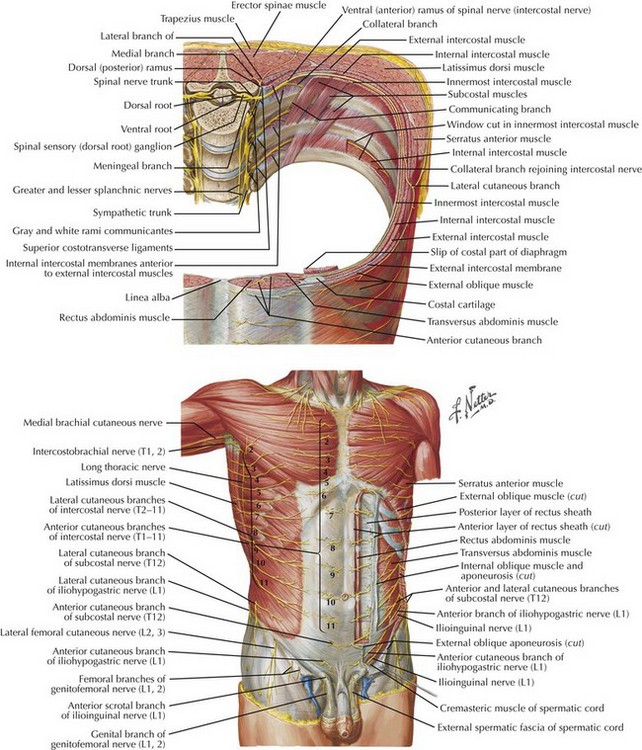
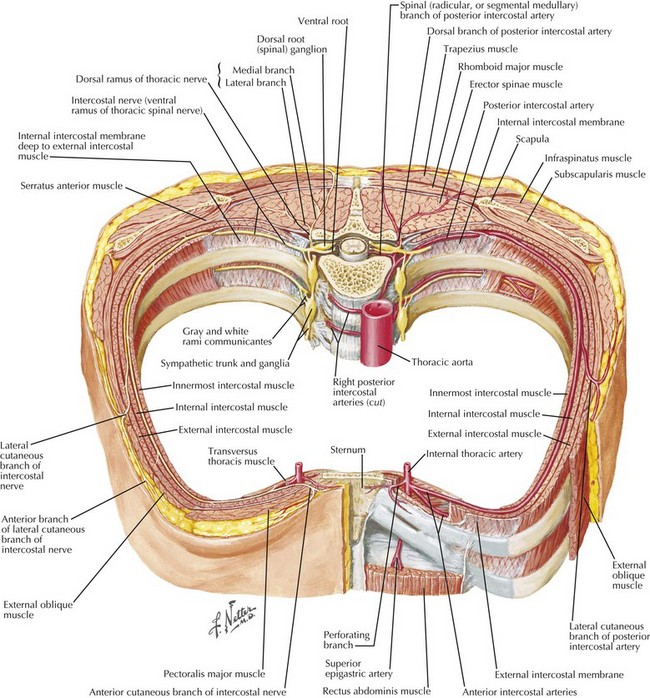
Chapter 31 Figures 31-1 and 31-2 show the anatomy of the vascular supply and innervation of the abdominal wall. Understanding the relationships of these nerves and vessels and their location in the abdominal wall is critical to preserve them during dissection, to maintain an innervated functional abdominal wall.
Open Ventral Hernia Repair
Anatomy of Abdominal Wall
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine