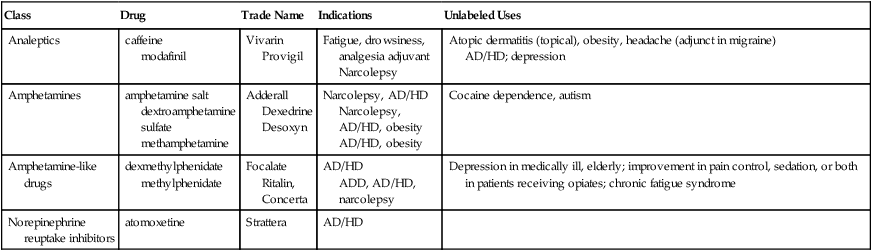
Chapter 41 INDICATIONS • Attention-deficit/hyperactivity disorder (AD/HD); see Table 41-1 TABLE 41-1 Selected AD/HD Drug Indications and Unlabeled Uses See Chapter 47 for antidepressants used for AD/HD. • Narcolepsy: dextroamphetamine, armodafinil, ephedrine, methylphenidate, modafinil, sodium oxybate • Obesity: benzphetamine, dexfenfluramine, diethylpropion, fenfluramine, methamphetamine, orlistat, phendimetrazine, phentermine, phenylpropanolamine Atomoxetine, which is indicated only for the treatment of AD/HD, increases extracellular concentrations of norepinephrine, although the precise mechanism for efficacy in AD/HD is unknown. Antidepressants are used occasionally in children who have failed to respond to other therapy. Modafinil, a CNS analeptic with a unique mechanism of action, is used to treat excessive sleepiness associated with narcolepsy, obstructive sleep apnea, and shift work sleep disorder in adults. It does not have FDA approval for use in AD/HD. Analeptics are not discussed here in detail. An analeptic is a drug that acts as a stimulant to the CNS. Caffeine is the most common analeptic seen in primary care. It is used on an OTC basis to help people stay awake and restore mental alertness and as an adjunct in analgesic formulations. It is a methylxanthine and is not discussed here in detail. An extended-release clonidine (Kapvay) was approved in late 2010 as adjunctive therapy to stimulants for AD/HD or as monotherapy. Chapter 16 provides a discussion of the theophyllines, which are related chemically to the methylxanthines. A variety of other drugs have been approved for use in AD/HD, including guanfacine, an oral, centrally acting, α2- adrenergic receptor agonist usually used in the treatment of hypertension. It is similar to clonidine, the extended form Kapvay, which has been approved for use in AD/HD. Some antidepressants may also be helpful in AD/HD, but they are not discussed in detail in this chapter (see Chapter 47). Antidepressants and α-agonists may cause adverse cardiac effects. • Subcommittee on Attention-Deficit/Hyperactivity Disorder. ADHD: clinical practice guidelines for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents, Pediatrics 128(5):1007-1022, 2011. Epub 2011 Oct 16. Available at http://pediatrics.aappublications.org/content/early/2011/10/14/peds.2011-2654.full.pdf+html. • Supplemental index to the above article: Implementing the Key Action Statements: an algorithm and explanation for the process of care for the evaluation, diagnosis, treatment, and monitoring of ADHD in children and adolescents. Available at http://pediatrics.aappublications.org/content/early/2011/10/14/peds.2011-2654/suppl/DC1.
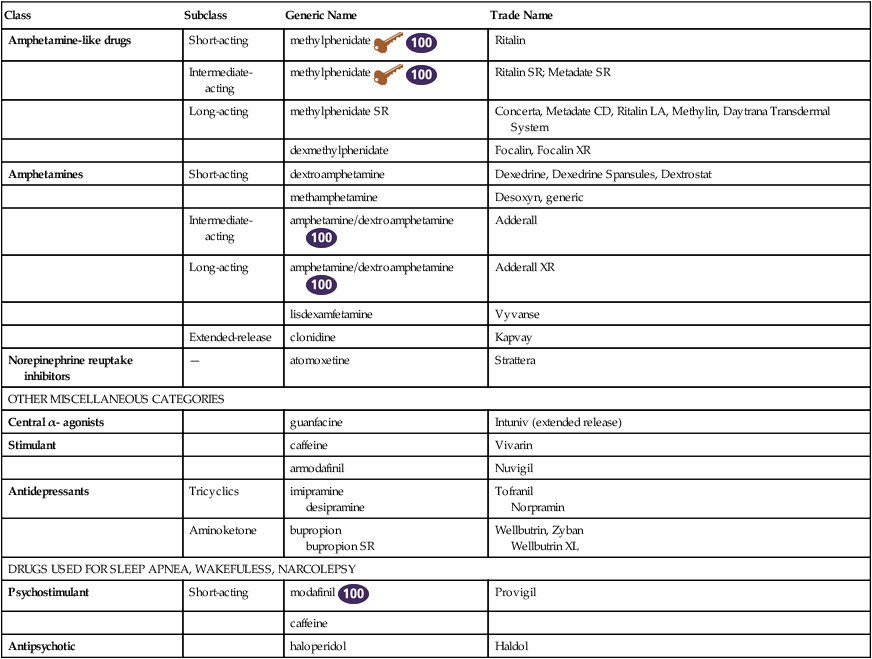
Medications for Attention-Deficit/Hyperactivity Disorder
Class
Subclass
Generic Name
Trade Name
Amphetamine-like drugs
Short-acting
methylphenidate 

Ritalin
Intermediate-acting
methylphenidate 

Ritalin SR; Metadate SR
Long-acting
methylphenidate SR
Concerta, Metadate CD, Ritalin LA, Methylin, Daytrana Transdermal System
dexmethylphenidate
Focalin, Focalin XR
Amphetamines
Short-acting
dextroamphetamine
Dexedrine, Dexedrine Spansules, Dextrostat
methamphetamine
Desoxyn, generic
Intermediate-acting
amphetamine/dextroamphetamine 
Adderall
Long-acting
amphetamine/dextroamphetamine 
Adderall XR
lisdexamfetamine
Vyvanse
Extended-release
clonidine
Kapvay
Norepinephrine reuptake inhibitors
—
atomoxetine
Strattera
OTHER MISCELLANEOUS CATEGORIES
Central α- agonists
guanfacine
Intuniv (extended release)
Stimulant
caffeine
Vivarin
armodafinil
Nuvigil
Antidepressants
Tricyclics
imipramine
desipramine
Tofranil
Norpramin
Aminoketone
bupropion
bupropion SR
Wellbutrin, Zyban
Wellbutrin XL
DRUGS USED FOR SLEEP APNEA, WAKEFULESS, NARCOLEPSY
Psychostimulant
Short-acting
modafinil 
Provigil
caffeine
Antipsychotic
haloperidol
Haldol
Class
Drug
Trade Name
Indications
Unlabeled Uses
Analeptics
caffeine
modafinil
Vivarin
Provigil
Fatigue, drowsiness, analgesia adjuvant
Narcolepsy
Atopic dermatitis (topical), obesity, headache (adjunct in migraine)
AD/HD; depression
Amphetamines
amphetamine salt
dextroamphetamine sulfate
methamphetamine
Adderall
Dexedrine
Desoxyn
Narcolepsy, AD/HD
Narcolepsy, AD/HD, obesity
AD/HD, obesity
Cocaine dependence, autism
Amphetamine-like drugs
dexmethylphenidate
methylphenidate
Focalate
Ritalin, Concerta
AD/HD
ADD, AD/HD, narcolepsy
Depression in medically ill, elderly; improvement in pain control, sedation, or both in patients receiving opiates; chronic fatigue syndrome
Norepinephrine reuptake inhibitors
atomoxetine
Strattera
AD/HD
Mechanism of Action
Amphetamine-like Drugs
α2- Adrenergic Receptor Agonists, Analeptics, Antidepressants, and Stimulants
Treatment Principles
Standardized Guidelines
![]()
Stay updated, free articles. Join our Telegram channel

 Top 100 drug;
Top 100 drug;  Key drug.
Key drug.
Full access? Get Clinical Tree


