Diffuse growth pattern, not scattered cells of lymphomatoid granulomatosis (LYG)
Not angiocentric, usually no necrosis, and no mixed background infiltrate
• Vasculitis
Can show similar histologic features to LYG with inflammation of blood vessels and involvement of multiple organ systems
Usually not EBV(+), vasculitis has nonmonoclonal B cells
LYG at Low Power Low-power view of cutaneous lymphomatoid granulomatosis (LYG) shows an extensive B-cell infiltrate with a perivascular angiodestructive distribution . The epidermis is not involved. (Courtesy M. Royer, MD.)
LYG Involving Subcutis LYG diffusely infiltrating into the fat can mimic a reactive panniculitis. There is angiocentric involvement with tumor cells surrounding and infiltrating blood vessels .
Epstein-Barr Virus Encoded Receptor in LYG A higher power magnification of the same lesion shows that many of the Epstein-Barr virus (EBV)-encoded receptor (EBER)(+) cells are large in size and show some nuclear irregularity. The smaller reactive T cells are EBER(-).
*IGH* Gene Rearrangement in LYG PCR test for IGH gene rearrangements shows a dominant monoclonal peak at position 250 . IGH gene rearrangements are often detected in LYG since it is a B-cell lymphoma.
TERMINOLOGY
Abbreviations
• Lymphomatoid granulomatosis (LYG)
Synonyms
• Angiocentric immunoproliferative lesion
Definitions
• Extranodal Epstein-Barr virus (EBV)-driven mature B-cell lymphoma that is angiocentric
It is uncertain whether LYG represents unique disease or is part of spectrum of EBV-associated B-cell lymphoproliferative disorders
ETIOLOGY/PATHOGENESIS
Epstein-Barr Virus
• Due to dysregulated immune surveillance of EBV-infected B cells, particularly by CD8(+) T cells
• Type III latency pattern, LMP and EBNA2(+)
Immunodeficiency
• Most have no clearly defined underlying immunodeficiency
• However, some patients have had allogeneic organ transplant, HIV infection, X-linked lymphoproliferative disorder, and Wiskott-Aldrich syndrome
Cytokines
• IP10 and Mig are implicated in pathogenesis of blood vessel damage
CLINICAL ISSUES
Epidemiology
• Age
Mostly adults, commonly in 6th decade
Children with immunodeficiency syndromes
• Sex
M:F > 2.0:1.0
Site
• Most common site is lung; skin is most frequent extrapulmonary site
For skin lesions, often trunk or limbs, cutaneous nodules often develop after pulmonary disease
May show any anatomic distribution, but usually spares bone marrow, lymph nodes, and spleen
Presentation
• Most commonly as erythematous subcutaneous and dermal nodules
• Pulmonary symptoms (cough and dyspnea)
Treatment
• Grade 1 and grade 2 may be treated more conservatively
Interferon α has been used
• Grade 3 lesions show some response to aggressive chemotherapy + rituximab
Only gold members can continue reading. Log In or Register to continue

 Can show similar histologic features to LYG with inflammation of blood vessels and involvement of multiple organ systems
Can show similar histologic features to LYG with inflammation of blood vessels and involvement of multiple organ systems
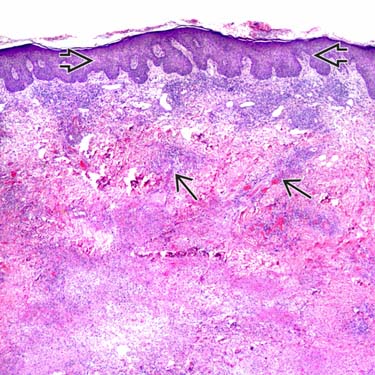
 . The epidermis
. The epidermis  is not involved. (Courtesy M. Royer, MD.)
is not involved. (Courtesy M. Royer, MD.)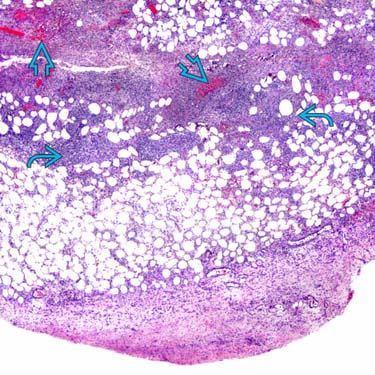
 can mimic a reactive panniculitis. There is angiocentric involvement with tumor cells surrounding and infiltrating blood vessels
can mimic a reactive panniculitis. There is angiocentric involvement with tumor cells surrounding and infiltrating blood vessels  .
.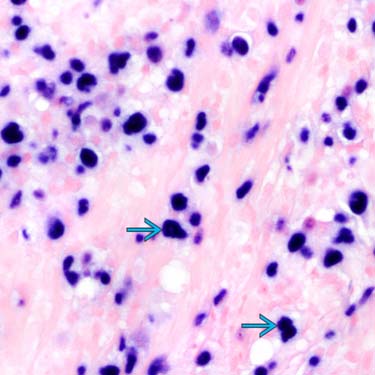
 and show some nuclear irregularity. The smaller reactive T cells are EBER(-).
and show some nuclear irregularity. The smaller reactive T cells are EBER(-).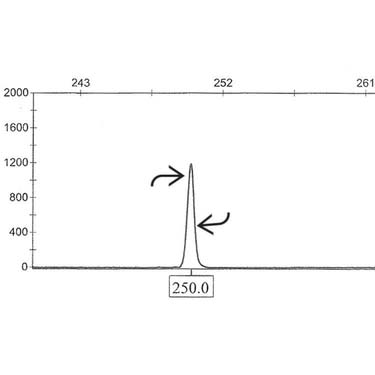
 . IGH gene rearrangements are often detected in LYG since it is a B-cell lymphoma.
. IGH gene rearrangements are often detected in LYG since it is a B-cell lymphoma.









