Chapter 33 • The Agency for Healthcare Research and Quality (AHRQ) Guideline on Benign Prostate Hyperplasia: Diagnosis and Treatment was developed in 1994 and continues as the seminal resource in this area. Guideline on the management of benign prostatic hyperplasia (BPH). American Urological Association Education and Research 2010. • The AUA has developed an algorithm for evaluation and treatment of patients with BPH. • α-Blockers and 5α-reductase inhibitors are beneficial. • Surgery: Transurethral microwave thermotherapy and transurethral resection are beneficial. • Herbal treatments: β-Sitosterol plant extract and saw palmetto plant extracts are likely to be beneficial; Pygeum africanum and rye grass pollen extract have unknown effectiveness. • First line: α1A-Selective antagonist for patients without HTN; long-acting α1-antagonist for patients with HTN given to reduce symptoms • 5α-Reductase inhibitor given to shrink the size of the prostate; however, 6 months of therapy is required to achieve maximum benefit. • Combination therapy with α1-antagonist plus a 5α- reductase inhibitor See Table 33-1. The short-acting drugs have an increased incidence of adverse effects because of the rapid increase in drug levels. TABLE 33-1 Pharmacokinetics of Male Genitourinary Agents
Male Genitourinary Agents
Class
Subclass
Generic Name
Trade Name
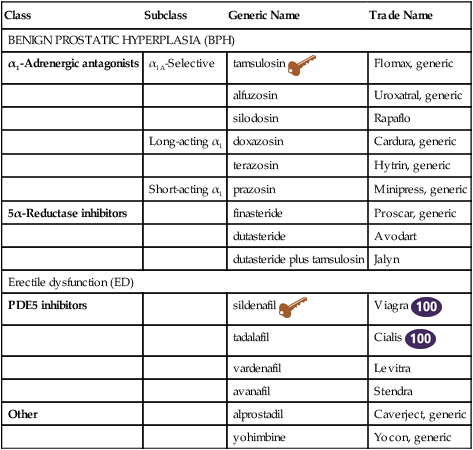
BENIGN PROSTATIC HYPERPLASIA (BPH)
α1-Adrenergic antagonists
α1A-Selective
tamsulosin 
Flomax, generic
alfuzosin
Uroxatral, generic
silodosin
Rapaflo
Long-acting α1
doxazosin
Cardura, generic
terazosin
Hytrin, generic
Short-acting α1
prazosin
Minipress, generic
5α-Reductase inhibitors
finasteride
Proscar, generic
dutasteride
Avodart
dutasteride plus tamsulosin
Jalyn
Erectile dysfunction (ED)
PDE5 inhibitors
sildenafil 
Viagra 
tadalafil
Cialis 
vardenafil
Levitra
avanafil
Stendra
Other
alprostadil
Caverject, generic
yohimbine
Yocon, generic
Treatment Principles
Standardized Guidelines
Evidence-Based Recommendations
Cardinal Points of Treatment
Specific Drugs
α1-Adrenergic Antagonists
 tamsulosin (Flomax)
tamsulosin (Flomax)
Drug
Absorption and Availability
Onset of Action
Peak Effect
Duration of Action
Protein Bound
Metabolism
Excretion
tamsulosin (Flomax)
90% available after first pass; decreased by food
4-8 hr
2-4 wk
24 hr
94%-99%
Hepatic CYP450 pathway not known
Urine, 76% metabolized; urine, 10% unchanged; feces, 21%
alfuzosin (Uroxatal)
49%; increased by food; take following meal
8 hr
4-6 wk
>24 hr
80%-90%
Extensive, some by CYP 3A4
69% feces; urine 24%-30%
Silodosin (Rapaflo)
32%
3 hr
97%
3A4
Feces 55%, urine 34%
doxazosin, extended release
62%-69%; not affected by food
2 wk
4-6 wk
>24 hr
98%
3A4, 2D6, 2C9
63% feces
terazosin
Completely absorbed, minimal effect from food
2 wk
4-6 wk
>24 hr
90%-94%
Liver, extensive
Feces, 55%-60%
finasteride (Proscar)
63% available after first pass
3 months
6 months
2 wk
90%
Hepatic
2D6
3A4
Urine, 40% as metabolites; feces, 60%
dutasteride (Avodart)
60%
3 months
6-12 months
5 wk
99%
3A4, 3A5
Feces, 45%
sildenafil (Viagra)
Rapid, 40% ↓ with high-fat meal
60 min
Peak 2 hr
4 hr
96%
CYP 3A42C9
Feces, 80%
tadalafil (Cialis)
Not affected by food
30-45 min
2 hr
36 hr
94%
CYP 3A4
Feces, 61%
vardenafil (Levitra)
15% bioavailable, ↓ with high-fat meal
60 min
2 hr
4 hr
95%
CYP 3A4
Feces, 91%
alprostadil pellets
Absorbed from urethra
30 min
30-60 min
1 hr
81%
—
Metabolized in lungs; 90% kidney as metabolites ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Male Genitourinary Agents

 Top 100 drug;
Top 100 drug;  Key drug. Key drug because it was the first on the market and is in common use. Drugs listed in general order of use within class.
Key drug. Key drug because it was the first on the market and is in common use. Drugs listed in general order of use within class. Finasteride and dutasteride are teratogenic. Tablets must not be touched by a woman who may be pregnant because the product may be absorbed through the skin. A pregnant woman should not come in contact with the semen of a man who is taking finasteride.
Finasteride and dutasteride are teratogenic. Tablets must not be touched by a woman who may be pregnant because the product may be absorbed through the skin. A pregnant woman should not come in contact with the semen of a man who is taking finasteride.