occur. Copper deficiency occurs in Menkes syndrome, dietary copper deficiency, and inadequate copper in parenteral nutrition formulas. Zinc excess may be acquired through topical creams, dietary supplements, and ingestion of pennies.
Ethanol abuse, defined as the regular daily intake of more than 80 g of ethanol per day, can cause bone marrow hypocellularity, megaloblastic change, vacuolation of erythroid and granulocytic precursors, multinuclearity of erythroid precursors, ringed sideroblasts, and impaired granulocyte maturation (15, 16, 17, 18, 19, 20, 21, 22).
Infectious agents causing NMD include cytomegalovirus, human herpesvirus 6, and parvovirus B19 (23, 24, 25, 26). Human immunodeficiency virus infection is associated with dysplastic and megaloblastic hematopoiesis (human immunodeficiency virus myelopathy), attributable to both the direct effects of human immunodeficiency virus infection and antiretroviral therapy (Fig. 16.2) (27, 28, 29, 30). Plasmodium falciparum infection (falciparum malaria) has been associated with numerous bone marrow changes, including myeloid and erythroid hyperplasia, megaloblastosis, dyserythropoiesis, erythroid karyorrhexis, and giant metamyelocytes (31, 32, 33, 34). Visceral leishmaniasis is associated with dyserythropoiesis and dysgranulopoiesis (35).
Medications can cause NMD. Valproic acid causes Pelger-Hüet anomaly of neutrophils, thrombocytopenia, macrocytic anemia, macrocytosis, myelodysplasia, aplastic anemia, and marrow changes resembling acute promyelocytic leukemia (36, 37, 38). Ganciclovir can produce intracytoplasmic and intranuclear inclusions in neutrophils and monocytes (39). Colchicine produces, in addition to marked bone marrow suppression, unusual mitotic figures arrested in metaphase attributable to microtubular dysfunction, in addition to striking dyserythropoiesis and dysgranulopoiesis (40). Tetracycline analogues may cause sideroblastic anemia (41).
TABLE 16.1 Conditions Associated with Acquired Nonclonal Myelodysplasia
Advanced age
Ethanol abuse
Aromatic hydrocarbon exposure
Infectious agents
Cigarette smoking
Medications
Erythroid hyperplasia and ineffective erythropoiesis
Hereditary disorders of metabolism
Arsenic intoxication
Solid organ transplantation
Lead poisoning
Advanced liver disease
Carcinoma
Hemophagocytic syndrome
Copper deficiency and zinc excess
Other inflammatory conditions
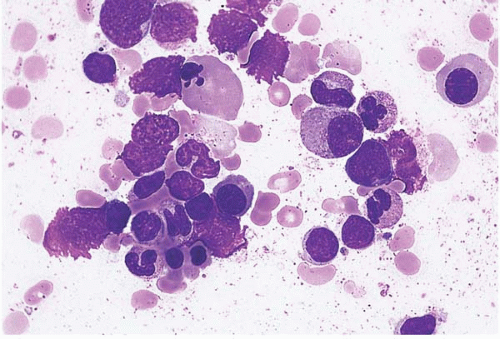
Figure 16.1 Acquired nonclonal myelodysplasia, bone marrow aspirate. Dyserythropoietic nucleated red blood cell precursors are present in this specimen from a patient with erythroid hyperplasia caused by cigarette smoking.
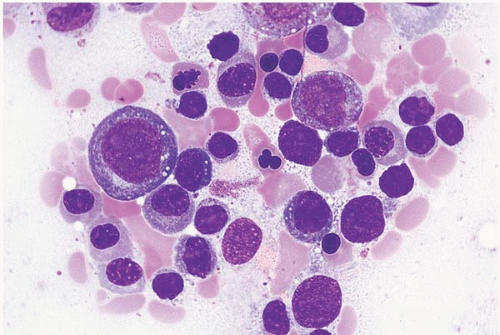
Figure 16.2 Acquired nonclonal myelodysplasia, bone marrow aspirate. A dysplastic erythroid precursor in seen in this specimen from a patient with human immunodeficiency virus infection.
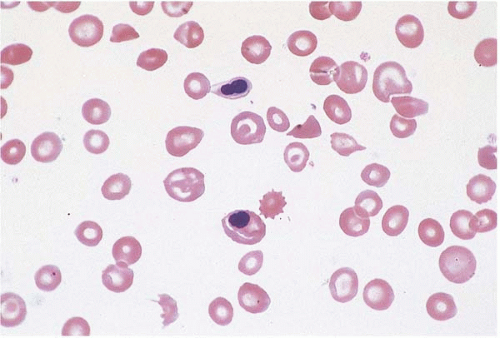
Figure 16.3 Acquired nonclonal myelodysplasia, peripheral blood. Dyserythropoietic nucleated red blood cells are seen in this specimen from a patient with sickle cell anemia.
Other conditions associated with acquired NMD include hereditary disorders of metabolism (42,43), solid organ transplantation (44), advanced liver disease (45), hemophagocytic syndrome (46), and other inflammatory conditions characterized by increased cytokine production (47, 48, 49).
Dyserythropoiesis may be the predominant finding, especially in cases of increased and’or ineffective erythropoiesis (Table 16.2 and Figs. 16.3 and 16.4). Underlying disorders are listed in Table 16.2. Turner syndrome may be accompanied by macrocytic anemia, dyserythropoiesis, and multinuclearity of erythroid precursors (63). Hairy cell leukemia may be accompanied by marked abnormalities in erythroid precursors, including megaloblastic change, abnormal nuclear lobation, multinuclearity, and ringed sideroblasts (64,65). Hyperosmolarity is an unusual cause of erythroblast vacuolation (66). Erythroblastic synartesis is a rare disorder in which erythroid precursors are linked by tight interdigitating membranes; it appears to be caused by an antimembrane immunoglobulin, which may account for its occurrence with monoclonal gammopathy (52,67).
TABLE 16.2 Conditions Associated with Acquired Nonclonal Dyserythropoiesis
Autoimmune hemolytic anemia
Drug reaction
Congenital Fas deficiency
Hemophagocytic syndrome
Hemoglobinopathy
Necrotic bone marrow metastasis
Iron deficiency
Turner syndrome
Vitamin B12 deficiency
Hairy cell leukemia
Malaria
Hyperosmolarity
Systemic lupus erythematosus
Erythroblastic synartesis
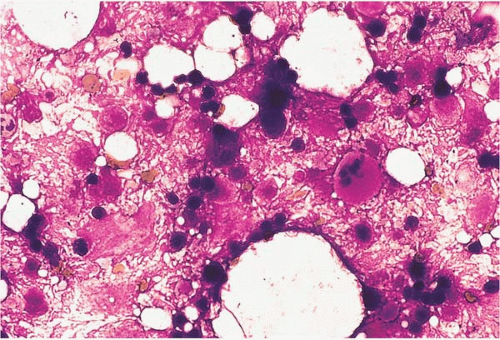
Figure 16.4 Necrosis, bone marrow aspirate. Smudged cellular remnants are seen in a background of dense amorphous material in this specimen from a patient with hemoglobin SC disease.
The differential diagnosis includes artifactual changes in erythroid precursors owing to storage in ethylenediaminetetraacetic acid (EDTA) (68).
Dysgranulopoiesis is the predominant finding in other settings. Acquired (pseudo-) Pelger-Hüet anomaly (PHA) is the appearance of hypolobated neutrophil nuclei, usually in adult life (Table 16.3). It may be the only sign of acquired NMD and is typically reversible with elimination of the underlying condition. Disorders and agents associated with acquired PHA include tuberculosis, Mycoplasma pneumonia, some medications, chronic lymphocytic leukemia, malignant lymphoma, Hodgkin lymphoma, and multiple myeloma (38,69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80).
The differential diagnosis includes constitutional PHA (see Chapter 4) and acquired clonal PHA, a frequent finding in clonal hematopoietic disease with chromosome 17p deletion.
TABLE 16.3 Conditions Associated with Acquired Nonclonal Pelger-Hüet Anomaly
Tuberculosis
Malignant lymphoma
Mycoplasma pneumonia
Hodgkin lymphoma
Medications
Multiple myeloma
Chronic lymphocytic leukemia
Only gold members can continue reading. Log In or Register to continue