Courtesy of Sally Ezra/CDC.
“It’s the perfect setup. Then you put air travel in and it could be around the world overnight.”
—Michael T. Osterholm1 stated in his growing concerns over influenza pandemic preparedness in the United States (September 29, 2005).
What are the odds that an epidemic could kill a million people in the United States? What kind of viral outbreaks will we see in the future? Will there continue to be emerging and reemerging viruses? Emerging viruses can be defined as new or recently identified viruses that are affecting human health. The majority of new viruses affecting humans are of zoonotic origin. In other words, the new viral infections are caused by viruses that crossed the species barrier from animals to people. Reemerging viruses are viruses once thought to be under control from a public health perspective but that are making a “comeback,” or reappearing and causing increased incidence or geographic range of infections in human populations. In developed countries, public health measures such as sanitation, sewage treatment, vaccination programs, and access to good medical care have virtually eliminated “traditional” viral diseases such as smallpox, yellow fever, measles, and poliomyelitis. However, since 2014, a number of viral outbreaks have resulted in epidemics that have caught the media’s attention in both developed and developing countries:
In 2015, Zika virus infections transmitted by Aedes aegypti and Aedes albopictus mosquitoes were associated with microcephaly in newborns in Brazil. The World Health Organization (WHO) declared the epidemic a public health emergency of international concern on February 1, 2016. Zika virus infections continues to spread to new areas.
In 2015, a measles outbreak that started at Disneyland, California, triggered a national debate on vaccinations.
In 2015, a small town in Scott County, Indiana, struggled with a human immunodeficiency virus (HIV) epidemic associated with injection drug abuse of a prescription pain-relieving drug.
In 2014, Guinea, West Africa, was the epicenter of the worst Ebola epidemic in human history.
In 2014, a multistate avian influenza A (H5N2) epidemic affected turkey and chicken farms located in 15 U.S. states that threatened the poultry and egg industries. Some of the hardest hit states were Minnesota (the leading turkey producer), Iowa (the leading egg producer), and Wisconsin. Egg prices soared 30–60% during April 2015. More than 49 million birds died or were euthanized to contain the epidemic. The price of a dozen Grade A eggs rose to $1.66. The price of liquid, or “beater,” eggs that are used by the food industry to make products ranging from pasta to the Egg McMuffins sold at McDonald’s restaurants to ice cream increased by 63 cents from April to June 2014.
In 2014, the United States saw a nationwide outbreak of enterovirus D68, which caused a polio-like illness in clusters of children. Some children were permanently paralyzed as a result of the infection.
From January 21 to 31, 2014, one of the worst cruise ship norovirus outbreaks occurred on board the Royal Caribbean’s Explorer of the Seas cruise ship. The Centers for Disease Control and Prevention (CDC) reported that 634 passengers (21%) and 55 crew members (5%) had become ill.
Chikungunya virus, transmitted by A. aegypti and A. albopictus mosquitoes to humans, spread to the Americas for the first time in December 2013 on islands of the Caribbean. Before 2013, Chikungunya infections only occurred in Africa, Asia, and islands in the Indian and Pacific Oceans. In January 2014, U.S. authorities reported cases among travelers returning from the Caribbean. In July 2014, the first acquired case of Chikungunya in a nontraveler was reported in Florida.
The emergence or reemergence of viral infections is influenced by changes in the viral pathogen, human host, or environment/ecological niche. The disease triangle model is used to predict infectious disease outbreaks based on these host-pathogen-environment interactions. Human behavior plays a key role in influencing the emergence of infectious diseases and their pattern of spread. Environmental disruptions impact the range of many viral diseases, especially those transmitted by insect vectors such as mosquitoes.
15.1 Viral Evolution and Adaptation
TABLE 15-1 lists emerging and reemerging viruses, the majority of which contain RNA genomes. Viruses evolve by rapidly ongoing processes. Some genes in viruses mutate rapidly, whereas others may mutate but the progeny viruses are not able to infect the host because the mutations are lethal. For example, a gene that codes for a viral polymerase (pol) has a very specific conformational shape that is an essential requirement of the polymerase’s function in the synthesis of the viral genome. A mutation in the pol gene is not tolerable, whereas a mutation in a gene that encodes a capsid protein might be tolerated and not prevent the synthesis of newly mutated infectious virions.
The RNA viruses possess high mutation rates due to the lack of proofreading capability of the viral RNA-dependent RNA polymerases used to transcribe or replicate the viral genomes. In general, in RNA viruses the rate of point mutations is one mutation per every 104 to 105 nucleotides. In contrast, the mutation rate of DNA viruses is one mutation per every 108 to 1011 nucleotides. The mutation rate of HIV is two mutations for every five genomes. The mutation rate for severe acute respiratory syndrome coronavirus (SARS-CoV) is estimated to be three mutations for every RNA genome in every round of replication. Point mutations in the viral genome may result in amino acid changes in the encoded protein products, affecting their function. Mutations in genes can result in drug resistance (e.g., changes in the viral reverse transcriptase or polymerases or proteases) or changes that prevent host antibodies from binding to the surface proteins of the virus, thereby evading the host’s immune system (e.g., antigenic drift occurs in influenza A viruses, resulting in the circulation of different viral strains every flu season).
Two other mechanisms of genetic variation play a role in the evolution of viruses: recombination and reassortment. Recombination occurs when two viruses infect the same host cell and a new chimeric, or hybrid, genome is formed by a process of intermolecular exchange of the viral genomes (FIGURE 15-1A). Recombination occurs in viruses with either segmented or nonsegmented genomes. The complete genome of nonsegmented viruses consists of one piece or fragment of nucleic acid. In contrast, in segmented viruses the complete genome consists of several nucleic acid parts or fragments.
A model for the recombination of RNA virus genomes is based on the premise that hybrid RNAs are formed when the viral RNA–dependent RNA polymerase complex switches, midreplication, from one RNA molecule to another. Examples of RNA viruses with high recombination rates include SARS-CoV, Eastern equine encephalitis virus, and Western equine encephalitis virus. Recombination can significantly contribute to the establishment of new virus families. Viruses can steal genes from their hosts through a recombination process with the host chromosome. The cellular genes may or may not be used. Retroviruses are notorious for pirating cellular genes.
Table 15-1 New or Reemerging Human Viruses 1989–2015
| Year | Location of Discovery* | Virus |
| 1989 | United States | Measles virus** |
| 1990 | Brazil, South America | Sabia virus |
| 1993 | United States Four Corners Region | Sin Nombre virus |
| 1994 | Hendra, Australia | Hendra virus |
| 1995 | United States*** | Kaposi’s sarcoma associated herpesvirus (KSHV or human herpesvirus type-8, HHV-8) |
| 1996 | Uganda | O’nyong’nyong fever virus** |
| 1997 | Hong Kong | Avian influenza A (H5N1)** |
| 1999 | New York City | West Nile virus** |
| 1999 | Malaysia and Singapore | Nipah virus |
| 2001 | The Netherlands | Human metapneumovirus (hMPV) |
| 2002 | Guangdong Province, China* | SARS coronavirus (SARS-CoV) |
| 2003 | Multistate outbreak in the United States | Monkeypox virus** |
| 2005 | Europe | Bocavirus |
| 2005 | Amish community in Minnesota | Poliovirus** |
| 2006 | Midwestern United States | Mumps virus** |
| 2006 | La Reunion Island, France | Chikungunya virus |
| 2007 | United States | Adenovirus 14 variant |
| 2007 | Yap Islands, Micronesia | Zika virus |
| 2008 | Africa | Lujo virus |
| 2009 | Worldwide (pandemic) | Swine influenza A virus (H1N1)** |
| 2011 | Europe, United Kingdom | Schmallenburg virus |
| 2012 | Saudi Arabia | MERS coronavirus (MERS-CoV) |
| 2012 | Australia | Norovirus GII.4, Sydney strain |
| 2012 | California, Yosemite National Park | Hantavirus** |
| 2012 | Missouri, United States | Heartland virus |
| 2013 | Caribbean | Chikungunya virus** |
| 2013 | Utah, United States | West Nile virus (bald eagle-dieoff) |
| 2014 | United States | Enterovirus D68** |
| 2014 | United States, Disneyland | Measles virus** |
| 2014 | Kansas, United States | Bourbon virus |
| 2014 | United States | Avian influenza A virus (H5N2) on poultry farms |
| 2014 | South Korea | MERS-CoV |
| 2014 | West Africa | Ebola virus** |
| 2015 | Chicago, Illinois, area | Dog influenza A virus (H3N8) |
| 2015 | Treasure Valley, southwestern Idaho and eastern Oregon | Iris yellow spot virus in commercial onion fields |
| 2015 | Brazil, South America | Zika virus |
* If epidemic spread to multiple locations, sometimes only the epicenter is listed. **Reemerging viruses are indicated with two asterisks. All other viruses listed are new or emerging. ***HHV-8 was discovered in 1995 but was present earlier in people living with HIV. See Moore, P. S., et al. 1995 (Resources: Primary Literature). | ||

FIGURE 15-1 (a) Two coronaviruses coinfect the same host cell in which the nonsegmented +ssRNA viral genomes undergo recombination, resulting in the genome of a new viral strain. (b) Two different strains of influenza A viruses (H1N1 and H2N2, in this case) coinfect the same host animal or bird. Influenza A viruses contain segmented genomes consisting of eight –ssRNA fragments. The H or N gene segments are swapped to form a new influenza A virus strain.
Gene swapping, or reassortment, occurs when viruses that contain segmented genomes coinfect the same cell (FIGURE 15-1B). Influenza A viruses are notorious for this type of genetic adaptation. The genome of influenza A virus consists of eight segments of single-stranded RNA of negative polarity (–ssRNA). When the virus surface glycoprotein genes coding for hemagglutinin (H) or neuraminidase (n) undergo reassortment, a new viral strain is formed. Progeny viruses contain a genome that has genes from two or more parent viruses. When gene swapping occurs, it is referred to as antigenic shift. Antigenic shift is associated with pandemic strains of influenza A virus.
15.2 Human Factors Contributing to New and Reemerging Viral Infections
The genetic adaptation of viruses does not appear to be the major driving force that causes viral emergence. Human demographics drive viral disease emergence more than virus evolution or ecological factors. Human demographics are physical population characteristics. Demographics include characteristics such as the following:
Sex/gender
Race/ethnicity
Age
Mobility/travel
Occupation
Sexual behavior
Socioeconomic status (the economic, social, and physical environments in which individuals live and work)
Geographic location
Family size
Population Growth: Density and Crowding
A virus emerges when it reaches a new host population and then disseminates to different locations. The dramatic increase in the human population on Earth is correlated with higher human densities in given areas. The global human population growth curve is shown in FIGURE 15-2A. Increases in human populations lead to urbanization, the migration of people from the countryside to cities and suburbs. It is often associated with jobs in new industries and technology. As of 2010, the world had 26 megacities, each of which had a population of at least 10 million inhabitants. FIGURE 15-2B shows the global distribution of the human population in 2010. China, India, and other parts of Asia and Africa are the most populated areas. The largest megacity is the greater Tokyo-Yokohama area, which has a population of 37.8 million. As of 2015, the nine largest megacities after Tokyo are (in decreasing order of population):

FIGURE 15-2 (a) Estimated human population growth since the Neolithic Age. World human population from 8000 BC to AD 2005. Global population is rising at an exponential rate. (b) Distribution of the worldwide human population in 2015.
Jakarta, Indonesia: 30,500,000
Delhi, India: 24,900,000
Manila, Philippines: 24,100,000
Seoul-Incheon, South Korea: 23,480,000
Shanghai, China: 23,410,000
Karachi, Pakistan: 22,100,000
Beijing, China: 21,000,000
New York City, United States: 20,600,000
Guangzhou-Foshan, China: 20,500,000
Higher population densities favor the spread of viral diseases; for example, dense populations result in the combined problems of:
Crowding
Improper sanitation
Inadequate drinking water
Pollution
Overwhelmed healthcare facilities
When sanitary conditions are poor, people are more susceptible to respiratory and gastrointestinal infections.
Human Movement (Travel and Migration): Viruses Live in a World Without Borders
Humans are constantly on the move either for planned migration (e.g., for leisure, work, or commerce) or unplanned migration (e.g., because of war or civil unrest or natural disasters). Commercial air travel allows infected travelers to reach any part of the world in less than 24 hours, possibly starting a global pandemic. The spread of viral diseases to new areas can happen at any time. Viruses present in rural populations in Africa or Asia may show up in a developed part of the world, such as Europe or the United States. The severe acute respiratory syndrome (SARS) pandemic of 2002–2003 demonstrated the rapid spread of a viral disease by international air travel (FIGURE 15-3). Within a month, almost 20 countries had reported cases of SARS.
It is difficult to predict when the next influenza A pandemic will occur. However, avian influenza A (H5N1) virus has raised concerns about a potential human pandemic for several reasons:
It is highly virulent.
It is spread by migratory birds.
It can be transmitted from birds to mammals (e.g., from birds to domestic cats) and, in limited circumstances, to humans.
It continues to evolve due to antigenic shift and drift.
Since 2003, 15 countries have reported human cases of avian influenza A (H5N1) to the WHO (TABLE 15-2 and FIGURE 15-4). Avian influenza A (H5N1) occurs naturally among wild waterfowl, which usually do not get sick from it. Avian influenza A (H5N1) virus is shed in bird feces, saliva, and nasal secretions. Avian influenza A (H5N1) is highly contagious and nearly 100% fatal in domesticated birds such as chickens, turkeys, and ducks, often within 48 hours. People in direct contact with sick birds or surfaces contaminated with secretions and/or excretions from infected birds on farms or live animal markets are most susceptible to infection by the virus. At the time of this writing, the virus does not efficiently spread from person to person. Approximately 53% of people infected with the influenza A (H5N1) strain died. To date, the risk of avian influenza A (H5N1) virus infection to travelers is very low.

FIGURE 15-3 Spread of SARS-CoV from the Metropole Hotel in Hong Kong as of March 28, 2003. Patient zero of the SARS pandemic stayed at the Metropole Hotel.
The U.S. Geological Survey’s National Wildlife Health Center located in Madison, Wisconsin, monitors samples colected from migratory waterfowl for avian influenza A viruses. They speculate that influenza virus A (H5N1) will enter North America through migratory birds in the Pacific flyway, which follows the eastern Pacific coastline from the western Arctic, including Alaska and the Aleutian Islands, down the Rocky Mountain and Pacific coastal regions of Canada, the United States, and Mexico, to where it blends with other flyways in Central and South America. If avian influenza A virus (H5N1) is detected among migratory birds, the monitoring can provide an early warning to agricultural communities, public health officials, and experts of wildlife agencies. Highly pathogenic avian influenza A viruses can also enter North America through other routes, such as through illegal importation of infected domestic birds or by an infected traveler.
Cruise vacations are an increasingly popular leisure activity. From 1993 to 1998, the number of cruise ship passengers in the United States increased by 50%. In North America alone, about 6.8 million passengers board cruise ships each year. In recent years, there has been an increase in gastrointestinal illness caused by norovirus on cruise ships, which in essence are floating mini-cities with a constantly changing population of hundreds of thousands of people in a confined space. Between 2001 and 2004, the number of norovirus outbreaks on cruise ships increased 10-fold. In 2002, a new norovirus variant emerged in hospitals in the United Kingdom and Ireland and on U.S. cruise ships, and two new variants emerged in 2006 in the Netherlands. In March 2012, a new norovirus strain, Genogroup 2, Genotype 4 II, originating in Sydney, Australia, became the leading cause of norovirus outbreaks in Australia, the United States, and the United Kingdom. The norovirus name is abbreviated GII.4, Sydney noro-virus. GII.4 Sydney norovirus is the predominant cause of norovirus outbreaks today, replacing the GII.4 New Orleans strain. GII.4 noroviruses are associated with increased hospitalizations and deaths during outbreaks. Norovirus outbreaks are reported through the CDC’s CaliciNet Laboratories Outbreak Support Centers (http://www.cdc.gov/norovirus/reporting/calicinet/participants.html).

Table 15-2 Cumulative Number of Confirmed Human Cases of Avian Influenza A (H5N1), 2003–2015
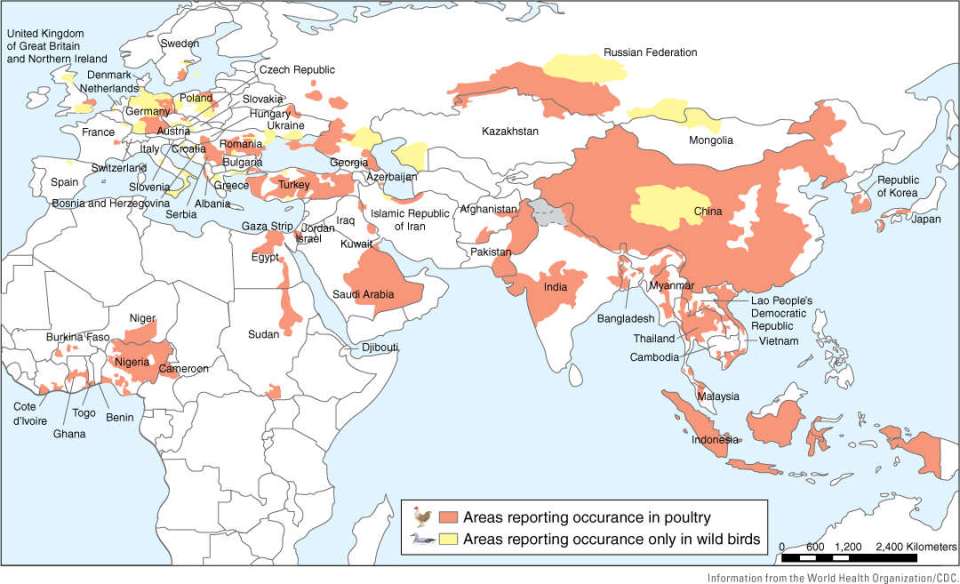
FIGURE 15-4 Nations with confirmed cases of avian influenza A (H5N1) virus in poultry and wild birds as of April 12, 2007.
Noroviruses cannot be cultured in the laboratory, and there is no animal model available to study them, making it difficult to determine what genetic changes in a norovirus trigger outbreaks or cause more severe symptoms. The CDC started the Vessel Sanitation Program (VSP) in the early 1970s as a result of several disease outbreaks on cruise ships. The mission of the VSP was to protect the health of passengers and crew by minimizing the risk of gastrointestinal illness on cruise ships. Routine inspections are now performed on the following in cruise ships:
Water supply (storage, distribution, protection, and disinfection)
Spas and pools (filtration and disinfection)
Food (protection during storage, preparation, and service)
Employee hygiene practices
General cleanliness and physical condition of the ship (absence of insects and rodents)
Training programs (environmental and public health practices)
Inspections scores are posted on the CDC’s VSP web-site (http://www.cdc.gov/nceh/vsp/).
War, famine, and natural disasters have played a large part in introducing infectious diseases into humans. Refugee camps and temporary shelters are often characterized by crowded living conditions, poor sanitation, a lack of access to clean water, and populations with poor nutritional status and limited access to medical care. Under these conditions, people are highly susceptible to infectious agents; for example, in 2005 Hurricane Katrina evacuees in the New Orleans Superdome and the Houston Astrodome and Reliant Center experienced a norovirus outbreak. For some time, there were no working toilets and little clean water in those facilities (FIGURE 15-5).

FIGURE 15-5 (a) Hurricane Katrina hit the U.S. Gulf Coast on August 29, 2005. This aerial photograph of New Orleans, Louisiana, was taken on September 5, 2005. The homes and streets remained flooded for 7 days after Hurricane Katrina hit the city. Much of the city was underwater and without electricity. (b) Many injured individuals were rescued from their flooded homes and evacuated following Hurricane Katrina in 2005. The photograph shows families evacuated to the Astrodome in Houston, Texas. Conditions in the large rescue centers quickly became overcrowded and unsanitary.
Aircraft are a potential means of unintentionally moving virus-infected animals or arthropod vectors such as mosquitoes from country to country and continent to continent. Researchers demonstrated that mosquitoes, houseflies, and flour beetles can survive in the wheel bays of commercial Boeing 747 airplanes. The insects were able to withstand the extreme temperatures of one-way and round-trip flights. The leading theory is that the 1999 West Nile virus (WNV) outbreak in New York was attributed to airplanes carrying WNV– infected Culex pipiens mosquitoes when they flew across the Atlantic Ocean from Israel. At the time, aircraft cabin spaces were not routinely sprayed with insecticides on intercontinental flights entering the United States.
Prior to 1999, West Nile encephalitis had never been reported in the Western hemisphere and no one had considered that it could be introduced. The outbreak was originally thought to be caused by St. Louis encephalitis virus, an endemic disease transmitted by mosquitoes in the United States. A correct diagnosis was made after a veterinarian at the Bronx Zoo correlated the death of native birds with human cases of encephalitis. (St. Louis encephalitis virus commonly infects birds but does not cause disease outbreaks.) WNV quickly spread across the contiguous states of the United States and into Canada, the Caribbean, and Mexico (FIGURES 15-6A and 15-6B). The main reservoir of WNV is birds. Mosquitoes pick up WNV while taking a blood meal from infected birds. From there, WNV moves to horses and humans through a mosquito bite. Humans and horses are “dead-end hosts” that cannot transmit WNV to other species (FIGURE 15-6C). Between 1999 and 2010, 30,702 human cases of encephalitis and 1,220 (4%) human deaths from encephalitis were reported in the United States. Between 1999 and 2010, 25,889 cases of equine encephalitis were reported. By 2004, 15,000 horses had died of West Nile encephalitis.
Investigation of a new reservoir of WNV began in 2007. Stable flies were suspected of being involved in the WNV deaths of hundreds of pelican chicks at the Medicine Lake National Wildlife Refuge in northeast Montana. Montana State University entomologist Greg Johnson observed stable flies feeding on the blood of sick and dying pelicans. Stable flies look like house flies, but they have a painful bite. Johnson captured 1,300 stable flies and divided them into 60 groups. Eighteen of those groups tested positive for WNV. This was the first evidence to suggest that stable flies might transmit WNV at the pelican colony.
In 2002, four novel routes of West Nile virus transmission to humans were reported:
Blood transfusion
Organ transplantation
Transplacental transfer
Breastfeeding
In the United States, 23 people were reported to have acquired WNV infection after receiving blood transfusions and 500 donations were identified as being given by donors infected with WNV in 2002. Beginning in 2003, per the recommendation of the Food and Drug Administration (FDA), blood-collection agencies implemented nucleic acid amplification tests (NATs) to screen all blood donations for WNV in order to prevent transmission of WNV through contaminated blood products. All blood units that test positive for WNV are discarded appropriately.

FIGURE 15-6 (a) Map of human West Nile encephalitis cases and avian, animal, or mosquito infections in 1999 (the first year of the outbreak in the United States). (b) Map of human West Nile encephalitis cases and avian, animal, or mosquito infections in 2006. The West Nile virus spread quickly across the United States through its mosquito vectors. (c) West Nile virus transmission cycle. Infected birds can develop viremia (high levels of West Nile viruses in their bloodstream). Mosquitoes become infected when taking a blood meal while biting infected birds. After a week, mosquitoes infected with West Nile virus bite and infect horses, people, and other mammals that are dead-end hosts for West Nile virus. Dead-end hosts do not develop viremia in their bloodstream and therefore cannot pass the West Nile virus on to other biting mosquitoes.
At the time of this writing, Zika virus is an emerging viral threat that is the focus of an ongoing pandemic and public health emergency. Zika virus is transmitted by day-biting Aedes spp. mosquitoes. Before 2007, Zika virus infections were limited to sporadic or small clusters of patients in Africa and Asia. The first major outbreak of Zika virus infections occurred in Yap (Federated States of Micronesia) in which 78% of the population was infected and 18% of infected individuals developed symptoms. Since then, Zika virus infection spread rapidly. Outbreaks have occurred in French Polynesia, Cook Islands, Easter Island, New Caldonia, and most recently, South America. Zika virus was first reported in May 2015, in Brazil where 440,000–1,300,000 people were subsequently infected by February 2016. Furthermore, cases originating in 29 additional countries in the Americas were reported. The ease of air travel and international trade caused further spread into regions where Zika virus is not endemic (VIRUS FILE 15-1).