Mycobacterium tuberculosis Lymphadenitis
Tariq Muzzafar, MBBS
Key Facts
Clinical Issues
High index of suspicion essential for diagnosis
Definitive diagnosis by histology and culture of LN
Molecular methods enable quicker identification of organism
FNA is as useful as excisional LN biopsy in HIV(+) patients
Microscopic Pathology
Granulomas, classically with necrotic center (caseation)
Concentric layers of epithelioid cells, Langhans giant cells, lymphocytes, and plasma cells
Fibrosis, hyalinization, calcification present in healing phase
In LN biopsy specimen, AFB identified morphologically by
Ziehl-Neelsen, Kinyoun, Fite-Faraco stains
It is common for stains to be negative in culture (+) cases
Auramine-rhodamine stain with fluorescent microscopy more sensitive for detection
Top Differential Diagnoses
M. avium-intracellulare lymphadenitis
Histoplasma lymphadenitis
Kikuchi-Fujimoto lymphadenitis
Cat scratch lymphadenitis
Sarcoidosis lymphadenopathy
Reporting Considerations
Suspected or confirmed cases of TB should be reported to local public health department
Identify contacts for follow-up
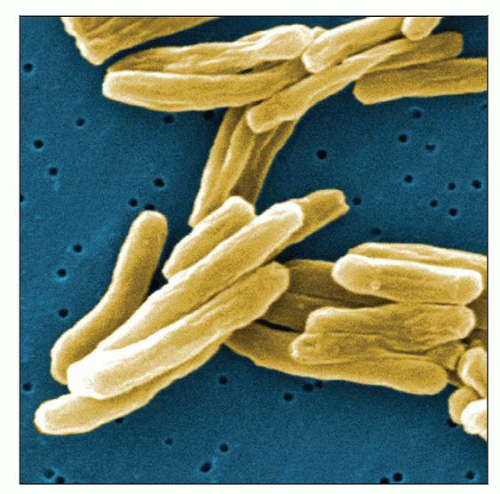 Scanning electron micrograph of M. tuberculosis. The bacterium ranges from 2-4 µm long and 0.2-0.5 µm wide. (Courtesy J. Carr, CDC Public Health Image Library, #9997.) |
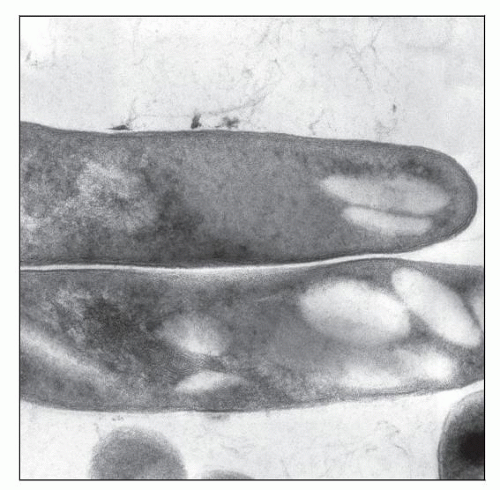 Thin section transmission electron micrograph demonstrates M. tuberculosis bacilli. (CDC Public Health Image Library, #8433.) |
TERMINOLOGY
Abbreviations
Acid-fast bacilli (AFB)
Tuberculosis (TB)
Definitions
Lymphadenitis caused by infection with Mycobacterium tuberculosis
ETIOLOGY/PATHOGENESIS
Infectious Agents
Mycobacterium tuberculosis
Immunocompetent Patients
Reactivation of disease at site seeded during primary infection by hematogenous route
Infection of tonsils, adenoids, and Waldeyer ring
Abdominal involvement may occur via ingestion of milk or sputum infected with M. tuberculosis
Immunocompromised Patients
Human immunodeficiency virus (HIV) infection most common
Reactivation of latent infection
Part of generalized infection, miliary dissemination
Greater mycobacterial load than immunocompetent patients
CLINICAL ISSUES
Epidemiology
Incidence
˜ 40% of peripheral lymphadenopathy in developing world
Prevalence of TB lymphadenitis in children ≤ 14 years in rural India: 4.4/1,000
Lymphadenitis is most common form of extrapulmonary tuberculosis (5-10% of cases)
In developed countries, most cases occur in immigrants and travelers to endemic areas
Immigrant populations mostly originate from Southeast Asia and Africa
In USA, 20% of TB cases are extrapulmonary
˜ 30% of these cases present with lymphadenitis
M. tuberculosis is common in HIV-positive individuals
Part of pulmonary or disseminated disease
Most extrapulmonary TB cases occur with CD4 counts ≤ 100 cells/µL
Age
Historically, common in children
At present, children affected predominantly in developing countries
Peak age in developed countries: 20-40 years
Gender
M:F ratio = 1:2
Ethnicity
Asian Pacific Islanders more susceptible
Presentation
Characteristically, multiple lymph nodes (LNs) involved
90% involve superficial LNs in head and neck region
Anterior and posterior cervical (most common)
Supraclavicular, submandibular, preauricular, submental also involved
Other LNs: Axillary, inguinal, mesenteric, mediastinal, and intramammary
Isolated intraabdominal LNs can be involved
Periportal, peripancreatic, and mesenteric
Generalized lymphadenopathy and hepatosplenomegaly in 5%
Painless progressive swelling in neck
Parabronchial and paratracheal involvement can lead to airway compromise
5% of children develop lymphadenopathy within 6 months of infection
In adults, TB represents reactivation of previous infection
Up to 1/3 of patients report previous or family history of TB
LN on physical examination
Firm, rubbery, discrete, and nontender
May be swollen and tender due to secondary bacterial infection
Ulcer &/or sinus tract formation in 10%
Laboratory Tests
Tuberculin skin test (TST)
Positive in 90% of cases with TB lymphadenopathy
May be negative in HIV-positive patients with TB
Interferon-γ release assays
Measure in vitro T-cell interferon-γ release in response to 2 unique antigens
Sensitivity in active TB: 75-90%
Highly specific for M. tuberculosis
Negative in prior BCG vaccination and in sensitization to nontuberculous mycobacteria
Cannot distinguish between latent and active tuberculosis
2 widely studied tests
Enzyme-linked immunospot (ELISpot) (T-SPOT.TB; Oxford Immunotec; Oxford, UK)
Enzyme-linked immunosorbent assay (ELISA) (QuantiFERON-TB Gold; Cellestis; Chadstone, VIC; Australia)
For diagnosis of latent infection
Sensitivity of ELISA similar to TST
ELISpot more sensitive
Direct staining
Carbolfuchsin stains (Ziehl-Neelsen stain; Kinyoun stain) highlight AFB
AFB are bright red against blue or green background, depending on counterstain
Must be scanned under oil-immersion
Time consuming due to limited size of field viewed at 1 time
Fluorochrome stain (auramine O, with or without rhodamine)
Scanning quicker since slides can be scanned at 25x objective
Confirmation may require 40x objective
Bacteria bright yellow (auramine) or orange-red (rhodamine) against dark background
Microbiological culture
Loewenstein-Jensen (L) medium
Less sensitive
Recommended only for chromogenic studies and biochemical tests
Middlebrook 7H10 and 7H11 agar medium used for isolation and susceptibility testing
Automated Radiometric Detection Systems: BACTEC 460 (BD Diagnostic Systems; Sparks, MD; USA)
Automated Nonradiometric Detection Systems
MGIT 960 (BD Diagnostic Systems)
MB/BacT System (BioMerieux; Durham, NC; USA)
BACTEC MYCO/F lytic blood culture bottle (BD Diagnostic Systems)
ESP Culture System II (TREK Diagnostic Systems, Inc.; Cleveland, OH; USA)
Gas-liquid and high-performance liquid chromatography
Useful in culture confirmation
Molecular diagnosis
Uses
Culture confirmation of isolates
Identification of isolates
Direct detection
DNA fingerprinting
Strain-typing
Quicker identification than by traditional methods
2 amplification-based methods FDA approved in USA
Amplicor M. tuberculosis PCR assay (Roche Diagnostics; Indianapolis, IN; USA)
Amplified M. tuberculosis Direct Test (Gen-Probe Incorporated; San Diego, CA; USA)
Home-brew PCR, including real-time PCR assays, have been developed but need validation by individual laboratories
DNA sequencing can make rapid and accurate identification
Strain-typing has been used in detection of drug resistance
Treatment
Surgical approaches
Needed in minority of patients
Indications: Failure of antimicrobial chemotherapy, pressure effect
Excisional biopsy preferred since incisional biopsy may result in sinus tract formation
Drugs
All patients treated with antituberculous agents
Treatment may be started prior to culture confirmation
Particularly when pathologic features suspicious or in high-risk subject
Adults: 6 months of isoniazid, rifampin, pyrazinamide, and ethambutol
Children: 2 months of isoniazid, rifampin, and pyrazinamide, plus 2 months of isoniazid and rifampin
Mediastinal lymph node involvement treated with same regimen as lung involvement
Prognosis
Antimicrobial therapy curative; relapse rates of up to 3.5%
In 30% of patients after beginning therapy
Paradoxical increase in LN size
New enlarged LNs may develop
Mechanism is immune response to mycobacterial killing
Must be differentiated from relapse
HIV-positive patients who begin HAART may develop immune reconstitution inflammatory syndrome with worsening lymphadenopathy
Residual palpable LNs after completion of therapy may be present in 5-30% of patients
Retreatment generally considered to be unnecessary if
Cultures are negative
Compliance with treatment is documented
IMAGE FINDINGS
General Features
Not definitively diagnostic of TB lymphadenitis
Radiographic Findings
80% of children and 20% of adults show evidence of recent or active tuberculosis in lungs



