Palatal MM With Satellite Lesions Primary mucosal melanoma (MM) of the hard palate presents as a diffuse, patchy area of heavy pigmentation with irregular borders . Satellite lesions are noted away from the main area of pigmentation .
Epithelioid Melanocytes in Nodular MM Nodular melanoma of the hard palate shows epithelioid malignant melanocytes, some with melanin pigment, expanded into the lamina propria. Individual melanocytes are seen in the upper layers of the mucosa (pagetoid spread).
Pseudoepitheliomatous Hyperplasia in MM There is a concurrent pseudoepitheliomatous hyperplasia present in association with an atypical melanocytic proliferation. An inflammatory infiltrate is also present. The melanoma may be obscured or missed due to this process.
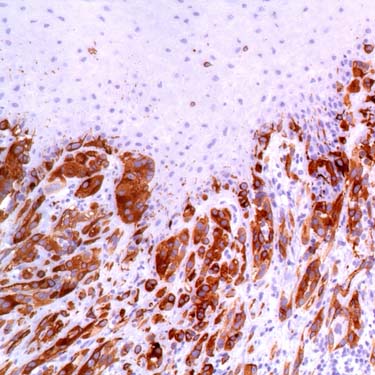
HMB-45 Highlights Melanocytes in MM HMB-45 immunohistochemistry highlights the melanocytes present both in the basal layer as well as in the submucosa. This is one of the more specific markers for melanoma. It is important to know that staining can be patchy or focal.
TERMINOLOGY
Definitions
• Malignant neural crest-derived neoplasm with melanocytic differentiation in oral cavity
Atypical melanocytes at epithelial-connective tissue interface with upward migration or connective tissue invasion
ETIOLOGY/PATHOGENESIS
Etiology
• Unknown: Not related to preexisting mucosal nevi or physiologic pigmentation
• Increased frequency of KIT (c-KIT, CD117) mutations in mucosal melanomas have been reported
Mutation not often detected in cutaneous melanomas
• BRAF mutations not detected in mucosal melanoma, but seen in cutaneous melanomas
CLINICAL ISSUES
Epidemiology
• Incidence
Extremely rare, accounting for < 1% of all melanomas
– 0.02/100,000 population/year in USA
Represent ~ 40% of all head and neck mucosal melanomas
Represent < 0.5% of all oral malignancies
Unlike cutaneous melanoma, oral melanoma incidence has been stable
• Age
Mean: 6th-7th decades; rare in pediatric patients
• Sex
M > F (2.5-3:1)
• Ethnicity
More common in Japan and western Africa
Site
• Hard palate and maxillary alveolus are most common sites of involvement (~ 80%)
• Remaining 20% include
Mandibular gingivae
Buccal mucosa
Floor of mouth and tongue
Presentation
• Most arise de novo, although 1/3 are preceded by pigmented lesion for few months or years
Melanosis reported before development of melanoma
• Asymmetric, painless, pigmented lesion
Irregular borders or outlines
Black, purple, red, gray
– 15% of oral melanomas are amelanotic
Macular, with nodular areas
• Many patients present at advanced stage with pain, ulceration, loose teeth
• Cervical lymph nodes metastases reported in up to 50% of cases at presentation
Lymph node metastases increase when tumor thickness > 5 mm
Only gold members can continue reading. Log In or Register to continue


 . Satellite lesions are noted away from the main area of pigmentation
. Satellite lesions are noted away from the main area of pigmentation  .
.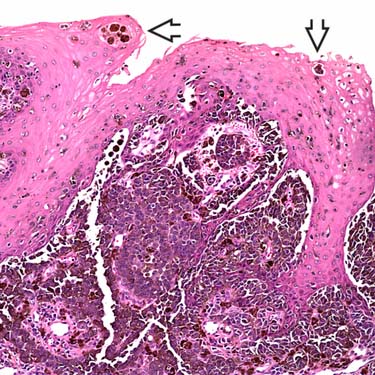
 are seen in the upper layers of the mucosa (pagetoid spread).
are seen in the upper layers of the mucosa (pagetoid spread).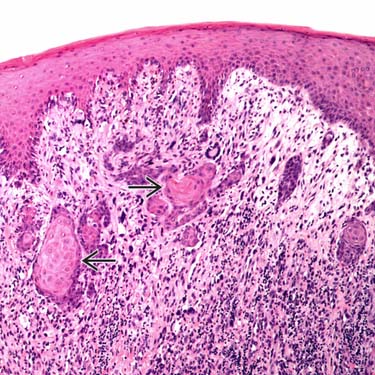
 present in association with an atypical melanocytic proliferation. An inflammatory infiltrate is also present. The melanoma may be obscured or missed due to this process.
present in association with an atypical melanocytic proliferation. An inflammatory infiltrate is also present. The melanoma may be obscured or missed due to this process.