Nutrition Therapy in Hospital and Outpatient Medicine1
Nutrition Therapy in Hospital and Outpatient Medicine1
Kris M. Mogensen
MalColm K. Robinson
1Abbreviations: ASPEN, American Society for Parenteral and Enteral Nutrition; CRBSI, catheter-related bloodstream infection; EN, enteral nutrition; GI, gastrointestinal; HEN, home enteral nutrition; HPN, home parenteral nutrition; NRI, nutrition risk index, NTT, nutrition therapy team; PN, parenteral nutrition.
Patients who have an impaired alimentary tract, altered sensorium, or are critically ill frequently require specialized nutrition and feeding regimens. Such patients are by definition complex. As a consequence, their care is improved when they are managed in part by a multidisciplinary team with expertise in the administration of such feedings.
This chapter focuses on the role of the nutrition therapy team (NTT), the benefits of the team approach to nutrition management, and the delivery of complex nutrition therapies in inpatient and outpatient settings.
NUTRITION THERAPY TEAM
Patients may require a forced-feeding regimen when they are unable to consume food by mouth for prolonged periods. Such feeding regimens consist of enteral feeding that bypasses the mouth, parenteral nutrition (PN), or a combination of the two. Both types of feedings are reviewed in detail in the chapters on enteral feeding and PN.
Administration of PN and enteral nutrition (EN) to those who need it is traditionally referred to as nutrition support. However, a more apt term may be nutrition therapy. Use of the term therapy recognizes the role of nutrition in affecting patient outcome and acknowledges the demonstrable risks and benefits to nutrition intervention in both the short term and the long term. In addition, health care professionals with specialized nutrition training can help optimize overall therapy for many patients by enhancing the possible benefits of nutrition intervention while controlling the risks. The interdisciplinary team approach in managing patients receiving EN and PN was recognized to be beneficial as early as the 1970s. Now, NTTs commonly comanage patients receiving forced feedings (1).
Team Structure and Members
Managing patients receiving EN or PN requires clinicians who are well versed in both clinical medicine and nutrition therapy. Knowledge of both is required for one to develop a rational plan for nutrition intervention within the larger context of overall patient care goals. Team members must be able to assess nutritional status, estimate energy and protein requirements, and evaluate micronutrient status. They should also understand drug-nutrient interactions; how to calculate and compound PN admixtures; and how to select, place, and care for parenteral and enteral access devices. Because of the broad range of knowledge required for management of nutrition therapy, the team is necessarily composed of several clinicians with expertise to include all these areas (2).
The classic NTT comprises a physician, dietitian, nurse, and pharmacist. Each member of the team has a unique role, but expertise frequently overlaps (2). With the increasing numbers of physician extenders entering the work force, teams may now include physician assistants and nurse practitioners. Other health care professionals, such as speech and swallowing pathologists and physical therapists, may participate in the team on an ad hoc basis. This is particularly important in managing patients with swallowing disorders that may predispose them to feeding aspiration or those severely debilitated individuals who need aggressive physical therapy in addition to nutrition to restore lean body mass (2).
The American Society for Parenteral and Enteral Nutrition (ASPEN) developed discipline-based Standards of Practice for the four core members (physician, dietitian, nurse, and pharmacist) of the traditional NTT (3, 4, 5, 6). These standards are reviewed and revised on a regular basis and are designed to provide guidelines for clinical competencies for providing appropriate care to the patient requiring nutrition support or therapy. Approximately 63% of large academic medical centers have a formal, comprehensive NTT based on the 2008 ASPEN member survey (2). In smaller hospitals, however, the team may be an informal consultation group in which each member works almost exclusively in his or her primary department. The group only meets periodically when necessary to discuss patient care. Other teams are structured in committee form to develop general policies and procedures related to nutrition therapies, but do not provide consultation for individual patients (2).
IMPACT OF THE DEDICATED TEAM
ASPEN and other societies such as the American Gastroenterological Association published guidelines for the initiation and management of PN and EN (7, 8, 9, 10, 11). The ASPEN guidelines for appropriate use of PN are summarized in Table 85.1, and typical indications for EN are summarized in Table 85.2 (7, 8, 9, 10). These guidelines are detailed and may lead some to believe that dedicated NTTs are unnecessary. However, EN and PN are frequently inappropriately used in the absence of a dedicated specialty team even in large academic medical centers.
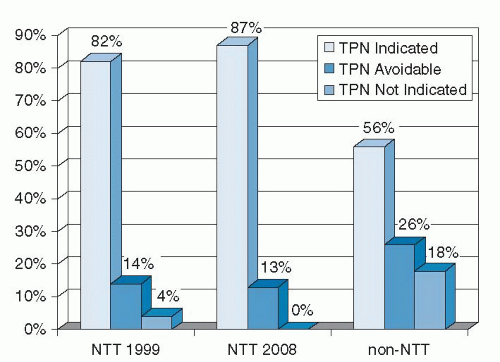
Trujillo et al (12) assessed the impact of a dedicated NTT in a busy academic medical center. These investigators looked at 209 consecutive patients started on PN with and without NTT consultation and used ASPEN guidelines to determine whether the PN was “indicated,” “avoidable” (i.e., could have been avoided if the appropriate enteral access was in place), or “not indicated.” They found that PN was indicated only 56% of the time and was clearly not indicated 18% of the time for patients without NTT consultation. In contrast, PN was indicated 82% of the time and was not indicated only 4% of the time for those patients with NTT consultation (p = .004).
TABLE 85.1 INDICATIONS FOR PARENTERAL NUTRITION
Inability to use GI tract for >7-10 d (3-5 d in the ICU)
Diffuse peritonitis
Enterocutaneous fistula where enteral feeding is not possible
GI ischemia
Intestinal obstruction
Intractable vomiting
Intractable diarrhea
Intestinal failure
Prolonged ileus
Severe exacerbation of inflammatory bowel disease
Severe GI bleeding
Severe pancreatitis after failed EN trial
Severe malabsorption with intolerance to EN or failed EN trial
Severe malnutrition with inability to use EN
EN, enteral nutrition; GI, gastrointestinal; ICU, intensive care unit.
TABLE 85.2 INDICATIONS FOR ENTERAL NUTRITION
Inadequate oral intake for >7-10 d (3-5 d in the ICU) with functional gastrointestinal tract
Enterocutaneous fistula (if feeding tube can be inserted distal to the fistula)
Head or neck cancer
Inadequate oral intake to meet a high metabolic demand (e.g., trauma or burn patient)
Significant malnutrition with inadequate oral intake for repletion
Stroke or other neurologic compromise with significant dysphagia
Swallowing disorders
ICU, intensive care unit.
Based on the initial success of the NTT, the hospital initiated a policy of requiring NTT approval for all PN starts and directed the pharmacy not to start PN without specific NTT physician sign-off. Follow-up review of PN utilization in 2008 revealed that PN was clearly indicated 87% of the time and was preventable 13% of the time if enteral access had been available (unpublished data). No patients for whom PN was not indicated were identified (Fig. 85.1). Other investigators confirmed the findings of Trujillo et al, thus documenting the value of a dedicated NTT (13, 14, 15, 16, 17).
Clinical Outcomes and Cost Savings
Decreasing inappropriate PN utilization alone improves patient outcomes and reduces health care costs. PN utilization increases the risk of catheter-related bloodstream infection (CRBSI) up to 10-fold (18, 19). NTTs have been instrumental in reducing the rate of CRBSIs with implementation of strict aseptic technique for catheter insertion and protocols for appropriate care of central venous catheters. For example, Nehme (20) reported a 1.3% infectious complication rate for NTT-managed patients compared with a 26.2% complication rate in patients not managed by NTTs. Similarly, Faubion et al (21) demonstrated a decrease in catheter-related infection from 24% to 3.5% with implementation of a team to insert catheters used for administration of PN; the team also certified staff to provide routine care for those catheters. In addition, loss of a nurse NTT member in one report (22) led to a significant increase in relative risk of central line infection, a finding emphasizing the importance of an intact NTT to prevent this severe complication.
Fig. 85.1. Mandatory nutrition therapy team (NTT) approval before initiation of total parenteral nutrition (TPN) has had a sustained impact on inappropriate TPN utilization. (Adapted with permission from Trujillo EB, Young LS, Chertow GM et al. Metabolic and monetary costs of avoidable parenteral nutrition use. JPEN J Parenter Enteral Nutr 1999;23:109-13.)
Thus, NTTs decrease infection risks through two avenues. First, nonindicated PN starts are minimized, thereby reducing the CRBSI risk associated with PN administration. Second, even in those patients who are receiving PN, NTTs have reduced CRBSIs by improving standards of catheter insertion and care.
Minimizing infection rates can translate into potentially huge cost savings for medical institutions. The cost of treating one central-line infection in the United States has been estimated to be $3700 to $29,000 (23). Hence, the prevention of a small number of CRBSIs can fund most, if not all, of the salaries of a comprehensive NTT. In large medical centers, the cost savings associated with prevention of CRBSIs can exceed the cost of funding an NTT.
Reduction of central-line associated infections is no longer a focus of just NTTs. With the initiation of the 100,000 Lives Campaign (24), reduction in central line infections has become a priority for all hospitals. Use of the Institute of Healthcare Improvement Central Line Bundle (25) has been shown to decrease incidence of central line infections (26, 27, 28). What was once a small outcome measure of the effectiveness of NTTs has grown into a key quality indicator for all hospitals.
Moreover, central line insertion carries with it a real morbidity and mortality risk and financial costs. Catheter insertion can lead to pneumothorax, vascular injury, and discomfort to the patient. Rarely, patients may die from catheter insertions complicated by uncontrollable bleeding from a vascular injury or administration of PN through misplaced catheters whose tips errantly end in the lung or pleural space. Such complications, as well as the cost associated with inserting the catheters and treating these potential mechanical complications, are avoided by limiting inappropriate PN initiation.
Finally, the reduction of inappropriate PN use and the increased use of EN save money. PN is inherently more costly than EN, given the cost of each component of the PN admixture and pharmacy costs associated with compounding time and complex equipment. The cost savings is even higher if the costs associated with PN monitoring, administration, and nursing time are included (29).
Many studies looking at reductions in inappropriate PN use evaluated cost savings to the hospital. The reported savings ranged from approximately $6000 for institutions with already low rates of inappropriate PN utilization (17) to more than $500,000/year in large hospitals in which inappropriate PN use was rampant (12). These savings easily justify the existence of an NTT.
The role of dedicated NTTs is not just limited to approval of PN and EN initiation and preventing PN-associated infections. Several studies indicated that such teams improve clinical outcome when forced feedings are indicated. For example, Trujillo et al (12) evaluated 209 PN starts and found that those patients followed by the NTT had a significantly lower incidence of metabolic complications such as electrolyte imbalances and hyperglycemia (34% versus 66% of PN days, p = .004). Similarly, Nehme (20) evaluated 211 patients receiving PN who were managed by the NTT compared with 164 patients whose PN was managed by the primary medical or surgical team. Only 3% of the NTT-managed patients experienced an electrolyte imbalance compared with 36% of the patients not managed by an NTT. In addition, no NTT-managed patients experienced hyperglycemia severe enough to lead to hyperglycemic nonketotic dehydration, compared with 7% of the patients who were not managed by an NTT.
In contrast, ChrisAnderson et al (30) evaluated the impact of an NTT on metabolic complications associated with PN at a large teaching hospital and compared the change from the elective to mandatory consultation of an NTT for all patients receiving PN. No significant differences in metabolic complications were associated with this change. The investigators believed that their institution had a robust nutrition teaching service before the implementation of mandatory consultation that minimized the team’s impact.
Only gold members can continue reading. Log In or Register to continue