Chapter 40 Low back pain is the second leading reason, behind upper respiratory infection, for visits to primary care. The lifetime prevalence of at least one episode of back pain is 70% to 85%. It is not possible to determine the exact cause of the pain in about 80% of cases. The differential diagnosis is broad. Most low back pain appears to be due to muscular or ligamentous injuries that usually are self-limited. Acute low back pain may become chronic even if properly treated. Careful evaluation is necessary to rule out a serious cause. Simple acute back pain does not require imaging studies unless trauma has occurred. Box 40-1 summarizes the classification of back pain.
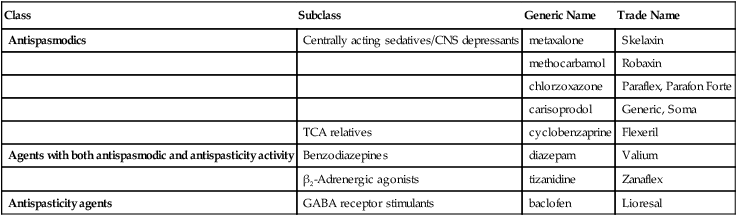
Muscle Relaxants
Class
Subclass
Generic Name
Trade Name
Antispasmodics
Centrally acting sedatives/CNS depressants
metaxalone
Skelaxin
methocarbamol
Robaxin
chlorzoxazone
Paraflex, Parafon Forte
carisoprodol
Generic, Soma
TCA relatives
cyclobenzaprine
Flexeril
Agents with both antispasmodic and antispasticity activity
Benzodiazepines
diazepam
Valium
β2-Adrenergic agonists
tizanidine
Zanaflex
Antispasticity agents
GABA receptor stimulants
baclofen
Lioresal
Therapeutic Overview
Pathophysiology
Disease Process
Low Back Pain
Mechanism of Action
Centrally Acting Sedatives/CNS Depressants
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


