A. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance).
B. The individual finds it difficult to control the worry.
C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms present for more days than not for the past 6 months): (1) restlessness or feeling keyed up or on edge; (2) being easily fatigued; (3) difficulty concentrating or mind going blank; (4) irritability; (5) muscle tension; (6) sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep).
D. The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
E. The disturbance is not attributable to the physiologic effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism).
F. The disturbance is not better explained by another mental disorder (e.g., anxiety or worry about having panic attacks in panic disorder, negative evaluation in social anxiety disorder [social phobia], contamination or other obsessions in obsessive-compulsive disorder, separation from attachment figures in separation anxiety disorder, reminders of traumatic events in posttraumatic stress disorder, gaining weight in anorexia nervosa, physical complaints in somatic symptom disorder, perceived appearance flaws in body dysmorphic disorder, having a serious illness in illness anxiety disorder, or the content of delusional beliefs in schizophrenia or delusional disorder).
Source: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC, American Psychiatric Association, 2013.
Etiology and Pathophysiology All anxiogenic agents act on the γ-aminobutyric acid (GABA)A receptor/chloride ion channel complex, implicating this neurotransmitter system in the pathogenesis of anxiety and panic attacks. Benzodiazepines are thought to bind two separate GABAA receptor sites: type I, which has a broad neuroanatomic distribution, and type II, which is concentrated in the hippocampus, striatum, and neocortex. The antianxiety effects of the various benzodiazepines are influenced by their relative binding to alpha 2 and 3 subunits of the GABAA receptor, and sedation and memory impairment to the alpha 1 subunit, Serotonin (5-hydroxytryptamine [5-HT]) and 3α-reduced neuroactive steroids (allosteric modulators of GABAA) also appear to have a role in anxiety, and buspirone, a partial 5-HT1A receptor agonist, and certain 5-HT2A and 5-HT2C receptor antagonists (e.g., nefazodone) may have beneficial effects.
PHOBIC DISORDERS
Clinical Manifestations The cardinal feature of phobic disorders is a marked and persistent fear of objects or situations, exposure to which results in an immediate anxiety reaction. The patient avoids the phobic stimulus, and this avoidance usually impairs occupational or social functioning. Panic attacks may be triggered by the phobic stimulus or may occur spontaneously. Unlike patients with other anxiety disorders, individuals with phobias usually experience anxiety only in specific situations. Common phobias include fear of closed spaces (claustrophobia), fear of blood, and fear of flying. Social phobia is distinguished by a specific fear of social or performance situations in which the individual is exposed to unfamiliar individuals or to possible examination and evaluation by others. Examples include having to converse at a party, use public restrooms, and meet strangers. In each case, the affected individual is aware that the experienced fear is excessive and unreasonable given the circumstance. The specific content of a phobia may vary across gender, ethnic, and cultural boundaries.
Phobic disorders are common, affecting ~7–9% of the population. Twice as many females are affected than males. Full criteria for diagnosis are usually satisfied first in early adulthood, but behavioral avoidance of unfamiliar people, situations, or objects dating from early childhood is common.
In one study of female twins, concordance rates for agoraphobia, social phobia, and animal phobia were found to be 23% for monozygotic twins and 15% for dizygotic twins. A twin study of fear conditioning, a model for the acquisition of phobias, demonstrated a heritability of 35–45%. Animal studies of fear conditioning have indicated that processing of the fear stimulus occurs through the lateral nucleus of the amygdala, extending through the central nucleus and projecting to the periaqueductal gray region, lateral hypothalamus, and paraventricular hypothalamus.
STRESS DISORDERS
Clinical Manifestations Patients may develop anxiety after exposure to extreme traumatic events such as the threat of personal death or injury or the death of a loved one. The reaction may occur shortly after the trauma (acute stress disorder) or be delayed and subject to recurrence (PTSD) (Table 466-6). In both syndromes, individuals experience associated symptoms of detachment and loss of emotional responsivity. The patient may feel depersonalized and unable to recall specific aspects of the trauma, although typically it is reexperienced through intrusions in thought, dreams, or flashbacks, particularly when cues of the original event are present. Patients often actively avoid stimuli that precipitate recollections of the trauma and demonstrate a resulting increase in vigilance, arousal, and startle response. Patients with stress disorders are at risk for the development of other disorders related to anxiety, mood, and substance abuse (especially alcohol). Between 5 and 10% of Americans will at some time in their life satisfy criteria for PTSD, with women more likely to be affected than men.
DIAGNOSTIC CRITERIA FOR POSTTRAUMATIC STRESS DISORDER |
Source: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC, American Psychiatric Association, 2013.
Risk factors for the development of PTSD include a past psychiatric history and personality characteristics of high neuroticism and extroversion. Twin studies show a substantial genetic influence on all symptoms associated with PTSD, with less evidence for an environmental effect.
Etiology and Pathophysiology It is hypothesized that in PTSD there is excessive release of norepinephrine from the locus coeruleus in response to stress and increased noradrenergic activity at projection sites in the hippocampus and amygdala. These changes theoretically facilitate the encoding of fear-based memories. Greater sympathetic responses to cues associated with the traumatic event occur in PTSD, although pituitary adrenal responses are blunted.
OBSESSIVE-COMPULSIVE DISORDER
Clinical Manifestations Obsessive-compulsive disorder (OCD) is characterized by obsessive thoughts and compulsive behaviors that impair everyday functioning. Fears of contamination and germs are common, as are handwashing, counting behaviors, and having to check and recheck such actions as whether a door is locked. The degree to which the disorder is disruptive for the individual varies, but in all cases, obsessive-compulsive activities take up >1 h per day and are undertaken to relieve the anxiety triggered by the core fear. Patients often conceal their symptoms, usually because they are embarrassed by the content of their thoughts or the nature of their actions. Physicians must ask specific questions regarding recurrent thoughts and behaviors, particularly if physical clues such as chafed and reddened hands or patchy hair loss (from repetitive hair pulling, or trichotillomania) are present. Comorbid conditions are common, the most frequent being depression, other anxiety disorders, eating disorders, and tics. OCD has a lifetime prevalence of 2–3% worldwide. Onset is usually gradual, beginning in early adulthood, but childhood onset is not rare. The disorder usually has a waxing and waning course, but some cases may show a steady deterioration in psychosocial functioning.
Etiology and Pathophysiology A genetic contribution to OCD is suggested by twin studies, but no susceptibility gene for OCD has been identified to date. Family studies show an aggregation of OCD with Tourette’s disorder, and both are more common in males and in first-born children.
The anatomy of obsessive-compulsive behavior is thought to include the orbital frontal cortex, caudate nucleus, and globus pallidus. The caudate nucleus appears to be involved in the acquisition and maintenance of habit and skill learning, and interventions that are successful in reducing obsessive-compulsive behaviors also decrease metabolic activity measured in the caudate.
MOOD DISORDERS
Mood disorders are characterized by a disturbance in the regulation of mood, behavior, and affect. Mood disorders are subdivided into (1) depressive disorders, (2) bipolar disorders, and (3) depression in association with medical illness or alcohol and substance abuse (Chaps. 467 through 471e). Major depressive disorder (MDD) is differentiated from bipolar disorder by the absence of a manic or hypomanic episode. The relationship between pure depressive syndromes and bipolar disorders is not well understood; MDD is more frequent in families of bipolar individuals, but the reverse is not true. In the Global Burden of Disease Study conducted by the World Health Organization, unipolar major depression ranked fourth among all diseases in terms of disability-adjusted life-years and was projected to rank second by the year 2020. In the United States, lost productivity directly related to mood disorders has been estimated at $55.1 billion per year.
DEPRESSION IN ASSOCIATION WITH MEDICAL ILLNESS
Depression occurring in the context of medical illness is difficult to evaluate. Depressive symptomatology may reflect the psychological stress of coping with the disease, may be caused by the disease process itself or by the medications used to treat it, or may simply coexist in time with the medical diagnosis.
Virtually every class of medication includes some agent that can induce depression. Antihypertensive drugs, anticholesterolemic agents, and antiarrhythmic agents are common triggers of depressive symptoms. Iatrogenic depression should also be considered in patients receiving glucocorticoids, antimicrobials, systemic analgesics, antiparkinsonian medications, and anticonvulsants. To decide whether a causal relationship exists between pharmacologic therapy and a patient’s change in mood, it may sometimes be necessary to undertake an empirical trial of an alternative medication.
Between 20 and 30% of cardiac patients manifest a depressive disorder; an even higher percentage experience depressive symptomatology when self-reporting scales are used. Depressive symptoms following unstable angina, myocardial infarction, cardiac bypass surgery, or heart transplant impair rehabilitation and are associated with higher rates of mortality and medical morbidity. Depressed patients often show decreased variability in heart rate (an index of reduced parasympathetic nervous system activity), which may predispose individuals to ventricular arrhythmia and increased morbidity. Depression also appears to increase the risk of developing coronary heart disease, possibly through increased platelet aggregation. TCAs are contraindicated in patients with bundle branch block, and TCA-induced tachycardia is an additional concern in patients with congestive heart failure. SSRIs appear not to induce ECG changes or adverse cardiac events and thus are reasonable first-line drugs for patients at risk for TCA-related complications. SSRIs may interfere with hepatic metabolism of anticoagulants, however, causing increased anticoagulation.
In patients with cancer, the mean prevalence of depression is 25%, but depression occurs in 40–50% of patients with cancers of the pancreas or oropharynx. This association is not due to the effect of cachexia alone, as the higher prevalence of depression in patients with pancreatic cancer persists when compared to those with advanced gastric cancer. Initiation of antidepressant medication in cancer patients has been shown to improve quality of life as well as mood. Psychotherapeutic approaches, particularly group therapy, may have some effect on short-term depression, anxiety, and pain symptoms.
Depression occurs frequently in patients with neurologic disorders, particularly cerebrovascular disorders, Parkinson’s disease, dementia, multiple sclerosis, and traumatic brain injury. One in five patients with left-hemisphere stroke involving the dorsolateral frontal cortex experiences major depression. Late-onset depression in otherwise cognitively normal individuals increases the risk of a subsequent diagnosis of Alzheimer’s disease. All classes of antidepressant agents are effective against these depressions, as are, in some cases, stimulant compounds.
The reported prevalence of depression in patients with diabetes mellitus varies from 8 to 27%, with the severity of the mood state correlating with the level of hyperglycemia and the presence of diabetic complications. Treatment of depression may be complicated by effects of antidepressive agents on glycemic control. MAOIs can induce hypoglycemia and weight gain, whereas TCAs can produce hyperglycemia and carbohydrate craving. SSRIs and SNRIs, like MAOIs, may reduce fasting plasma glucose, but they are easier to use and may also improve dietary and medication compliance.
Hypothyroidism is frequently associated with features of depression, most commonly depressed mood and memory impairment. Hyperthyroid states may also present in a similar fashion, usually in geriatric populations. Improvement in mood usually follows normalization of thyroid function, but adjunctive antidepressant medication is sometimes required. Patients with subclinical hypothyroidism can also experience symptoms of depression and cognitive difficulty that respond to thyroid replacement.
The lifetime prevalence of depression in HIV-positive individuals has been estimated at 22–45%. The relationship between depression and disease progression is multifactorial and likely to involve psychological and social factors, alterations in immune function, and central nervous system (CNS) disease. Chronic hepatitis C infection is also associated with depression, which may worsen with interferon-α treatment.
Some chronic disorders of uncertain etiology, such as chronic fatigue syndrome (Chap. 464e) and fibromyalgia (Chap. 396), are strongly associated with depression and anxiety; patients may benefit from antidepressant treatment or anticonvulsant agents such as pregabalin.
DEPRESSIVE DISORDERS
Clinical Manifestations Major depression is defined as depressed mood on a daily basis for a minimum duration of 2 weeks (Table 466-7). An episode may be characterized by sadness, indifference, apathy, or irritability and is usually associated with changes in sleep patterns, appetite, and weight; motor agitation or retardation; fatigue; impaired concentration and decision making; feelings of shame or guilt; and thoughts of death or dying. Patients with depression have a profound loss of pleasure in all enjoyable activities, exhibit early morning awakening, feel that the dysphoric mood state is qualitatively different from sadness, and often notice a diurnal variation in mood (worse in morning hours). Patients experiencing bereavement or grief may exhibit many of the same signs and symptoms of major depression, although the emphasis is usually on feelings of emptiness and loss, rather than anhedonia and loss of self-esteem, and the duration is usually limited. In certain cases, however, the diagnosis of major depression may be warranted even in the context of a significant loss.
CRITERIA FOR A MAJOR DEPRESSIVE EPISODE |
Source: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC, American Psychiatric Association, 2013.
Approximately 15% of the population experiences a major depressive episode at some point in life, and 6–8% of all outpatients in primary care settings satisfy diagnostic criteria for the disorder. Depression is often undiagnosed, and even more frequently, it is treated inadequately. If a physician suspects the presence of a major depressive episode, the initial task is to determine whether it represents unipolar or bipolar depression or is one of the 10–15% of cases that are secondary to general medical illness or substance abuse. Physicians should also assess the risk of suicide by direct questioning, as patients are often reluctant to verbalize such thoughts without prompting. If specific plans are uncovered or if significant risk factors exist (e.g., a past history of suicide attempts, profound hopelessness, concurrent medical illness, substance abuse, or social isolation), the patient must be referred to a mental health specialist for immediate care. The physician should specifically probe each of these areas in an empathic and hopeful manner, being sensitive to denial and possible minimization of distress. The presence of anxiety, panic, or agitation significantly increases near-term suicidal risk. Approximately 4–5% of all depressed patients will commit suicide; most will have sought help from physicians within 1 month of their deaths.
In some depressed patients, the mood disorder does not appear to be episodic and is not clearly associated with either psychosocial dysfunction or change from the individual’s usual experience in life. Persistent depressive disorder (dysthymic disorder) consists of a pattern of chronic (at least 2 years), ongoing depressive symptoms that are usually less severe and/or less numerous than those found in major depression, but the functional consequences may be equivalent to or even greater; the two conditions are sometimes difficult to separate and can occur together (“double depression”). Many patients who exhibit a profile of pessimism, disinterest, and low self-esteem respond to antidepressant treatment. Persistent and chronic depressive disorders occur in approximately 2% of the general population.
Depression is approximately twice as common in women as in men, and the incidence increases with age in both sexes. Twin studies indicate that the liability to major depression of early onset (before age 25) is largely genetic in origin. Negative life events can precipitate and contribute to depression, but genetic factors influence the sensitivity of individuals to these stressful events. In most cases, both biologic and psychosocial factors are involved in the precipitation and unfolding of depressive episodes. The most potent stressors appear to involve death of a relative, assault, or severe marital or relationship problems.
Unipolar depressive disorders usually begin in early adulthood and recur episodically over the course of a lifetime. The best predictor of future risk is the number of past episodes; 50–60% of patients who have a first episode have at least one or two recurrences. Some patients experience multiple episodes that become more severe and frequent over time. The duration of an untreated episode varies greatly, ranging from a few months to ≥1 year. The pattern of recurrence and clinical progression in a developing episode are also variable. Within an individual, the nature of episodes (e.g., specific presenting symptoms, frequency and duration) may be similar over time. In a minority of patients, a severe depressive episode may progress to a psychotic state; in elderly patients, depressive symptoms may be associated with cognitive deficits mimicking dementia (“pseudodementia”). A seasonal pattern of depression, called seasonal affective disorder, may manifest with onset and remission of episodes at predictable times of the year. This disorder is more common in women, whose symptoms are anergy, fatigue, weight gain, hypersomnia, and episodic carbohydrate craving. The prevalence increases with distance from the equator, and improvement may occur by altering light exposure.
Etiology and Pathophysiology Although evidence for genetic transmission of unipolar depression is not as strong as in bipolar disorder, monozygotic twins have a higher concordance rate (46%) than dizygotic siblings (20%), with little support for any effect of a shared family environment.
Neuroendocrine abnormalities that reflect the neurovegetative signs and symptoms of depression include: (1) increased cortisol and corticotropin-releasing hormone (CRH) secretion, (2) an increase in adrenal size, (3) a decreased inhibitory response of glucocorticoids to dexamethasone, and (4) a blunted response of thyroid-stimulating hormone (TSH) level to infusion of thyroid-releasing hormone (TRH). Antidepressant treatment leads to normalization of these abnormalities. Major depression is also associated with changes in levels of proinflammatory cytokines and neurotrophins.
Diurnal variations in symptom severity and alterations in circadian rhythmicity of a number of neurochemical and neurohumoral factors suggest that biologic differences may be secondary to a primary defect in regulation of biologic rhythms. Patients with major depression show consistent findings of a decrease in rapid eye movement (REM) sleep onset (REM latency), an increase in REM density, and, in some subjects, a decrease in stage IV delta slow-wave sleep.
Although antidepressant drugs inhibit neurotransmitter uptake within hours, their therapeutic effects typically emerge over several weeks, implicating adaptive changes in second messenger systems and transcription factors as possible mechanisms of action.
The pathogenesis of depression is discussed in detail in Chap. 465e.
TREATMENT | DEPRESSIVE DISORDERS |
Treatment planning requires coordination of short-term strategies to induce remission combined with longer term maintenance designed to prevent recurrence. The most effective intervention for achieving remission and preventing relapse is medication, but combined treatment, incorporating psychotherapy to help the patient cope with decreased self-esteem and demoralization, improves outcome (Fig. 466-1). Approximately 40% of primary care patients with depression drop out of treatment and discontinue medication if symptomatic improvement is not noted within a month, unless additional support is provided. Outcome improves with (1) increased intensity and frequency of visits during the first 4–6 weeks of treatment, (2) supplemental educational materials, and (3) psychiatric consultation as indicated. Despite the widespread use of SSRIs and other second-generation antidepressant drugs, there is no convincing evidence that these classes of antidepressants are more efficacious than TCAs. Between 60 and 70% of all depressed patients respond to any drug chosen, if it is given in a sufficient dose for 6–8 weeks.
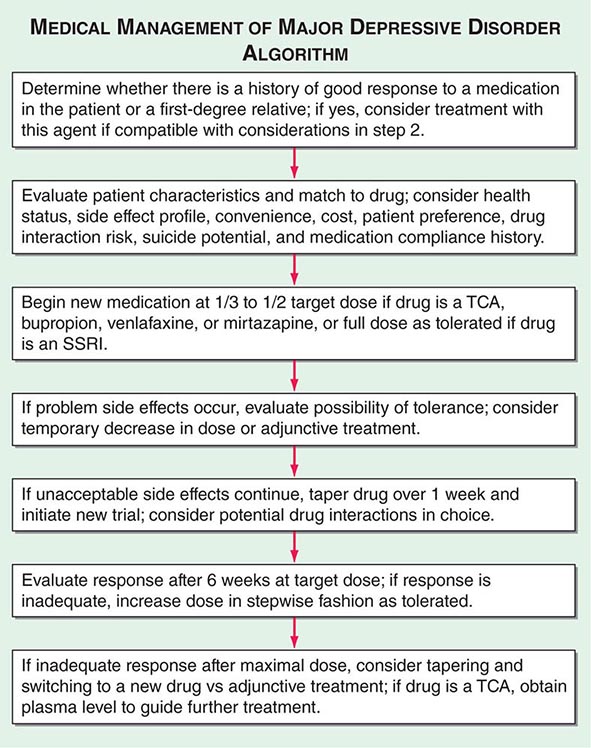
FIGURE 466-1 A guideline for the medical management of major depressive disorder. SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
A rational approach to selecting which antidepressant to use involves matching the patient’s preference and medical history with the metabolic and side effect profile of the drug (Tables 466-4 and 466-5). A previous response, or a family history of a positive response, to a specific antidepressant often suggests that that drug be tried first. Before initiating antidepressant therapy, the physician should evaluate the possible contribution of comorbid illnesses and consider their specific treatment. In individuals with suicidal ideation, particular attention should be paid to choosing a drug with low toxicity if taken in overdose. Newer antidepressant drugs are distinctly safer in this regard; nevertheless, the advantages of TCAs have not been completely superseded. The existence of generic equivalents makes TCAs relatively cheap, and for secondary tricyclics, particularly nortriptyline and desipramine, well-defined relationships among dose, plasma level, and therapeutic response exist. The steady-state plasma level achieved for a given drug dose can vary more than 10-fold between individuals, and plasma levels may help in interpreting apparent resistance to treatment and/or unexpected drug toxicity. The principal side effects of TCAs are antihistamine (sedation) and anticholinergic (constipation, dry mouth, urinary hesitancy, blurred vision). TCAs are contraindicated in patients with serious cardiovascular risk factors, and overdoses of tricyclic agents can be lethal, with desipramine carrying the greatest risk. It is judicious to prescribe only a 10-day supply when suicide is a risk. Most patients require a daily dose of 150–200 mg of imipramine or amitriptyline or its equivalent to achieve a therapeutic blood level of 150–300 ng/mL and a satisfactory remission; some patients show a partial effect at lower doses. Geriatric patients may require a low starting dose and slow escalation. Ethnic differences in drug metabolism are significant, with Hispanic, Asian, and black patients generally requiring lower doses than whites to achieve a comparable blood level. P450 profiling using genetic chip technology may be clinically useful in predicting individual sensitivity.
Second-generation antidepressants are similar to tricyclics in their effect on neurotransmitter reuptake, although some also have specific actions on catecholamine and indolamine receptors as well. Amoxapine is a dibenzoxazepine derivative that blocks norepinephrine and serotonin reuptake and has a metabolite that shows a degree of dopamine blockade. Long-term use of this drug carries a risk of tardive dyskinesia. Maprotiline is a potent noradrenergic reuptake blocker that has little anticholinergic effect but may produce seizures. Bupropion is a novel antidepressant whose mechanism of action is thought to involve enhancement of noradrenergic function. It has no anticholinergic, sedating, or orthostatic side effects and has a low incidence of sexual side effects. It may, however, be associated with stimulant-like side effects, may lower seizure threshold, and has an exceptionally short half-life, requiring frequent dosing. An extended-release preparation is available.
SSRIs such as fluoxetine, sertraline, paroxetine, citalopram, and escitalopram cause a lower frequency of anticholinergic, sedating, and cardiovascular side effects but a possibly greater incidence of gastrointestinal complaints, sleep impairment, and sexual dysfunction than do TCAs. Akathisia, involving an inner sense of restlessness and anxiety in addition to increased motor activity, may also be more common, particularly during the first week of treatment. One concern is the risk of “serotonin syndrome,” which is thought to result from hyperstimulation of brainstem 5-HT1A receptors and characterized by myoclonus, agitation, abdominal cramping, hyperpyrexia, hypertension, and potentially death. Serotonergic agonists taken in combination should be monitored closely for this reason. Considerations such as half-life, compliance, toxicity, and drug-drug interactions may guide the choice of a particular SSRI. Fluoxetine and its principal active metabolite, norfluoxetine, for example, have a combined half-life of almost 7 days, resulting in a delay of 5 weeks before steady-state levels are achieved and a similar delay for complete drug excretion once its use is discontinued. All the SSRIs may impair sexual function, resulting in diminished libido, impotence, or difficulty in achieving orgasm. Sexual dysfunction frequently results in noncompliance and should be asked about specifically. Sexual dysfunction can sometimes be ameliorated by lowering the dose, by instituting weekend drug holidays (two or three times a month), or by treatment with amantadine (100 mg tid), bethanechol (25 mg tid), buspirone (10 mg tid), or bupropion (100–150 mg/d). Paroxetine appears to be more anticholinergic than either fluoxetine or sertraline, and sertraline carries a lower risk of producing an adverse drug interaction than the other two. Rare side effects of SSRIs include angina due to vasospasm and prolongation of the prothrombin time. Escitalopram is the most specific of currently available SSRIs and appears to have no specific inhibitory effects on the P450 system.
Venlafaxine, desvenlafaxine, duloxetine, vilazodone, vortioxetine, and levomilnacipran block the reuptake of both norepinephrine and serotonin but produce relatively little in the way of traditional tricyclic side effects. Unlike the SSRIs, venlafaxine and vortioxetine have relatively linear dose-response curves. Patients on immediate release venlafaxine should be monitored for a possible increase in diastolic blood pressure, and multiple daily dosing is required because of the drug’s short half-life. An extended-release form is available and has a somewhat lower incidence of gastrointestinal side effects. Mirtazapine is a TCA that has a unique spectrum of activity. It increases noradrenergic and serotonergic neurotransmission through a blockade of central α2-adrenergic receptors and postsynaptic 5-HT2 and 5-HT3 receptors. It is also strongly antihistaminic and, as such, may produce sedation. Levomilnacipran is the most noradrenergic of the SNRIs and theoretically may be appropriate for patients with more severe fatigue and anergia.
With the exception of citalopram and escitalopram, each of the SSRIs may inhibit one or more cytochrome P450 enzymes. Depending on the specific isoenzyme involved, the metabolism of a number of concomitantly administered medications can be dramatically affected. Fluoxetine and paroxetine, for example, by inhibiting 2D6, can cause dramatic increases in the blood level of type 1C antiarrhythmics, whereas sertraline, by acting on 3A4, may alter blood levels of carbamazepine or digoxin. Depending on drug specificity for a particular CYP enzyme for its own metabolism, concomitant medications or dietary factors, such as grapefruit juice, may in turn affect the efficacy or toxicity of the SSRI.
The MAOIs are highly effective, particularly in atypical depression, but the risk of hypertensive crisis following intake of tyramine-containing food or sympathomimetic drugs makes them inappropriate as first-line agents. Transdermal selegiline may avert this risk at low dose. Common side effects include orthostatic hypotension, weight gain, insomnia, and sexual dysfunction. MAOIs should not be used concomitantly with SSRIs, because of the risk of serotonin syndrome, or with TCAs, because of possible hyperadrenergic effects.
Electroconvulsive therapy is at least as effective as medication, but its use is reserved for treatment-resistant cases and delusional depressions. Transcranial magnetic stimulation (TMS) is approved for treatment-resistant depression and has been shown to have efficacy in several controlled trials. Vagus nerve stimulation (VNS) has also recently been approved for treatment-resistant depression, but its degree of efficacy is controversial. Deep brain stimulation and ketamine, a glutamatergic antagonist, are experimental approaches for treatment-resistant cases.
Regardless of the treatment undertaken, the response should be evaluated after ~2 months. Three-quarters of patients show improvement by this time, but if remission is inadequate, the patient should be questioned about compliance, and an increase in medication dose should be considered if side effects are not troublesome. If this approach is unsuccessful, referral to a mental health specialist is advised. Strategies for treatment then include selection of an alternative drug, combinations of antidepressants, and/or adjunctive treatment with other classes of drugs, including lithium, thyroid hormone, atypical antipsychotic agents, and dopamine agonists. A large randomized trial (STAR-D) was unable to show preferential efficacy, but the addition of certain atypical antipsychotic drugs (quetiapine extended-release; aripiprazole) has received FDA approval, as has usage of a combined medication, olanzapine and fluoxetine (Symbyax). Patients whose response to an SSRI wanes over time may benefit from the addition of buspirone (10 mg tid) or pindolol (2–5 mg tid) or small amounts of a TCA such as desipramine (25 mg bid or tid). Most patients will show some degree of response, but aggressive treatment should be pursued until remission is achieved, and drug treatment should be continued for at least 6–9 more months to prevent relapse. In patients who have had two or more episodes of depression, indefinite maintenance treatment should be considered.
It is essential to educate patients both about depression and the benefits and side effects of medications they are receiving. Advice about stress reduction and cautions that alcohol may exacerbate depressive symptoms and impair drug response are helpful. Patients should be given time to describe their experience, their outlook, and the impact of the depression on them and their families. Occasional empathic silence may be as helpful for the treatment alliance as verbal reassurance. Controlled trials have shown that cognitive-behavioral and interpersonal therapies are effective in improving psychological and social adjustment and that a combined treatment approach is more successful than medication alone for many patients.
BIPOLAR DISORDER
Clinical Manifestations Bipolar disorder is characterized by unpredictable swings in mood from mania (or hypomania) to depression. Some patients suffer only from recurrent attacks of mania, which in its pure form is associated with increased psychomotor activity; excessive social extroversion; decreased need for sleep; impulsivity and impairment in judgment; and expansive, grandiose, and sometimes irritable mood (Table 466-8). In severe mania, patients may experience delusions and paranoid thinking indistinguishable from schizophrenia. One-half of patients with bipolar disorder present with a mixture of psychomotor agitation and activation with dysphoria, anxiety, and irritability. It may be difficult to distinguish mixed mania from agitated depression. In some bipolar patients (bipolar II disorder), the full criteria for mania are lacking, and the requisite recurrent depressions are separated by periods of mild activation and increased energy (hypomania). In cyclothymic disorder, there are numerous hypomanic periods, usually of relatively short duration, alternating with clusters of depressive symptoms that fail, either in severity or duration, to meet the criteria of major depression. The mood fluctuations are chronic and should be present for at least 2 years before the diagnosis is made.
CRITERIA FOR A MANIC EPISODE |
Source: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC, American Psychiatric Association, 2013.
Manic episodes typically emerge over a period of days to weeks, but onset within hours is possible, usually in the early morning hours. An untreated episode of either depression or mania can be as short as several weeks or last as long as 8–12 months, and rare patients have an unremitting chronic course. The term rapid cycling is used for patients who have four or more episodes of either depression or mania in a given year. This pattern occurs in 15% of all patients, almost all of whom are women. In some cases, rapid cycling is linked to an underlying thyroid dysfunction, and in others, it is iatrogenically triggered by prolonged antidepressant treatment. Approximately one-half of patients have sustained difficulties in work performance and psychosocial functioning, with depressive phases being more responsible for impairment than mania.
Bipolar disorder is common, affecting ~1.5% of the population in the United States. Onset is typically between 20 and 30 years of age, but many individuals report premorbid symptoms in late childhood or early adolescence. The prevalence is similar for men and women; women are likely to have more depressive and men more manic episodes over a lifetime.
Differential Diagnosis The differential diagnosis of mania includes secondary mania induced by stimulant or sympathomimetic drugs, hyperthyroidism, AIDS, and neurologic disorders such as Huntington’s or Wilson’s disease and cerebrovascular accidents. Comorbidity with alcohol and substance abuse is common, either because of poor judgment and increased impulsivity or because of an attempt to self-treat the underlying mood symptoms and sleep disturbances.
Etiology and Pathophysiology Genetic predisposition to bipolar disorder is evident from family studies; the concordance rate for monozygotic twins approaches 80%. Patients with bipolar disorder also appear to have altered circadian rhythmicity, and lithium may exert its therapeutic benefit through a resynchronization of intrinsic rhythms keyed to the light/dark cycle.
TREATMENT | BIPOLAR DISORDER |
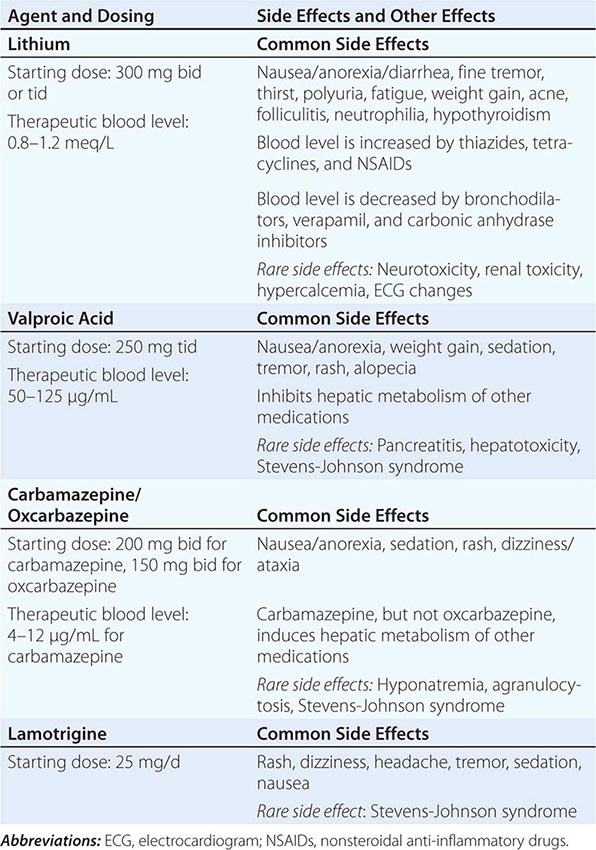
(Table 466-9) Lithium carbonate is the mainstay of treatment in bipolar disorder, although sodium valproate and carbamazepine, as well as a number of second-generation antipsychotic agents (aripiprazole, asenapine, olanzapine, quetiapine, risperidone, ziprasidone), also have FDA approval for the treatment of acute mania. Oxcarbazepine is not FDA approved, but appears to enjoy carbamazepine’s spectrum of efficacy. The response rate to lithium carbonate is 70–80% in acute mania, with beneficial effects appearing in 1–2 weeks. Lithium also has a prophylactic effect in prevention of recurrent mania and, to a lesser extent, in the prevention of recurrent depression. A simple cation, lithium is rapidly absorbed from the gastrointestinal tract and remains unbound to plasma or tissue proteins. Some 95% of a given dose is excreted unchanged through the kidneys within 24 h.
CLINICAL PHARMACOLOGY OF MOOD STABILIZERS |
Serious side effects from lithium are rare, but minor complaints such as gastrointestinal discomfort, nausea, diarrhea, polyuria, weight gain, skin eruptions, alopecia, and edema are common. Over time, urine-concentrating ability may be decreased, but significant nephrotoxicity does not usually occur. Lithium exerts an antithyroid effect by interfering with the synthesis and release of thyroid hormones. More serious side effects include tremor, poor concentration and memory, ataxia, dysarthria, and incoordination. There is suggestive, but not conclusive, evidence that lithium is teratogenic, inducing cardiac malformations in the first trimester.
In the treatment of acute mania, lithium is initiated at 300 mg bid or tid, and the dose is then increased by 300 mg every 2–3 days to achieve blood levels of 0.8–1.2 meq/L. Because the therapeutic effect of lithium may not appear until after 7–10 days of treatment, adjunctive usage of lorazepam (1–2 mg every 4 h) or clonazepam (0.5–1 mg every 4 h) may be beneficial to control agitation. Antipsychotics are indicated in patients with severe agitation who respond only partially to benzodiazepines. Patients using lithium should be monitored closely, since the blood levels required to achieve a therapeutic benefit are close to those associated with toxicity.
Valproic acid may be better than lithium for patients who experience rapid cycling (i.e., more than four episodes a year) or who present with a mixed or dysphoric mania. Tremor and weight gain are the most common side effects; hepatotoxicity and pancreatitis are rare toxicities.
The recurrent nature of bipolar mood disorder necessitates maintenance treatment. A sustained blood lithium level of at least 0.8 meq/L is important for optimal prophylaxis and has been shown to reduce the risk of suicide, a finding not yet apparent for other mood stabilizers. Combinations of mood stabilizers together or with atypical antipsychotic drugs are sometimes required to maintain mood stability. Quetiapine extended release, olanzapine, risperidone, and lamotrigine have been approved for maintenance treatment as sole agents, in combination with lithium and with aripiprazole and ziprasidone as adjunctive drugs. Lurasidone, olanzapine/fluoxetine, and quetiapine are also approved to treat acute depressive episodes in bipolar disorder. Compliance is frequently an issue and often requires enlistment and education of concerned family members. Efforts to identify and modify psychosocial factors that may trigger episodes are important, as is an emphasis on lifestyle regularity. Antidepressant medications are sometimes required for the treatment of severe breakthrough depressions, but their use should generally be avoided during maintenance treatment because of the risk of precipitating mania or accelerating the cycle frequency. Loss of efficacy over time may be observed with any of the mood-stabilizing agents. In such situations, an alternative agent or combination therapy is usually helpful.
SOMATIC SYMPTOM DISORDER
Many patients presenting in general medical practice, perhaps as many as 5–7%, will experience a somatic symptom(s) as particularly distressing and preoccupying, to the point that it comes to dominate their thoughts, feelings, and beliefs and interferes to a varying degree with everyday functioning. Although the absence of a medical explanation for these complaints was historically emphasized as a diagnostic element, it has been recognized that the patient’s interpretation and elaboration of the experience is the critical defining factor and that patients with well-established medical causation may qualify for the diagnosis. Multiple complaints are typical, but severe single symptoms can occur as well. Comorbidity with depressive and anxiety disorders is common and may affect the severity of the experience and its functional consequences. Personality factors may be a significant risk factor, as may a low level of educational or socioeconomic status or a history of recent stressful life events. Cultural factors are relevant as well and should be incorporated into the evaluation. Individuals who have persistent preoccupations about having or acquiring a serious illness, but who do not have a specific somatic complaint, may qualify for a related diagnosis—illness anxiety disorder. The diagnosis of conversion disorder (functional neurologic symptom disorder) is used to specifically identify those individuals whose somatic complaints involve one or more symptoms of altered voluntary motor or sensory function that cannot be medically explained and that causes significant distress or impairment or requires medical evaluation.
In factitious illnesses, the patient consciously and voluntarily produces physical symptoms of illness. The term Munchausen’s syndrome is reserved for individuals with particularly dramatic, chronic, or severe factitious illness. In true factitious illness, the sick role itself is gratifying. A variety of signs, symptoms, and diseases have been either simulated or caused by factitious behavior, the most common including chronic diarrhea, fever of unknown origin, intestinal bleeding or hematuria, seizures, and hypoglycemia. Factitious disorder is usually not diagnosed until 5–10 years after its onset, and it can produce significant social and medical costs. In malingering, the fabrication derives from a desire for some external reward such as a narcotic medication or disability reimbursement.
FEEDING AND EATING DISORDERS
CLINICAL MANIFESTATIONS
Feeding and eating disorders constitute a group of conditions in which there is a persistent disturbance of eating or associated behaviors that significantly impair an individual’s physical health or psychosocial functioning. In DSM-5 the described categories (with the exception of pica) are defined to be mutually exclusive in a given episode, based on the understanding that although they are phenotypically similar in some ways, they differ in course, prognosis, and effective treatment interventions. Compared with DSM-IV-TR, three disorders (i.e., avoidant/restrictive food intake disorder, rumination disorder, pica) that were previously classified as disorders of infancy or childhood have been grouped together with the disorders of anorexia and bulimia nervosa. Binge-eating disorder is also now included as a formal diagnosis; the intent of each of these modifications is to encourage clinicians to be more specific in their codification of eating and feeding pathology.
PICA
Pica is diagnosed when the individual, over age 2, eats one or more nonnutritive, nonfood substances for a month or more and requires medical attention as a result. There is usually no specific aversion to food in general but a preferential choice to ingest substances such as clay, starch, soap, paper, or ash. The diagnosis requires the exclusion of specific culturally approved practices and has not been commonly found to be caused by a specific nutritional deficiency. Onset is most common in childhood but the disorder can occur in association with other major psychiatric conditions in adults. An association with pregnancy has been observed, but the condition is only diagnosed when medical risks are increased by the behavior.
RUMINATION DISORDER
In this condition, individuals who have no demonstrable associated gastrointestinal or other medical condition repeatedly regurgitate their food after eating and then either rechew or swallow it or spit it out. The behavior typically occurs on a daily basis and must persist for at least 1 month. Weight loss and malnutrition are common sequelae, and individuals may attempt to conceal their behavior, either by covering their mouth or through social avoidance while eating. In infancy, the onset is typically between 3 to 12 months, and the behavior may remit spontaneously, although in some it appears to be recurrent.
AVOIDANT/RESTRICTIVE FOOD INTAKE DISORDER
The cardinal feature of this disorder is avoidance or restriction of food intake, usually stemming from a lack of interest in or distaste of food and associated with weight loss, nutritional deficiency, dependency on nutritional supplementation, or marked impairment in psychosocial functioning, either alone or in combination. Culturally approved practices, such as fasting, or a lack of available food must be excluded as possible causes. The disorder is distinguished from anorexia nervosa by the presence of emotional factors, such as a fear of gaining weight and distortion of body image in the latter condition. Onset is usually in infancy or early childhood, but avoidant behaviors may persist into adulthood. The disorder is equally prevalent in males and females and is frequently comorbid with anxiety and cognitive and attention-deficit disorders and situations of familial stress. Developmental delay and functional deficits may be significant if the disorder is long-standing and unrecognized.
ANOREXIA NERVOSA
Individuals are diagnosed with anorexia nervosa if they restrict their caloric intake to a degree that their body weight deviates significantly from age, gender, health, and developmental norms and if they also exhibit a fear of gaining weight and an associated disturbance in body image. The condition is further characterized by differentiating those who achieve their weight loss predominantly through restricting intake or by excessive exercise (restricting type) from those who engage in recurrent binge eating and/or subsequent purging, self-induced vomiting, and usage of enemas, laxatives, or diuretics (binge-eating/purging type). Such subtyping is more state than trait specific, as individuals may transition from one profile to the other over time. Determination of whether an individual satisfies the primary criterion of significant low weight is complex and must be individualized, using all available historical information and comparison of body habitus to international body mass norms and guidelines.
Individuals with anorexia nervosa frequently lack insight into their condition and are in denial about possible medical consequences; they often are not comforted by their achieved weight loss and persist in their behaviors despite having met previously self-designated weight goals. Recent research has identified alterations in the circuitry of reward sensitivity and executive function in anorexia and implicated disturbances in frontal cortex and anterior insula regulation of interoceptive awareness of satiety and hunger. Neurochemical findings, including the role of ghrelin, remain controversial.
Onset is most common in adolescence, although onset in later life can occur. Many more females than males are affected, with a lifetime prevalence in women of up to 4%. The disorder appears most prevalent in postindustrialized and urbanized countries and is frequently comorbid with preexisting anxiety disorders. The medical consequences of prolonged anorexia nervosa are multisystemic and can be life-threatening in severe presentations. Changes in blood chemistry include leukopenia with lymphocytosis, elevations in blood urea nitrogen, and metabolic alkalosis and hypokalemia when purging is present. History and physical examination may reveal amenorrhea in females, skin abnormalities (petechiae, lanugo hair, dryness), and signs of hypometabolic function, including hypotension, hypothermia, and sinus bradycardia. Endocrine effects include hypogonadism, growth hormone resistance, and hypercortisolemia. Osteoporosis is a longer-term concern.
The course of the disorder is variable, with some individuals recovering after a single episode, while others exhibit recurrent episodes or a chronic course. Untreated anorexia has a mortality of 5.1/1000, the highest among psychiatric conditions. Maudsley family-based therapy has proven to be an effective therapy in younger individuals, with strict behavioral contingencies used when weight loss becomes critical. No pharmacologic intervention has proven to be specifically beneficial, but comorbid depression and anxiety should be treated. Weight gain should be undertaken gradually with a goal of 0.5 to 1 pound per week to prevent refeeding syndrome. Most individuals are able to achieve remission within 5 years of the original diagnosis.
BULIMIA NERVOSA
Bulimia nervosa describes individuals who engage in recurrent and frequent (at least once a week for 3 months) periods of binge eating and who then resort to compensatory behaviors, such as self-induced purging, enemas, use of laxatives, or excessive exercise to avoid weight gain. Binge eating itself is defined as excessive food intake in a prescribed period of time, usually <2 h. As in anorexia nervosa, disturbances in body image occur and promote the behavior, but unlike in anorexia, individuals are of normal weight or even somewhat overweight. Subjects typically describe a loss of control and express shame about their actions, and often relate that their episodes are triggered by feelings of negative self-esteem or social stresses. The lifetime prevalence in women is approximately 2%, with a 10:1 female-to-male ratio. The disorder typically begins in adolescence and may be persistent over a number of years. Transition to anorexia occurs in only 10–15% of cases. Many of the medical risks associated with bulimia nervosa parallel those of anorexia nervosa and are a direct consequence of purging, including fluid and electrolyte disturbances and conduction abnormalities. Physical examination often results in no specific findings, but dental erosion and parotid gland enlargement may be present. Effective treatment approaches include SSRI antidepressants, usually in combination with cognitive-behavioral, emotion regulation, or interpersonal-based psychotherapies.
BINGE-EATING DISORDER
Binge-eating disorder is distinguished from bulimia nervosa by the absence of compensatory behaviors to prevent weight gain after an episode and by a lack of effort to restrict weight gain between episodes. Other features are similar, including distress over the behavior and the experience of loss of control, resulting in eating more rapidly or in greater amounts than intended or eating when not hungry. The 12-month prevalence in females is 1.6%, with a much lower female-to-male ratio than bulimia nervosa. Little is known about the course of the disorder, given its recent categorization, but its prognosis is markedly better than for other eating disorders, both in terms of its natural course and response to treatment. Transition to other eating disorder conditions is thought to be rare.
PERSONALITY DISORDERS
CLINICAL MANIFESTATIONS
Personality disorders are characteristic patterns of thinking, feeling, and interpersonal behavior that are relatively inflexible and cause significant functional impairment or subjective distress for the individual. The observed behaviors are not secondary to another mental disorder, nor are they precipitated by substance abuse or a general medical condition. This distinction is often difficult to make in clinical practice, because personality change may be the first sign of serious neurologic, endocrine, or other medical illness. Patients with frontal lobe tumors, for example, can present with changes in motivation and personality while the results of the neurologic examination remain within normal limits. Individuals with personality disorders are often regarded as “difficult patients” in clinical medical practice because they are seen as excessively demanding and/or unwilling to follow recommended treatment plans. Although DSM-5 portrays personality disorders as qualitatively distinct categories, there is an alternative perspective that personality characteristics vary as a continuum between normal functioning and formal mental disorder.
Personality disorders have been grouped into three overlapping clusters. Cluster A includes paranoid, schizoid, and schizotypal personality disorders. It includes individuals who are odd and eccentric and who maintain an emotional distance from others. Individuals have a restricted emotional range and remain socially isolated. Patients with schizotypal personality disorder frequently have unusual perceptual experiences and express magical beliefs about the external world. The essential feature of paranoid personality disorder is a pervasive mistrust and suspiciousness of others to an extent that is unjustified by available evidence. Cluster B disorders include antisocial, borderline, histrionic, and narcissistic types and describe individuals whose behavior is impulsive, excessively emotional, and erratic. Cluster C incorporates avoidant, dependent, and obsessive-compulsive personality types; enduring traits are anxiety and fear. The boundaries between cluster types are to some extent artificial, and many patients who meet criteria for one personality disorder also meet criteria for aspects of another. The risk of a comorbid major mental disorder is increased in patients who qualify for a diagnosis of personality disorder.
SCHIZOPHRENIA
CLINICAL MANIFESTATIONS
Schizophrenia is a heterogeneous syndrome characterized by perturbations of language, perception, thinking, social activity, affect, and volition. There are no pathognomonic features. The syndrome commonly begins in late adolescence, has an insidious (and less commonly acute) onset, and, often, a poor outcome, progressing from social withdrawal and perceptual distortions to recurrent delusions and hallucinations. Patients may present with positive symptoms (such as conceptual disorganization, delusions, or hallucinations) or negative symptoms (loss of function, anhedonia, decreased emotional expression, impaired concentration, and diminished social engagement) and must have at least two of these for a 1-month period and continuous signs for at least 6 months to meet formal diagnostic criteria. Disorganized thinking or speech and grossly disorganized motor behavior, including catatonia, may also be present. As individuals age, positive psychotic symptoms tend to attenuate, and some measure of social and occupational function may be regained. “Negative” symptoms predominate in one-third of the schizophrenic population and are associated with a poor long-term outcome and a poor response to drug treatment. However, marked variability in the course and individual character of symptoms is typical.
The term schizophreniform disorder describes patients who meet the symptom requirements but not the duration requirements for schizophrenia, and schizoaffective disorder is used for those who manifest symptoms of schizophrenia and independent periods of mood disturbance. The terms “schizotypal” and “schizoid” refer to specific personality disorders and are discussed in that section. The diagnosis of delusional disorder is used for individuals who have delusions of various content for at least 1 month but who otherwise do not meet criteria for schizophrenia. Patients who experience a sudden onset of a brief (<1 month) alteration in thought processing, characterized by delusions, hallucinations, disorganized speech, or gross motor behavior, are most appropriately designated as having a brief psychotic disorder. Catatonia is recognized as a nonspecific syndrome that can occur as a consequence of other severe psychiatric/medical disorders and is diagnosed by the documentation of three or more of a cluster of motor and behavioral symptoms, including stupor, cataplexy, mutism, waxy flexibility, and stereotypy, among others. Prognosis depends not on symptom severity but on the response to antipsychotic medication. A permanent remission without recurrence does occasionally occur. About 10% of schizophrenic patients commit suicide.
Schizophrenia is present in 0.85% of individuals worldwide, with a lifetime prevalence of ~1–1.5%. An estimated 300,000 episodes of acute schizophrenia occur annually in the United States, resulting in direct and indirect costs of $62.7 billion.
DIFFERENTIAL DIAGNOSIS
The diagnosis is principally one of exclusion, requiring the absence of significant associated mood symptoms, any relevant medical condition, and substance abuse. Drug reactions that cause hallucinations, paranoia, confusion, or bizarre behavior may be dose-related or idiosyncratic; parkinsonian medications, clonidine, quinacrine, and procaine derivatives are the most common prescription medications associated with these symptoms. Drug causes should be ruled out in any case of newly emergent psychosis. The general neurologic examination in patients with schizophrenia is usually normal, but motor rigidity, tremor, and dyskinesias are noted in one-quarter of untreated patients.
EPIDEMIOLOGY AND PATHOPHYSIOLOGY
Epidemiologic surveys identify several risk factors for schizophrenia, including genetic susceptibility, early developmental insults, winter birth, and increasing parental age. Genetic factors are involved in at least a subset of individuals who develop schizophrenia. Schizophrenia is observed in ~6.6% of all first-degree relatives of an affected proband. If both parents are affected, the risk for offspring is 40%. The concordance rate for monozygotic twins is 50%, compared to 10% for dizygotic twins. Schizophrenia-prone families are also at risk for other psychiatric disorders, including schizoaffective disorder and schizotypal and schizoid personality disorders, the latter terms designating individuals who show a lifetime pattern of social and interpersonal deficits characterized by an inability to form close interpersonal relationships, eccentric behavior, and mild perceptual distortions.
TREATMENT | SCHIZOPHRENIA |
Antipsychotic agents (Table 466-10) are the cornerstone of acute and maintenance treatment of schizophrenia and are effective in the treatment of hallucinations, delusions, and thought disorders, regardless of etiology. The mechanism of action involves, at least in part, binding to dopamine D2/D3 receptors in the ventral striatum; the clinical potencies of traditional antipsychotic drugs parallel their affinities for the D2 receptor, and even the newer “atypical” agents exert some degree of D2 receptor blockade. All neuroleptics induce expression of the immediate-early gene c-fos in the nucleus accumbens, a dopaminergic site connecting prefrontal and limbic cortices. The clinical efficacy of newer atypical neuroleptics, however, may involve N-methyl-D-aspartate (NMDA) receptor blockade, α1– and α2-noradrenergic activity, altering the relationship between 5-HT2 and D2 receptor activity, and faster dissociation of D2 binding and effects on neuroplasticity.
ANTIPSYCHOTIC AGENTS |
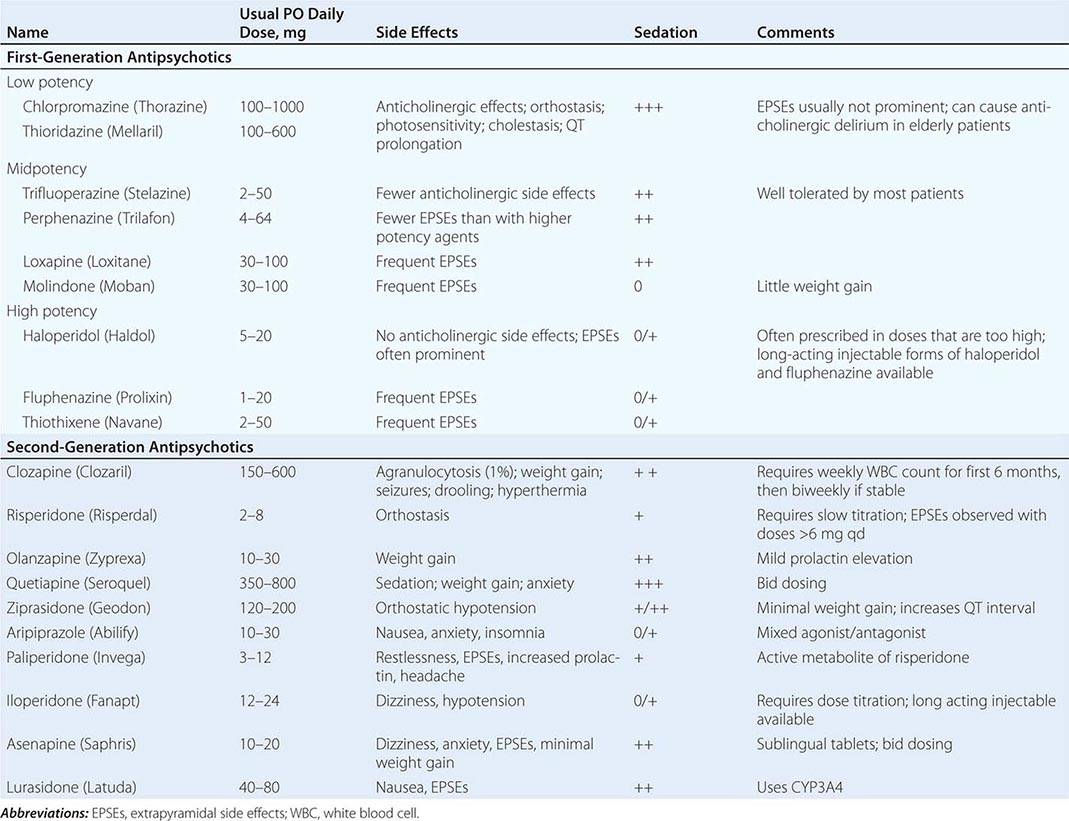
Conventional neuroleptics differ in their potency and side effect profile. Older agents, such as chlorpromazine and thioridazine, are more sedating and anticholinergic and more likely to cause orthostatic hypotension, whereas higher potency antipsychotics, such as haloperidol, perphenazine, and thiothixene, are more likely to induce extrapyramidal side effects. The model “atypical” antipsychotic agent is clozapine, a dibenzodiazepine that has a greater potency in blocking the 5-HT2 than the D2 receptor and a much higher affinity for the D4 than the D2 receptor. Its principal disadvantage is a risk of blood dyscrasias. Paliperidone is a recently approved agent that is a metabolite of risperidone and shares many of its properties. Unlike other antipsychotics, clozapine does not cause a rise in prolactin level. Approximately 30% of patients who do not benefit from conventional antipsychotic agents will have a better response to this drug, which also has a demonstrated superiority to other antipsychotic agents in preventing suicide; however, its side effect profile makes it most appropriate for treatment-resistant cases. Risperidone, a benzisoxazole derivative, is more potent at 5-HT2 than D2 receptor sites, like clozapine, but it also exerts significant α2 antagonism, a property that may contribute to its perceived ability to improve mood and increase motor activity. Risperidone is not as effective as clozapine in treatment-resistant cases but does not carry a risk of blood dyscrasias. Olanzapine is similar neurochemically to clozapine but has a significant risk of inducing weight gain. Quetiapine is distinct in having a weak D2 effect but potent α1 and histamine blockade. Ziprasidone causes minimal weight gain and is unlikely to increase prolactin but may increase QT prolongation. Aripiprazole also has little risk of weight gain or prolactin increase but may increase anxiety, nausea, and insomnia as a result of its partial agonist properties. Asenapine is associated with minimal weight gain and anticholinergic effect but may have a higher than expected risk of extrapyramidal symptoms.
Antipsychotic agents are effective in 70% of patients presenting with a first episode. Improvement may be observed within hours or days, but full remission usually requires 6–8 weeks. The choice of agent depends principally on the side effect profile and cost of treatment or on a past personal or family history of a favorable response to the drug in question. Atypical agents appear to be more effective in treating negative symptoms and improving cognitive function. An equivalent treatment response can usually be achieved with relatively low doses of any drug selected (i.e., 4–6 mg/d of haloperidol, 10–15 mg of olanzapine, or 4–6 mg/d of risperidone). Doses in this range result in >80% D2 receptor blockade, and there is little evidence that higher doses increase either the rapidity or degree of response. Maintenance treatment requires careful attention to the possibility of relapse and monitoring for the development of a movement disorder. Intermittent drug treatment is less effective than regular dosing, but gradual dose reduction is likely to improve social functioning in many schizophrenic patients who have been maintained at high doses. If medications are completely discontinued, however, the relapse rate is 60% within 6 months. Long-acting injectable preparations (risperidone, paliperidone, olanzapine, aripiprazole) are considered when noncompliance with oral therapy leads to relapses but should not be considered interchangeable, because the agents differ in their indications, injection intervals and sites/volumes, and possible adverse reactions, among other factors. In treatment-resistant patients, a transition to clozapine usually results in rapid improvement, but a prolonged delay in response in some cases necessitates a 6- to 9-month trial for maximal benefit to occur.
Antipsychotic medications can cause a broad range of side effects, including lethargy, weight gain, postural hypotension, constipation, and dry mouth. Extrapyramidal symptoms such as dystonia, akathisia, and akinesia are also frequent with first-generation agents and may contribute to poor adherence if not specifically addressed. Anticholinergic and parkinsonian symptoms respond well to trihexyphenidyl, 2 mg bid, or benztropine mesylate, 1–2 mg bid. Akathisia may respond to beta blockers. In rare cases, more serious and occasionally life-threatening side effects may emerge, including hyperprolactinemia, ventricular arrhythmias, gastrointestinal obstruction, retinal pigmentation, obstructive jaundice, and neuroleptic malignant syndrome (characterized by hyperthermia, autonomic dysfunction, muscular rigidity, and elevated creatine phosphokinase levels). The most serious adverse effects of clozapine are agranulocytosis, which has an incidence of 1%, and induction of seizures, which has an incidence of 10%. Weekly white blood cell counts are required, particularly during the first 3 months of treatment.
The risk of type 2 diabetes mellitus appears to be increased in schizophrenia, and second-generation agents as a group produce greater adverse effects on glucose regulation, independent of effects on obesity, than traditional agents. Clozapine, olanzapine, and quetiapine seem more likely to cause hyperglycemia, weight gain, and hypertriglyceridemia than other atypical antipsychotic drugs. Close monitoring of plasma glucose and lipid levels are indicated with the use of these agents.
A serious side effect of long-term use of first-generation antipsychotic agents is tardive dyskinesia, characterized by repetitive, involuntary, and potentially irreversible movements of the tongue and lips (bucco-linguo-masticatory triad) and, in approximately half of cases, choreoathetosis. Tardive dyskinesia has an incidence of 2–4% per year of exposure and a prevalence of 20% in chronically treated patients. The prevalence increases with age, total dose, and duration of drug administration. The risk associated with second-generation agents appears to be much lower. The cause may involve formation of free radicals and perhaps mitochondrial energy failure. Vitamin E may reduce abnormal involuntary movements if given early in the syndrome.
The CATIE study, a large-scale investigation of the effectiveness of antipsychotic agents in “real-world” patients, revealed a high rate of discontinuation of treatment over 18 months. Olanzapine showed greater effectiveness than quetiapine, risperidone, perphenazine, or ziprasidone but also a higher discontinuation rate due to weight gain and metabolic effects. Surprisingly, perphenazine, a first-generation agent, showed little evidence of inferiority to newer drugs.
Drug treatment of schizophrenia is by itself insufficient. Educational efforts directed toward families and relevant community resources have proved to be necessary to maintain stability and optimize outcome. A treatment model involving a multidisciplinary case-management team that seeks out and closely follows the patient in the community has proved particularly effective.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


