1Abbreviations: ADA, American Dental Association; AIDS, acquired immunodeficiency syndrome; CRA, caries risk assessment; DMFS, decayed-missing-filled surfaces; ECC, early childhood caries; GI, gastrointestinal; HIV, human immunodeficiency virus; NHANES, National Health and Nutrition Examination Survey; NIDR, National Institute of Dental Research.
CELLULAR AND STRUCTURAL CHARACTERISTICS OF THE ORAL TISSUES
Distinctive characteristics of oral tissues, such as the inability of enamel to remodel and the high cellular turnover rate of oral mucosa, the rates of alveolar bone growth, and the production of saliva, make oral tissues a unique indicator of physiologic perturbations. The oral cavity is a site of symptoms of many chronic diseases including dental caries, periodontal disease, acquired immunodeficiency syndrome (AIDS), nutritional anemias, herpes, salivary gland disorders, osteoporosis, diabetes, and cancer. Congenital anomalies such as cleft lip and palate are birth defects that have a complex genetic and environmental etiology linked to maternal nutrient status, folate in particular.
The linkages between oral disease and systemic health are expanding in depth and breadth with some profound observations. Within the past two decades, clear linkages have been established between periodontal disease and cardiovascular disease, diabetes, stroke, and adverse pregnancy outcomes. For example, periodontal disease is associated with increased risk of cardiovascular disease (1) and preterm delivery (2, 3). The inherent nature of oral infectious d iseases requires an adequately functioning immune and cellular repair system, and unequivocal data link nutrient intake and these host defense mechanisms. The relationships among oral health, systemic health, and nutrition require the careful attention of all health professionals including physicians, dentists, registered dietitians, and nurses (3).
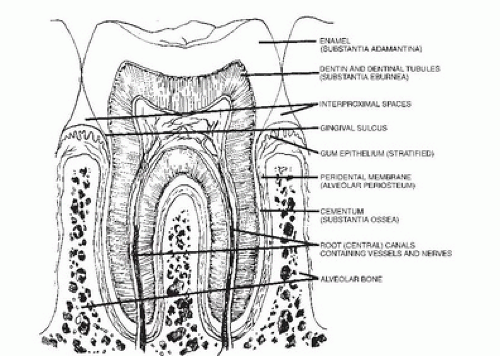
To fully appreciate these complex relationships, it is vital to understand the structure and function of the craniofacial-oral-dental complex. Teeth are specialized structures necessary for the initial processing of food and are composed of three mineralized tissues: enamel, dentin, and cementum, which encase the highly vascular dental pulp or “nerve.” These relationships can be seen in the schematic cross section of a tooth in Figure 73.1. The teeth are retained in their bony sockets by means of a fibrous structure termed the periodontal membrane or ligament. Factors such as bacteria and the inflammatory immune response can affect the integrity of this structure and bone surrounding the socket, resulting in periodontal disease that may progress sufficiently to cause loosening and loss of the teeth (4).
Each tooth develops from a tooth bud or germ located in the jaws. The bud consists of an epithelial component that arises as an invagination from the surface and produces enamel. The mesenchymal component consists of the dental papilla, which produces the tooth pulp and dentin, and the dental follicle, which produces the cementum and periodontal ligament once the tooth has formed. Table 73.1 details the chronology of the formation of the human dentition. The primary teeth begin forming at approximately 6 weeks in utero when cells in the primitive oral cavity differentiate to form the dental lamina, which is the site of tooth bud development. The formation of the crown of the tooth begins with the secretion of a dentin matrix containing collagen fibrils. Mineral ions then enter the matrix to form small crystals on or between the collagen fibrils. Enamel formation begins as soon as the first dentin layer has been laid down. This mineralization process constitutes the maturation of enamel and continues after the matrix is fully formed. As can be seen in Table 73.1, the mineralization process begins as early as 4 months in utero and continues into late adolescence. After the tooth erupts into the oral cavity, it continues to incorporate minerals (including fluoride) into its structure from saliva, food, and drinking fluids (5).
The life history of a tooth may be divided into three main eras: (a) the period during which its crown is forming and mineralizing in the jaw, (b) the period of maturation when the tooth is erupting into the oral cavity and its root or roots are forming, and (c) the maintenance period while it is functioning in the oral cavity (5). During the preeruptive period, the developing enamel and dentin are subject to nutritional deficiencies or imbalances in the same manner as any other developing tissues. Nutrient deficiencies can affect the secretory and the maturation stages of enamel formation. Following eruption into the oral cavity, the enamel is bathed in saliva and is exposed to oral microorganisms and their byproducts as well as food, so nutritional deficiencies or excesses and dietary habits may affect teeth in a local manner (5).
Fig. 73.1. Schematic illustration of teeth in contact with the alveolar bone.
At least three striking differences exist between the mineralized tissues of teeth and other tissues of the body. First, enamel contains no capillary or lymphatic vessels to act as transport systems; however, the intimate relationships between the organic and the inorganic components of enamel suggest that pathways in the enamel exist for diffusion of ions and small molecules from saliva, and possibly from blood. Although the dentin likewise contains no vascular elements, it is more readily permeable to the passage of extracellular fluids from the blood, by way of the dentinal tubules that traverse the dentin. The interchange among elements in the enamel takes place through the bathing of its external surface with saliva. In contrast, the interchange in the dentin occurs by the movement of ions present in the blood supply to the pulp or periodontal membrane (4). Second, because of the absence of cells, mineralized dental tissues do not have a microscopically or chemically detectable ability to repair improperly formed or mineralized areas, and the tooth does not have the ability to repair itself after a portion has been destroyed by tooth decay or mechanical injury. An exception is the remineralization of slightly demineralized, superficial areas of the enamel where the organic matrix and surface integrity are still intact, commonly referred to as “white spots.” In addition, secondary dentin is formed by the odontoblasts, which persist throughout life on the pulpal surface of the dentin, in response to chemical stimuli from an advancing carious lesion in an effort to mitigate the noxious influence. Lack of ability to repair dental tissues is in direct contrast to bone, with its continual turnover and ability to remodel (4). Third, unlike other tissues, the mineralized tissues of teeth undergo a partial change of environment. When the tooth begins to emerge into the oral cavity, the vascular supply to the enamel organ is severed, and the enamel surface comes in contact with a complex mixture of saliva, microorganisms, food debris, and epithelial remnants. Thus, instead of a pure systemic environment, the erupted tooth has, in addition, an oral or external environment. As a consequence, the enamel and cementum surfaces on which carious lesions are initiated by microbial action are largely outside the influences of humoral immune systems, so immune relationships with the caries process are primarily limited to those in saliva (4).
TABLE 73.1 CHRONOLOGY OF DEVELOPMENT OF THE HUMAN DENTITION
TOOTH
HARD TISSUE FORMATION BEGINS
AMOUNT OF ENAMEL FORMED AT BIRTH
ENAMEL COMPLETED
ERUPTION
ROOT COMPLETED
Primary dentition
Maxillary
Central incisor
4 mo in utero
Five sixths
1½ mo
7½ mo
1½ y
Lateral incisor
4½ mo in utero
Two thirds
2½ mo
9 mo
2 y
Cuspid
5 mo in utero
One third
9 mo
18 mo
3¼ y
First molar
5 mo in utero
Cusps united
6 mo
14 mo
2½ y
Second molar
6 mo in utero
Cusp tips still isolated
11 mo
24 mo
3 y
Mandibular
Central incisor
4½ mo in utero
Three fifths
2½ mo
6 mo
1½ y
Lateral incisor
4½ mo in utero
Three fifths
3 mo
7 mo
1½ y
Cuspid
5 mo in utero
One third
9 mo
16 mo
3¼ y
First molar
5 mo in utero
Cusps united
5½ mo
12 mo
2¼ y
Second molar
6 mo in utero
Cusp tips still isolated
10 mo
20 mo
3 y
Permanent dentition
Maxillary
Central incisor
3-4 mo
—
4-5 y
7-8 y
10 y
Lateral incisor
10-12 mo
—
4-5 y
8-9 y
11 y
Cuspid
4-5 mo
—
6-7 y
11-12 y
13-15 y
First bicuspid
1½-1¾ y
—
5-6 y
10-11 y
12-13 y
Second bicuspid
2-2¼ y
—
6-7 y
10-12 y
12-14 y
First molar
At birth
Sometimes a trace
2½-3 y
6-7 y
9-10 y
Second molar
2½-3 y
—
7-8 y
12-13 y
14-16 y
Mandibular
Central incisor
3-4 mo
—
4-5 y
6-7 y
9 y
Lateral incisor
3-4 mo
—
4-5 y
7-8 y
10 y
Cuspid
4-5 mo
—
6-7 y
9-10 y
12-14 y
First bicuspid
1¾-2 y
—
5-6 y
10-12 y
12-13 y
Second bicuspid
2¼-2½ y
—
6-7 y
11-12 y
13-14 y
First molar
At birth
Sometimes a trace
2½ -3 y
6-7 y
9-10 y
Second molar
2½-3 y
—
7-8 y
11-13 y
14-5 y
The development and maintenance of the soft tissues and bone that support the teeth are also subject to nutrient defects. The periodontium, as seen in Figure 73.1, comprises the gingiva; the periodontal ligament ( peridental membrane), which joins the root cementum to the alveolar bone; the root cementum, which is a specialized, mineralized tissue similar to bone that covers the root of the tooth; and the alveolar bone, which forms and supports the sockets of the teeth. The alveolar bone grows in response to dental eruption, is modified by dental changes, and resorbs when teeth are lost. The finite space between the tooth and the gingiva, known as the gingival sulcus, is lined by a nonkeratinized epithelium. In addition, dental plaque, one of the primary agents responsible for the initiation of both dental caries and gingivitis, contains a high concentration of bacteria, which, in the gingival sulcus, are juxtaposed with a “naked” epithelium. Thus, bacteria and their byproducts or antigens can permeate the gingival epithelium and precipitate a classic inflammatory response that denotes periodontal disease. In fact, an intact immune system, which is highly dependent on nutrient status, is vital to maintain periodontal health. The diversity of hard and soft tissues that comprise the oral structures and the distinctive nutritional needs of each contribute to the uniqueness of the mouth as an external reflection of past and present nutritional problems (3, 6).
ROLE OF NUTRITION IN CRANIOFACIAL AND ORAL TISSUE DEVELOPMENT
Nutrient deficits can result in defects in tooth and salivary gland development. The most commonly studied conditions and nutrients that have affected tooth integrity, enamel solubility, and salivary flow and composition in animal models include protein-calorie malnutrition, ascorbic acid, vitamin A, vitamin D, calcium and phosphorus, iron, zinc, and fluoride. Malnutrition—deficiencies of vitamin A, ascorbic acid, vitamin D, and iodine—and fluoride excess have been demonstrated to affect human dentition (Table 73.2). The reader is also encouraged to review relevant sections of chapters in this text on each specific nutrient mentioned.
Enamel hypoplastic defects and hypomineralization have been the hallmarks of undernutrition and overnutrition during tooth development (7, 8). Vitamin A deficiency has been implicated as a critical factor in tooth health because it frequently accompanies proteincalorie malnutrition and is known to affect epithelial tissue development, tooth morphogenesis, and odontoblast differentiation (9). The interference with calcification is manifested clinically by enamel hypoplasia (10). Additionally, vitamin A excess, when present during the first trimester of pregnancy, can result in severe craniofacial and oral clefts and limb defects (11).
Vitamin D, calcium, and phosphorus deficiencies all result in significant effects on tooth development and decreased resistance to dental caries. If a vitamin D deficiency occurs in utero or young infants, there may be delays in tooth eruption and quality of enamel is delayed, thereby increasing caries risk (12). Leaver demonstrated that extreme calcium and phosphorus deficiencies may result in hypomineralization of developing teeth (13). The deficit, however, must be severe enough to reduce plasma levels of calcium and phosphorus. The highly effective homeostatic mechanisms in humans that mobilize calcium from the skeleton to maintain normal plasma calcium levels make the chances of this occurring rare. Bawden postulated that vitamin D hypovitaminosis may be more important in considering hypomineralization resulting from inadequate calcium transport into developing dental tissues (14). Vitamin D deficiency has also been shown to affect tooth structure and to delay eruption patterns of teeth (15).
TABLE 73.2 EFFECTS OF NUTRIENT DEFICIENCIES ON TOOTH DEVELOPMENT
Stability of enamel crystal (enamel formation) Inhibition of demineralization Stimulation of remineralization Mottled enamel (excess) Inhibition of bacterial growth
In childhood vitamin D deficiency, teeth are characterized microscopically by a widened layer of predentin, by the presence of interglobular dentin, and by interference with enamel formation (hypoplastic defects) (16). Young children with rickets have delayed eruption of the deciduous teeth, and the sequence of eruption is altered. The permanent incisors, cuspids, and first molars are usually affected because their development coincides with the age at which rickets is most common. Vitamin D-resistant rickets results in more frequent and severe tooth defects relative to primary rickets, including large pulps with developmental “exposures” of the pulp.
Vitamin C deficiency has also been demonstrated to affect tooth development and eruption. Deciduous and permanent teeth of scorbutic infants contain minute pulpal hemorrhages attributable to vitamin C deficiency. In older vitamin C-deficient children, the dental pulp undergoes hyperemia, edema, necrosis, and aberrant calcification, whereas the dentin shows odontoblastic degeneration and irregular formation (17). The relationship between vitamin C deficiency and dental caries is poorly defined, however. Although it is likely that the primary mechanism of vitamin C deficiency-induced tooth, gingival, and bone disease is mediated through the disruption of collagen biosyntheses, no study has clearly demonstrated the relationship between scurvy and dental caries (18). In areas where goiter is endemic, children born to mothers with severe iodine deficiency are characterized by marked mental and physical growth retardation. Eruption of the primary and secondary teeth is often greatly delayed and precluded. Malocclusion may occur because of the altered patterns of craniofacial growth and development.
Nutritional status during development can have profound effects on oral disease when malnutrition is present. Several studies have demonstrated that tooth eruption is delayed, tooth integrity is compromised (especially enamel surface solubility), and the incidence of dental caries is increased in chronically malnourished animals and children (19, 20). In Lima, Peru, Alvarez et al demonstrated significant delays in tooth eruption and exfoliation in three groups of malnourished children; such delays were associated with and appeared to be the direct cause of a significant temporal delay in caries development in the primary teeth (21). These data support previous studies on malnourished children in India and Guatemala (22, 23).
The development of teeth and salivary glands is intimately associated with the nutrient supply. Teeth subjected to nutritional insult during critical stages of development show a diminished ability to withstand caries and thus are at a higher risk for decay. Menaker and Navia found that impaired salivary function has accompanied the morphologic changes in teeth, which may be a primary factor in the subsequent increase in caries susceptibility (24). These data also explain in part the positive association between socioeconomic status and the prevalence of dental caries in deciduous but not permanent teeth (20). Nutritional injuries early in life may affect tooth formation and may result in increased caries susceptibility, and, depending on when malnutrition occurs in childhood, will impact caries risk. Malnutrition early in life delays tooth development; hence, teeth erupt later and caries will occur in the older child (20). As is discussed in the section under dental caries, the incidence of caries is more prevalent among economically deprived population groups, which also have a high risk of poor diets. As such, one may see concurrent increases in caries and malnutrition risk; in cases such as this, it may be difficult to determine which came first, the caries or the malnutrition, but both warrant immediate intervention using a team-based approach (5). Thus, in understanding any cross-sectional survey on caries prevalence, the nutritional and diet history must be taken into account.
On a broader scale, 3% of babies born in the United States each year have some birth defect evident at birth or later (25, 26). Prominent among these defects are structural, functional, or biochemical abnormalities involving the craniofacial complex. The most common of these malformations are cleft lip and cleft palate, affecting, 1 in 600 white infants, with the incidence higher among Asians, Native Americans, and Inuit and lower among blacks (25, 27). In addition, select other craniofacial oral-dental disorders such as craniosynostosis, hemifacial microsomia, anodontia, amelogenesis imperfecta, dentinogenesis imperfecta, osteogenesis imperfecta, chondrodystrophies, and juvenile periodontitis represent major challenges to human oral health (28). Neural tube defects are among the most common birth defects despite the decline in incidence with folate fortification of grain products (29); they range in severity and can result in incomplete formation of cranial bones. Many of these malformations and disorders have a genetic basis or an environmental cause. Certain nutrients given in excess, especially early in pregnancy (e.g., retinoic acid, and other lipophilic molecules such as vitamins K and E) are known to induce craniofacial oraldental malformations.
The regulatory genes and gene products functioning as transcriptional factors for the bronchial arches that give rise to the midface and lower face are being discovered, and their interaction with nutrients (e.g., retinoic acid via its specific receptors) has been found to be critical to craniofacial oral-dental morphogenesis (30). Excess exogenous retinoic acid produces significant craniofacial malformations associated with clefting, dental development, hemifacial microsomia, spina bifida, eye defects, and limb morphogenesis (31). A striking illustration of the need to understand the effects of nutrition on birth defects are the data that demonstrated that folate supplements provided around the time of conception significantly reduced the recurrence of neural tube defects among high-risk persons in the United Kingdom and elsewhere (29, 32, 33). Similar data are being established relating folic acid or multivitamins in congenital craniofacial malformations such as cleft lip and/or cleft palate (29, 33). Taparia et al advocated for the role of adequate folate for its protection against neurotubular and craniofacial defects and hypothesize roles for folate receptors in these disorders (33).
NUTRITION AND DENTAL CARIES
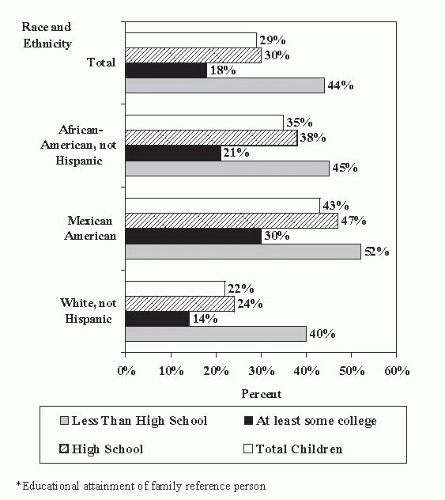
Dental caries is “the most common chronic disease in the United States and among the most common diseases in the world” and one of the most frequently occurring preventable infectious diseases of the oral cavity, globally affecting up to 90% of individuals in some countries (5, 34). It is a major cause of tooth loss in children and adults in the United States. It occurs more often than asthma, the second most common chronic pediatric disease (5). In 2000, the US Surgeon General reported that approximately 80% of the caries incidence in children and adolescents was present in approximately 25% of the population (5). More current reports show the problems remain, with the greatest incidence being among those in lower socioeconomic groups and children in the United States and globally (34, 35, 36). According to data from the National Health and Nutrition Examination Survey (NHANES 1999 to 2004), among 2- to 11-year-olds, the prevalence of dental caries in primary dentition is approximately 42% for the time period 1999 to 2004; in permanent teeth, the prevalence is approximately 21% for this age group (37). Among adults, the incidence of caries is substantially higher, approximately 90% for coronal caries and 14% for root caries, according to NHANES 1999 to 2004 data (37). The US Surgeon General has labeled children’s tooth decay as America’s silent epidemic and continues to be a major unmet health need in the United States (5). Data on the percentage of US children and adolescents who are caries free by age and ethnicity from the 1988 to 1994 NHANES survey are shown in Figure 73.2.
Since the mid-1970s, the incidence of dental caries has declined, mainly because of preventive measures such as fluoride and dental sealants (35, 37, 38). Dietary intake may contribute to dental caries (see the next section on the cause of dental caries); additionally, preserving the integrity of dentition is essential for overall nutritional status. Untreated tooth decay may lead to pain, eventual tooth loss with subsequent masticatory dysfunction, and compromised dietary intake.
The extent of dental decay in a population may be measured by decayed-missing-filled surfaces (DMFS), representing the sum of the number of permanent tooth surfaces (out of a possible 128 surfaces on 32 teeth) that are decayed, missing, or filled (39). According to NHANES data for 1999 to 2004 (the most recent for which data are available for this statistic) for children between the ages of 6 and 11, 42% had caries in their primary teeth (27); and for 6- to 19-year-olds using NHANES data for 1999 to 2002, 41% had caries in their permanent teeth (37). In contrast, NHANES III data for 1988 to 1994 show that, among US children aged 5 to 17 years old who were examined, more than one half (54.7%) had a cariesfree permanent dentition; however, the mean DMFS was 2.5 (36). In comparison, in the 1979 to 1980 survey conducted by the National Institute of Dental Research (NIDR) survey, 37% of school children examined had no caries in their permanent teeth, and the mean DMFS was 4.77. However, dental decay increases with age, so by 15 years of age approximately two thirds of US teens had experienced caries in their permanent dentition (see Fig. 73.2). Cavitation occurs most frequently on the occlusal or chewing surface of the tooth. The prevalence of decay and unfilled tooth surfaces tends to be greater among low-income children than those of higher income strata according to US and global data (27, 36, 40, 41).
Fig. 73.2. Percentage of US children and adolescents who are caries free by age and ethnicity. (From National Center for Health Statistics. Plan and Operation of the Third National Health and Nutrition Examination Survey 1988-94. Series 1, no. 322. Hyattsville, MD: National Center for Health Statistics, 1994; DHHS publ. no. [PHS] 94-1308, with permission.).
The rate of tooth loss, or edentulousness, has continued to decline (3). In the most recent US data available for the periods 1988 to 1994 and 1999 to 2004, for older adults the prevalence of edentulism decreased from approximately 34% to 27% (38). In the 1988 to 1991 survey, 26% of adults 65 to 69 years of age were edentulous as compared with 32% of adults in the 1985 to 1986 NIDR adult survey (27, 42). Many adults have had fluoride exposure for part of their lives; as a result, teeth are being retained longer.
Caries is a dynamic process that has three phases: (a) demineralization (loss of mineral when plaque pH falls to less than 5.5), (b) equilibrium, and (c) remineralization (occurs when plaque pH rises above the critical level to neutral or alkaline levels) of tooth enamel. In the early stage of tooth decay, often resulting from frequent fermentable carbohydrate exposure and poor oral hygiene, incipient lesions may develop rapidly. During periods when no bacterial fermentation is occurring, calcium, phosphorus, and fluoride that have been released from the tooth enamel can be redeposited in the enamel to remineralize the tooth. A clinical cavity (caries) is the final stage in the disease process. The average time for progression of incipient caries to a carious lesion in children is approximately 18 ± 6 months.
Diet or Nutrition as a Component of Caries Risk Assessment and Management Protocols
Caries risk assessment (CRA) guidelines and protocols exist for both children and adults (43, 44). In both, diet is identified as having a role in both etiology and management. Frequency of intake rather than total volume of fermentable carbohydrates (including sucrose, glucose, fructose, and cooked starches) is the critical factor when assessing caries risk (43). Although sugar consumption in the United States is still high, the availability of fluoridated water and the presence of fluoride in other foods and fluids have weakened the impact. The 2010 American Academy of Pediatric Dentistry (AAPD) CRA protocol includes the following diet-related factors for children up until the age of 5 years: consumption of more than three sugar-containing snacks or beverages between meals and going to bed with a bottle that contains sugared beverages (for age 6 and over the bottle factor is deleted) (45). Featherstone et al (43, 44) described CRA as a two-step process, the first of which is to determine patient-specific disease risk factors or indicators. The second step focuses on risk level determination. Diet-nutrition-related risk factors include between-meal snacks (foods and beverages) more than three times a day that contain fermentable carbohydrates.
Strategies for caries prevention are likewise multidimensional and include fluoride, as well as diet counseling with a focus on eating patterns and between-meal and bedtime consumption of foods and beverages containing fermentable carbohydrates (43, 44, 45, 46). More recently, xylitol-containing gum and mint consumption as an anticariogenic measure has been promoted (43, 45, 47). Caries management protocols for children more than 5 years old and for adults include diet counseling for children at moderate or high risk, with the addition of xylitol gums or mints (44, 45).
Role of Carbohydrates in Dental Caries
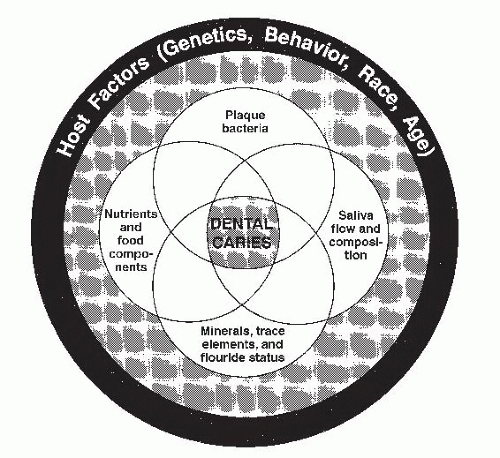
Dental caries is a multifactorial oral infectious disease. Fermentable carbohydrates are only one component in the etiology, along with the oral environment and dental plaque (Fig. 73.3). Fluoridated water and oral hygiene practices can have a dramatic impact on caries risk and development. Tooth erosion, which impairs tooth integrity, is not an infectious disease, but the resultant defects increase risk of caries. Presence and adequacy of saliva, immune status, and lifestyle behaviors affect caries risk.
Fig. 73.3. Major factors that interact in the dental caries process. (Adapted with permission from Navia JM. Carbohydrates and dental health. Am J Clin Nutr 1994;59[Suppl]:719S-27S.)
In addition to fluoride, primary factors influencing this balance are nutrition and diet (48). Nutrition has a systemic effect, whereas diet has a local effect. For example, systemically, malnutrition has a negative impact on the volume, antibacterial properties, and physiochemical properties of saliva. In addition, nutrition during development can affect the integrity of the tooth and salivary glands and the ability of the tooth to withstand bacterial challenge. Systemic diseases, medications affecting the integrity of the oral cavity, and salivary flow also can have an impact on nutritional well-being as well as oral health and oral infectious disease (including caries) risk (48, 49).
Sugars and cooked starches are fermentable carbohydrates. Sugars are found in the diet either as intrinsic, which are those found naturally in foods such as fruits, honey, and dairy products, or extrinsic, which are sugars added to foods during processing (50, 51, 52). Examples of added sugars include white or brown sugar, honey, molasses, maple, malt, corn syrup or high-fructose corn syrup, fructose, and dextrose (48, 51). Other disaccharides, in particular trehalose and isomaltose, have a lesser cariogenic risk than sucrose. Starches are subsequently digested by salivary amylase to oligosaccharides, which may be fermented by the oral microflora. According to Lingstrom et al, only the gelatinized starches are susceptible to breakdown by salivary amylase into maltose, maltotriose, and dextrins (53). Examples of cooked starches would include cereals (even those advertised as having no added sugar), cakes, cookies, pies, and snack foods.
Locally, dietary sources of fermentable carbohydrates are metabolized to acids by plaque bacteria, thus causing a drop in pH. Fermentable carbohydrates are carbohydrates (sugars and starch) that begin digestion in the oral cavity with salivary amylase. The low pH (<5.5) favors the growth of Streptococcus mutans (primary bacteria in the development of caries). In contrast, a diet with plenty of calcium-rich cheese eaten around mealtime favors remineralization.
Epidemiologic surveys, animal experiments, and early controlled human studies have all linked sugars to the development of dental caries. Studies from the later part of the twentieth century and the 2001 Caries Consensus Conference reported that diet could only explain a relatively small percentage of caries risk because of the introduction and widespread use of fluoride toothpastes (48, 54, 55, 56). However in 2009, Anderson et al conducted an evidence analysis of sucrose intake (quantity and patterns) and dental caries and reported that there was a significant relationship between frequency of sucrose intake and dental caries but not overall quantity (57). Konig and Navia (58) provided four inherent limitations in quantifying the relationship between dietary sources of sugars and dental caries: (a) variability in sugar consumption patterns that alter duration of exposure of the teeth to the sugars; (b) lack of specificity provided by diet recalls or food diaries, which are limited to an approximation of self-reported intake of actual sugars and eating patterns; (c) the differences in data timing—in other words, that sugar intake patterns can be calculated annually, but caries formation can take several years; and (d) other factors including fluoride, calcium, and phosphorus in the diet, along with oral hygiene habits and education level, all of which influence caries risk (58).
The results of the 2001 National Institutes of Health Consensus Development Conference on Caries at which 69 studies on diet and caries published between 1980 and 2000 were reviewed showed that only two found a strong diet-caries relationship, 16 showed a moderate relationship, and 18 demonstrated a weak relationship (56). The authors did not differentiate between sugars consumed as sucrose and other monosaccharides and disaccharides; however, these authors concluded that diets that promote coronal caries also promote root caries. They emphasized that the reviewed studies differed from sugar-caries studies published in the decades before fluoride. Although the articles reviewed indicated a decline in caries risk in relation to sugar intake, they attributed the relative drop to fluoride use. The evidence for the diet-caries relationship is clear in their conclusion that “sugar consumption is likely to be a more powerful indicator for risk of caries infection in persons that don’t have regular exposure to fluoride” (49). This relationship has been further supported by relevant articles (34, 51, 57).
As the per capita consumption of sucrose increased in England and the United States in the last 100 years, the prevalence of caries rose (51). Since the later part of the twentieth century, sugar intake by adults and children has increased considerably; per capita consumption of added sugars increased 23% from 1970 to 1999 (50, 59). Added sugars intake increased in the period from 1989 to 1991 to the period from 1994 to 1996, an increase from 13.2% to 15.8% of total energy intake (60). Using the NHANES 2004 data, at that time Americans consumed an average of 22.4 teaspoons of sugar daily (55). In 2005 to 2006, the most frequently reported source of added sugars in the US diet was nondiet sodas, energy drinks, and sport drinks, which accounted for approximately 35% of total intake of sugars (52).
In humans, the presence of sucrose in the mouth increases the volume and rate of plaque formation. Sucrose has a unique role in permitting bacteria to colonize on the teeth. When high concentrations of sucrose are present, S. mutans is able to produce extracellular polysaccharides, glucans, which form an organic matrix on the tooth. These insoluble, sticky polymers permit bacterial colonies to adhere to the tooth. In addition to glucans, S. mutans produces intracellular polysaccharides, primarily fructans, from sucrose that are stored and used in glycolysis when dietary carbohydrates are unavailable.
The critical concentration of carbohydrate in a food that will cause human caries is unknown. The Hopewood House Study showed that children eating diets containing complex carbohydrates but few refined sugars had low caries increments (61). In a longitudinal study of school children in England where the fluoride level in the drinking water was low, the relationship between sugar intake and caries increment was examined; the highest significant correlation was between grams of sugar eaten daily and caries experience (62).
The other monosaccharides and disaccharides—glucose, fructose, maltose, and lactose—found in fruits, dairy products, and processed foods are also readily used by oral microorganisms. These sugars diffuse rapidly through dental plaque to become available for bacterial fermentation. Within a few minutes of ingestion, fructose and glucose cause a decline in plaque pH similar to sucrose; thus, they are considered as cariogenic as sucrose.
When eaten with meals, fruits pose a lower caries risk than when eaten alone as a snack. For citrus fruits and melons, this is attributed to the high water content and the presence of citric acid (citrus only), which stimulates saliva secretion; for others it’s because the combination of foods and increased salivary flow has the potential to modulate the salivary pH. Fresh fruits vary in sucrose content from 10% to 15% by weight in apples, bananas, and some grapes; 7% to 8% in citrus fruits; and to 2% in berries, cherries, and pears. Foods with a high acid content may prevent bacterial fermentation but cause enamel erosion.
Sugars in solution (e.g., beverages) have been considered less harmful to teeth than solid sweets because beverages clear the mouth quickly. In 1940, however, Stephan showed that a 10% glucose rinse lowered the plaque pH to less than 5.5 (63). The total amount of sugars in carbonated beverages, fruit drinks, and fruit juices is approximately 10%; and sport drinks contain approximately 4.4% total sugars. Based on sugar content, acidity, and changes in plaque pH after rinsing with these beverages, all of them appear to have similar cariogenic potential (64). Use of sugar-sweetened soft drinks three or more times between meals on a daily basis increases odds of having a high decayed-missing-filled teeth (DMFT) score. However, over time, food manufacturers have replaced some of the sucrose in beverages with high-fructose corn syrup, saccharin, or aspartame. Whether beverages formulated with high-fructose corn syrup are less cariogenic is unknown. Sports and energy drinks have a low pH associated with increased risk of caries (<5.5) (65, 66). Drinking sugarsweetened tea or coffee over an extended period of time can lead to enamel dissolution.
Sugar alcohols notably seen in sugar-free gums and beverages can have a positive impact on caries risk (51, 67, 68, 69). Examples include sorbitol, xylitol, mannitol, erythritol, and isomalt. Sugar-free gums with these polyols serve to stimulate saliva, thereby speeding clearance of fermentable carbohydrates from the oral cavity and serving as an oral buffer (51, 69). Chewing sugar-free gum following meals and snacks when brushing is not possible is a reasonable caries risk-reduction measure.
Frequent use of chewing gum sweetened with xylitol or xylitol/sorbitol mixtures causes significant reductions in dental plaque as well as plaque and saliva levels of S. mutans (67, 68). Gum chewing stimulates salivary flow and pushes saliva into the interproximal area, where salivary buffers can neutralize bacterial acids. Chewing also removes food particles from plaque and the soft tissues. The net result is that the stimulation of salivary flow caused by the physical act of chewing, coupled with the helpful effects of a noncaloric and noncariogenic sweetener, can be beneficial to oral health by “neutralizing” the plaque bacteria’s acid response to fermentable carbohydrate-containing foods.
Only gold members can continue reading. Log In or Register to continue