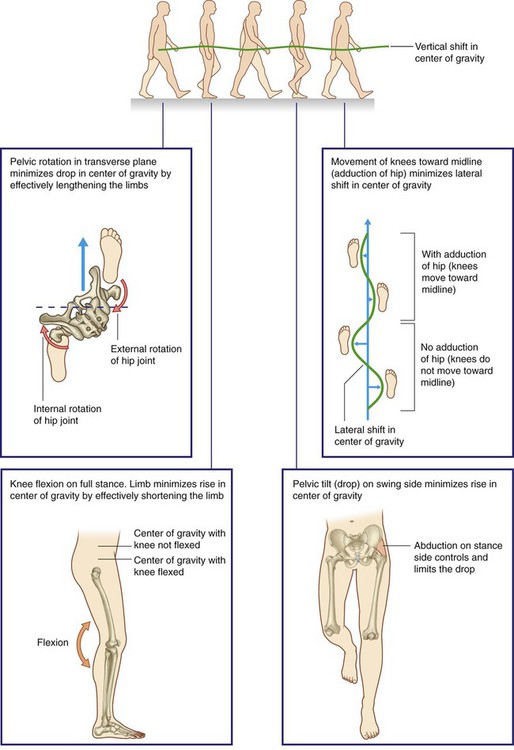
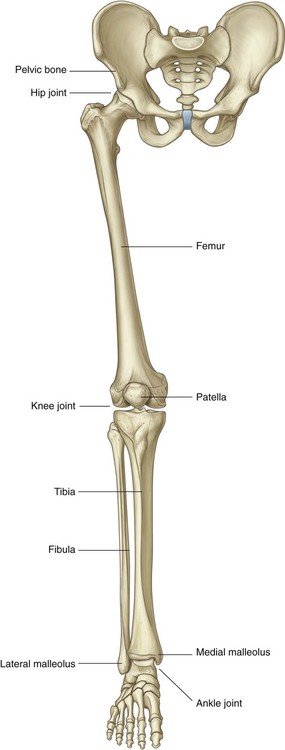
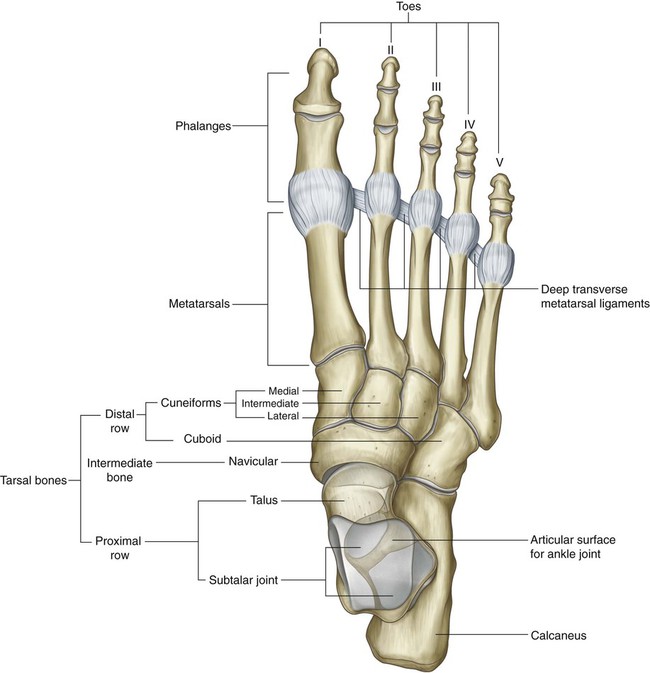
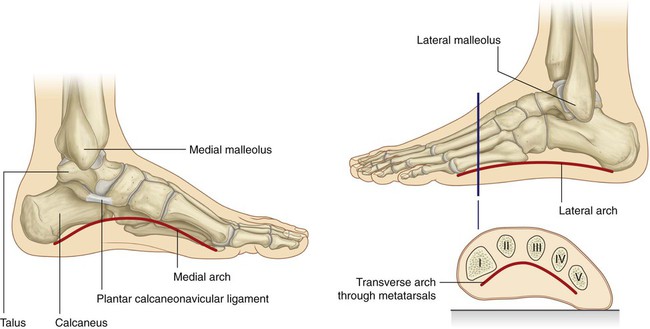
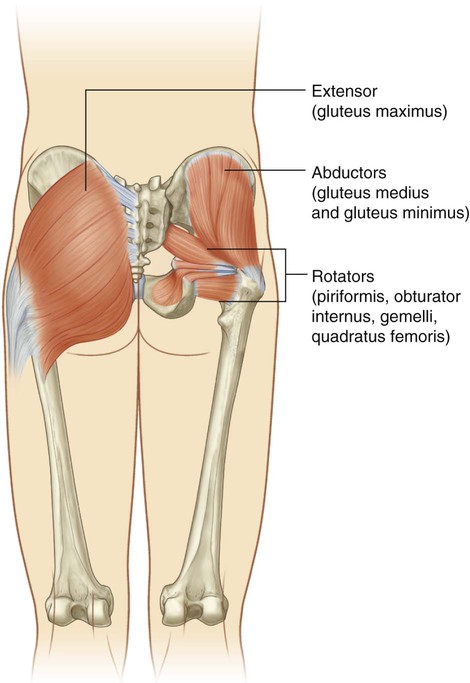
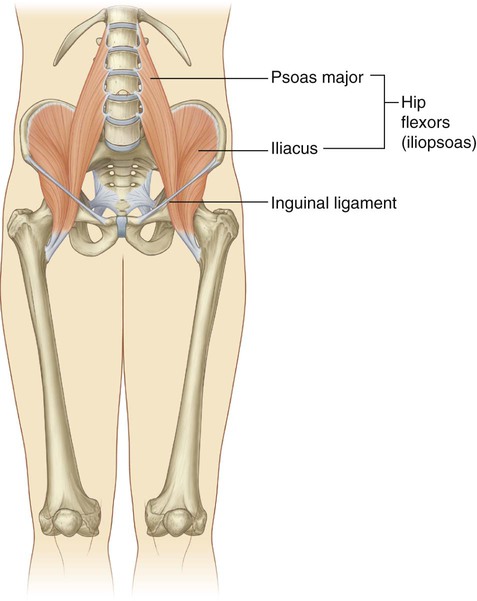
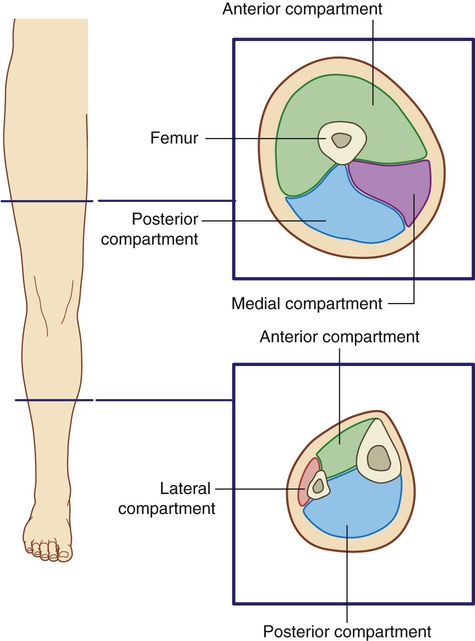
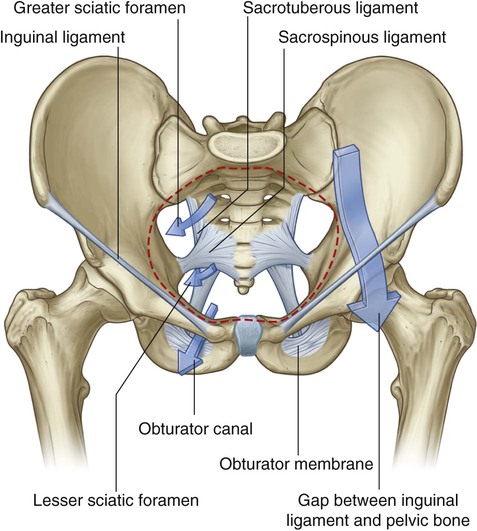
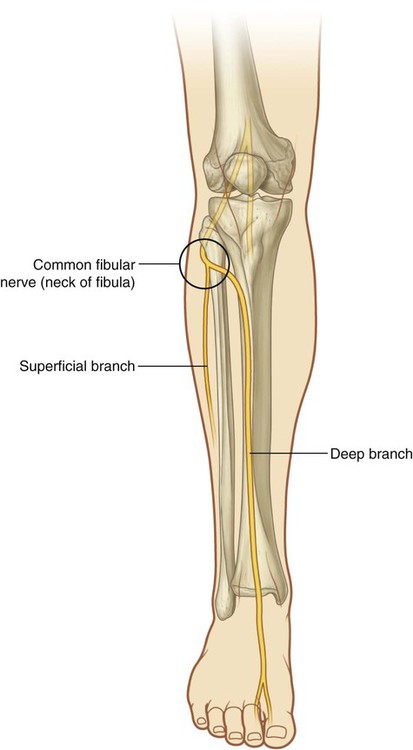
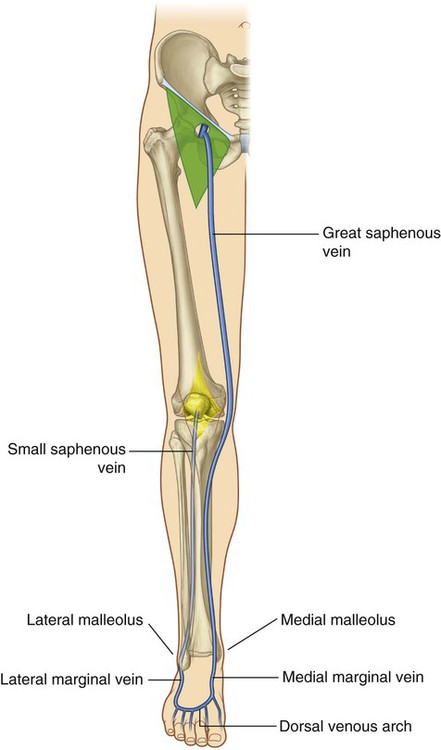
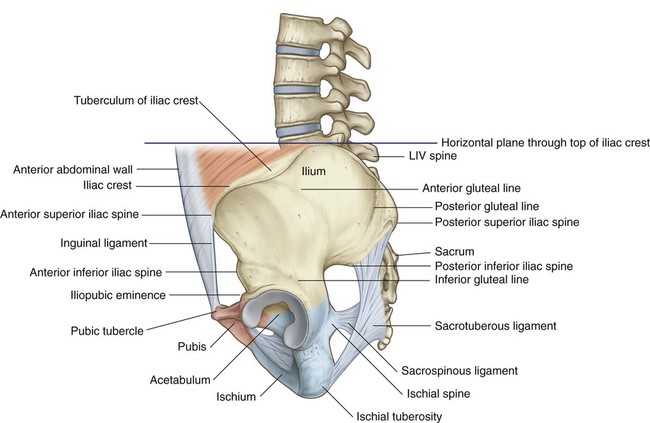
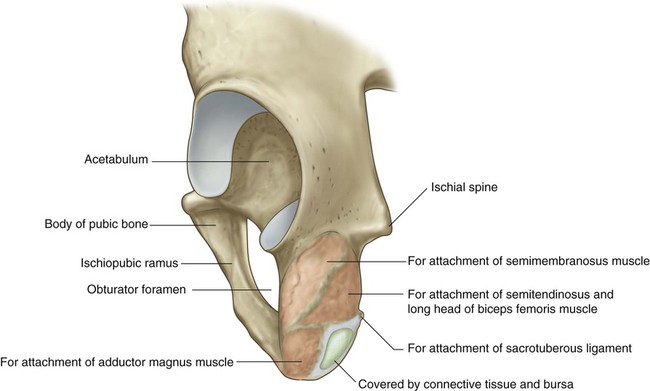
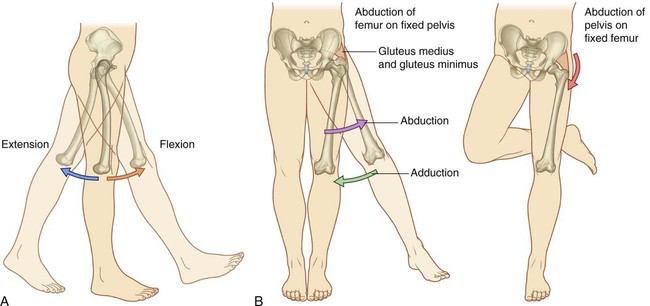
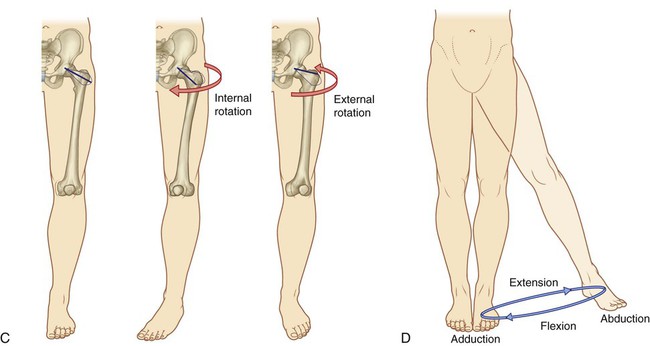
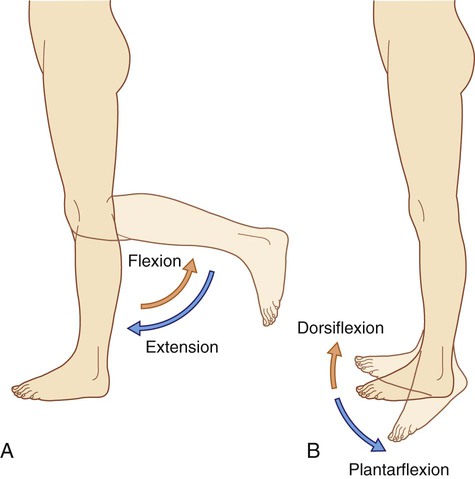
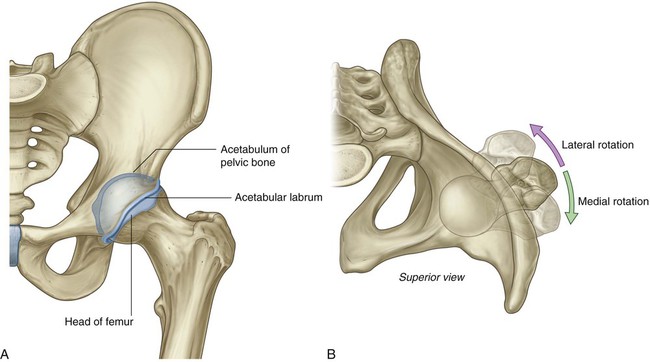
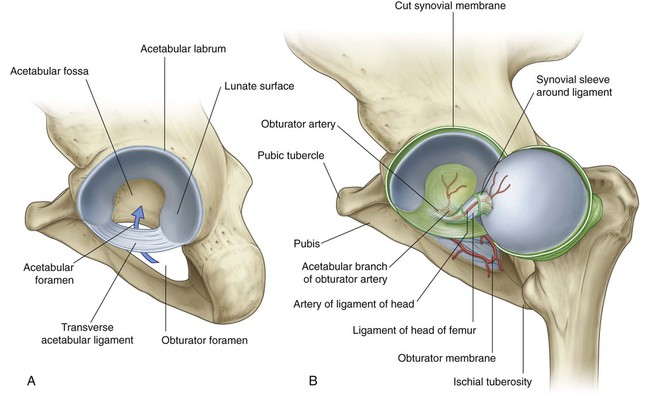
6 ADDITIONAL LEARNING RESOURCES for Chapter 6, Lower Limb, on STUDENT CONSULT (www.studentconsult.com): The lower limb is directly anchored to the axial skeleton by a sacroiliac joint and by strong ligaments, which link the pelvic bone to the sacrum. It is separated from the abdomen, back, and perineum by a continuous line (Fig. 6.1), which: The lower limb is divided into the gluteal region, thigh, leg, and foot on the basis of major joints, component bones, and superficial landmarks (Fig. 6.2): The femoral triangle and popliteal fossa, as well as the posteromedial side of the ankle, are important areas of transition through which structures pass between regions (Fig. 6.3). A major function of the lower limb is to support the weight of the body with minimal expenditure of energy. When standing erect, the center of gravity is anterior to the edge of the SII vertebra in the pelvis (Fig. 6.4). The vertical line through the center of gravity is slightly posterior to the hip joints, anterior to the knee and ankle joints, and directly over the almost circular support base formed by the feet on the ground and holds the knee and hip joints in extension. Movements at the hip joint are flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction (Fig. 6.5). The knee and ankle joints are primarily hinge joints. Movements at the knee are mainly flexion and extension (Fig. 6.6A). Movements at the ankle are dorsiflexion (movement of the dorsal side of the foot toward the leg) and plantarflexion (Fig. 6.6B). During walking, many anatomical features of the lower limbs contribute to minimizing fluctuations in the body’s center of gravity and thereby reduce the amount of energy needed to maintain locomotion and produce a smooth, efficient gait (Fig. 6.7). They include pelvic tilt in the coronal plane, pelvic rotation in the transverse plane, movement of the knees toward the midline, flexion of the knees, and complex interactions between the hip, knee, and ankle. As a result, during walking, the body’s center of gravity normally fluctuates only 5 cm in both vertical and lateral directions. The bones of the gluteal region and the thigh are the pelvic bone and the femur (Fig. 6.8). The large ball and socket joint between these two bones is the hip joint. The bones of the foot consist of the tarsal bones, the metatarsals, and the phalanges (Fig. 6.9). There are seven tarsal bones, which are organized in two rows with an intermediate bone between the two rows on the medial side. Inversion and eversion of the foot, or turning the sole of the foot inward and outward, respectively, occur at joints between the tarsal bones. The interphalangeal joints are hinge joints and allow flexion and extension. The bones of the foot are not organized in a single plane so that they lie flat on the ground. Rather, the metatarsals and tarsals form longitudinal and transverse arches (Fig. 6.10). The longitudinal arch is highest on the medial side of the foot. The arches are flexible in nature and are supported by muscles and ligaments. They absorb and transmit forces during walking and standing. Muscles of the gluteal region consist predominantly of extensors, rotators, and abductors of the hip joint (Fig. 6.11). In addition to moving the thigh on a fixed pelvis, these muscles also control the movement of the pelvis relative to the limb bearing the body’s weight (weight-bearing or stance limb) while the other limb swings forward (swing limb) during walking. Major flexor muscles of the hip (iliopsoas—psoas major and iliacus) do not originate in the gluteal region or the thigh. Instead, they are attached to the posterior abdominal wall and descend through the gap between the inguinal ligament and pelvic bone to attach to the proximal end of the femur (Fig. 6.12). Muscles in the thigh and leg are separated into three compartments by layers of fascia, bones, and ligaments (Fig. 6.13). In the thigh, there are medial (adductor), anterior (extensor), and posterior (flexor) compartments: Muscles in the leg are divided into lateral (fibular), anterior, and posterior compartments: Unlike in the upper limb where most structures pass between the neck and limb through a single axillary inlet, in the lower limb, there are four major entry and exit points between the lower limb and the abdomen, pelvis, and perineum (Fig. 6.14). These are: Nerves originating from the lumbar and sacral plexuses and entering the lower limb carry fibers from spinal cord levels L1 to S3 (Fig. 6.15). Nerves from lower sacral segments innervate the perineum. Terminal nerves exit the abdomen and pelvis through a number of apertures and foramina and enter the limb. As a consequence of this innervation, lumbar and upper sacral nerves are tested clinically by examining the lower limb. In addition, clinical signs (such as pain, pins-and-needles sensations, paresthesia, and fascicular muscle twitching) resulting from any disorder affecting these spinal nerves (e.g., herniated intervertebral disc in the lumbar region) appear in the lower limb. Dermatomes in the lower limb are shown in Fig. 6.16. Regions that can be tested for sensation and are reasonably autonomous (have minimal overlap) are: The dermatomes of S4 and S5 are tested in the perineum. Selected joint movements are used to test myotomes (Fig. 6.17). For example: Each of the major muscle groups or compartments in the lower limb is innervated primarily by one or more of the major nerves that originate from the lumbar and sacral plexuses (Fig. 6.18): In addition to innervating major muscle groups, each of the major peripheral nerves originating from the lumbar and sacral plexuses carries general sensory information from patches of skin (Fig. 6.19). Sensation from these areas can be used to test for peripheral nerve lesions: The common fibular branch of the sciatic nerve curves laterally around the neck of the fibula when passing from the popliteal fossa into the leg (Fig. 6.20). The nerve can be rolled against bone just distal to the attachment of biceps femoris to the head of the fibula. In this location, the nerve can be damaged by impact injuries, fractures to the bone, or leg casts that are placed too high. Large veins embedded in the subcutaneous (superficial) fascia of the lower limb (Fig. 6.21) often become distended (varicose). These vessels can also be used for vascular transplantation. The external surfaces of the pelvic bones, sacrum, and coccyx are predominantly the regions of the pelvis associated with the lower limb, although some muscles do originate from the deep or internal surfaces of these bones and from the deep surfaces of the lumbar vertebrae, above (Fig. 6.22). The ischial tuberosity is posteroinferior to the acetabulum and is associated mainly with the hamstring muscles of the posterior thigh (Fig. 6.23). It is divided into upper and lower areas by a transverse line. When sitting, this medial part supports the body weight. The external surfaces of the ischiopubic ramus anterior to the ischial tuberosity and the body of the pubis provide attachment for muscles of the medial compartment of the thigh (Fig. 6.23). These muscles include the adductor longus, adductor brevis, adductor magnus, pectineus, and gracilis. The large cup-shaped acetabulum for articulation with the head of the femur is on the lateral surface of the pelvic bone in the region where the ilium, pubis, and ischium fuse (Fig. 6.24). The margin of the acetabulum is marked inferiorly by a prominent notch (acetabular notch). The wall of the acetabulum consists of nonarticular and articular parts: In the clinic Pelvic fractures Pelvic fractures can be associated with appreciable blood loss (concealed exsanguination) and blood transfusion is often required. In addition, this bleeding tends to form a significant pelvic hematoma, which can compress nerves, press on organs, and inhibit pelvic visceral function (Fig. 6.25). The femur is the bone of the thigh and the longest bone in the body. Its proximal end is characterized by a head and neck, and two large projections (the greater and lesser trochanters) on the upper part of the shaft (Fig. 6.26). The greater trochanter extends superiorly from the shaft of the femur just lateral to the region where the shaft joins the neck of the femur (Fig. 6.26). It continues posteriorly where its medial surface is deeply grooved to form the trochanteric fossa. The lateral wall of this fossa bears a distinct oval depression for attachment of the obturator externus muscle. The lesser trochanter is smaller than the greater trochanter and has a blunt conical shape. It projects posteromedially from the shaft of the femur just inferior to the junction with the neck (Fig. 6.26). It is the attachment site for the combined tendons of psoas major and iliacus muscles. The intertrochanteric line is a ridge of bone on the anterior surface of the upper margin of the shaft that descends medially from a tubercle on the anterior surface of the base of the greater trochanter to a position just anterior to the base of the lesser trochanter (Fig. 6.26). It is continuous with the pectineal line (spiral line), which curves medially under the lesser trochanter and around the shaft of the femur to merge with the medial margin of the linea aspera on the posterior aspect of the femur. The intertrochanteric crest is on the posterior surface of the femur and descends medially across the bone from the posterior margin of the greater trochanter to the base of the lesser trochanter (Fig. 6.26). It is a broad smooth ridge of bone with a prominent tubercle (the quadrate tubercle) on its upper half, which provides attachment for the quadratus femoris muscle. The shaft of the femur descends from lateral to medial in the coronal plane at an angle of 7° from the vertical axis (Fig. 6.27). The distal end of the femur is therefore closer to the midline than the upper end of the shaft. The linea aspera is a major site of muscle attachment in the thigh. In the proximal third of the femur, the medial and lateral margins of the linea aspera diverge and continue superiorly as the pectineal line and gluteal tuberosity, respectively (Fig. 6.27): The gluteus maximus muscle is attached to the gluteal tuberosity. In the clinic Femoral neck fractures Femoral neck fractures (Fig. 6.28) can interrupt the blood supply to the femoral head. The blood supply to the head and neck is primarily from an arterial ring formed around the base of the femoral neck. From here, vessels course along the neck, penetrate the capsule, and supply the femoral head. The blood supply to the femoral head and femoral neck is further enhanced by the artery of the ligamentum teres, which is generally small and variable. Femoral neck fractures may disrupt associated vessels and lead to necrosis of the femoral head. The hip joint is a synovial articulation between the head of the femur and the acetabulum of the pelvic bone (Fig. 6.29A). The joint is a multiaxial ball and socket joint designed for stability and weight-bearing at the expense of mobility. Movements at the joint include flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction. When considering the effects of muscle action on the hip joint, the long neck of the femur and the angulation of the neck on the shaft of the femur must be borne in mind. For example, medial and lateral rotation of the femur involves muscles that move the greater trochanter forward and backward, respectively, relative to the acetabulum (Fig. 6.29B). The articular surfaces of the hip joint are: Except for the fovea, the head of the femur is also covered by hyaline cartilage. The rim of the acetabulum is raised slightly by a fibrocartilaginous collar (the acetabular labrum). Inferiorly, the labrum bridges across the acetabular notch as the transverse acetabular ligament and converts the notch into a foramen (Fig. 6.30A). The ligament of the head of the femur is a flat band of delicate connective tissue that attaches at one end to the fovea on the head of the femur and at the other end to the acetabular fossa, transverse acetabular ligament, and margins of the acetabular notch (Fig. 6.30B). It carries a small branch of the obturator artery, which contributes to the blood supply of the head of the femur. The synovial membrane attaches to the margins of the articular surfaces of the femur and acetabulum, forms a tubular covering around the ligament of the head of the femur, and lines the fibrous membrane of the joint (Figs. 6.30B and 6.31). From its attachment to the margin of the head of the femur, the synovial membrane covers the neck of the femur before reflecting onto the fibrous membrane (Fig. 6.31). The fibrous membrane that encloses the hip joint is strong and generally thick. Medially, it is attached to the margin of the acetabulum, the transverse acetabular ligament, and the adjacent margin of the obturator foramen (Fig. 6.32A). Laterally, it is attached to the intertrochanteric line on the anterior aspect of the femur and to the neck of the femur just proximal to the intertrochanteric crest on the posterior surface. Vascular supply to the hip joint is predominantly through branches of the obturator artery, medial and lateral circumflex femoral arteries, superior and inferior gluteal arteries, and the first perforating branch of the deep artery of the thigh. The articular branches of these vessels form a network around the joint (Fig. 6.33).
Lower Limb
Conceptual overview
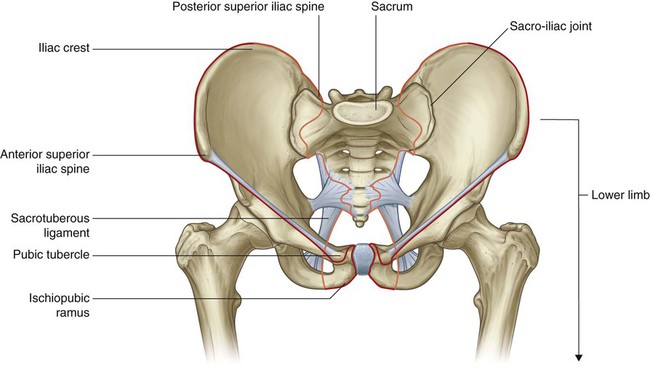
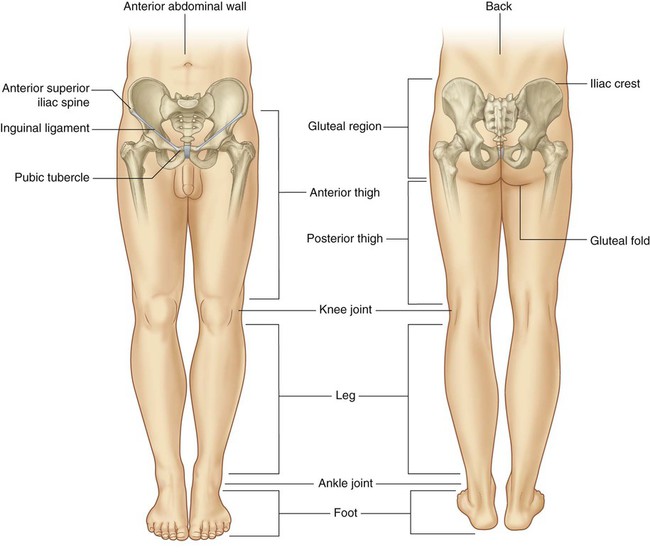
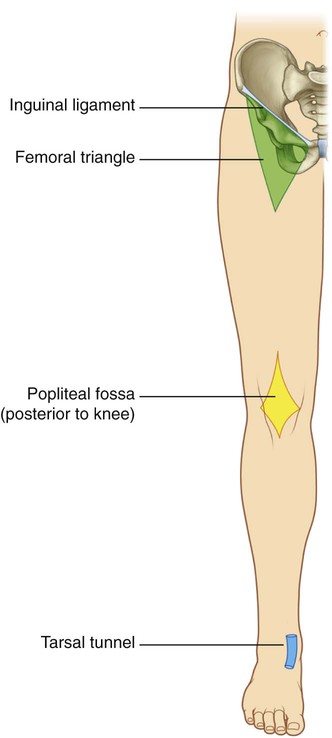
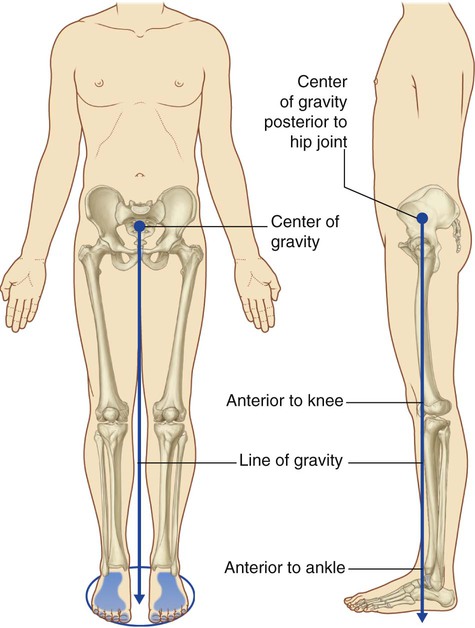
General introduction
 joins the pubic tubercle with the anterior superior iliac spine (position of the inguinal ligament) and then continues along the iliac crest to the posterior superior iliac spine to separate the lower limb from the anterior and lateral abdominal walls;
joins the pubic tubercle with the anterior superior iliac spine (position of the inguinal ligament) and then continues along the iliac crest to the posterior superior iliac spine to separate the lower limb from the anterior and lateral abdominal walls;
 The gluteal region is posterolateral and between the iliac crest and the fold of skin (gluteal fold) that defines the lower limit of the buttocks.
The gluteal region is posterolateral and between the iliac crest and the fold of skin (gluteal fold) that defines the lower limit of the buttocks.
 The leg is between the knee and ankle joint.
The leg is between the knee and ankle joint.
Function
Support the body weight
Locomotion
Component parts
Bones and joints
 The tibia is medial in position, is larger than the laterally positioned fibula, and is the weight-bearing bone.
The tibia is medial in position, is larger than the laterally positioned fibula, and is the weight-bearing bone.
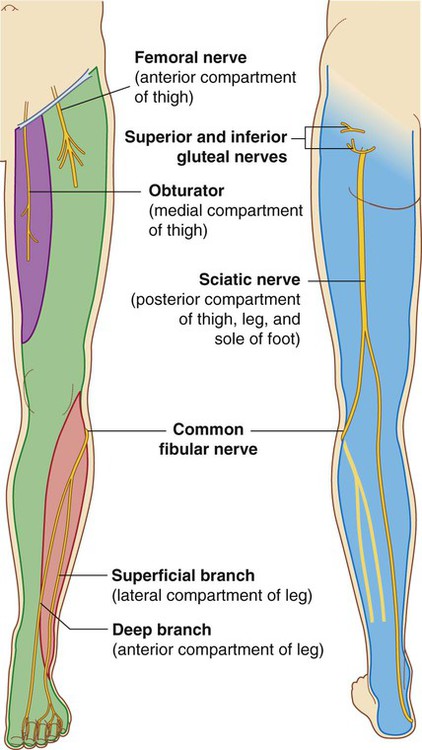
Muscles
 Most muscles in the medial compartment act mainly on the hip joint.
Most muscles in the medial compartment act mainly on the hip joint.
 Muscles in the anterior compartment (quadriceps femoris) predominantly extend the knee.
Muscles in the anterior compartment (quadriceps femoris) predominantly extend the knee.
 Muscles in the lateral compartment predominantly evert the foot.
Muscles in the lateral compartment predominantly evert the foot.
 Muscles in the anterior compartment dorsiflex the foot and extend the digits.
Muscles in the anterior compartment dorsiflex the foot and extend the digits.
Relationship to other regions
 the gap between the inguinal ligament and pelvic bone,
the gap between the inguinal ligament and pelvic bone,
 the obturator canal (at the top of the obturator foramen), and
the obturator canal (at the top of the obturator foramen), and
Key points
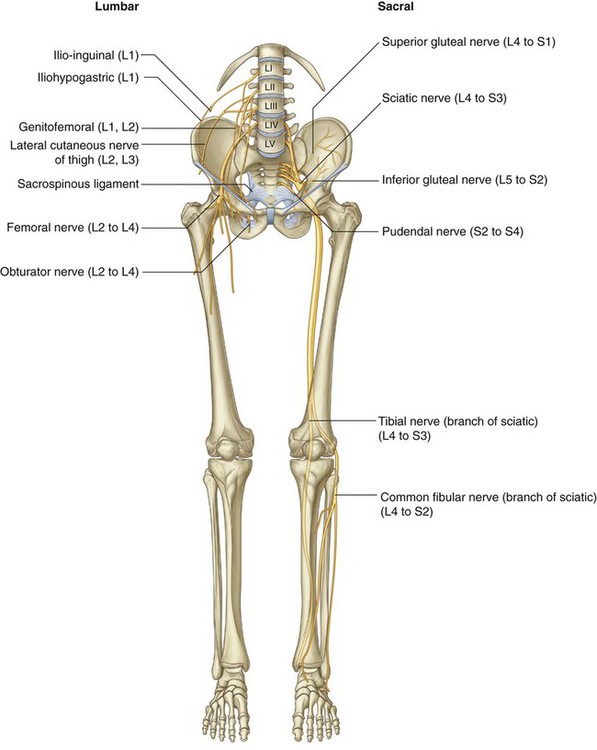
Innervation is by lumbar and sacral spinal nerves
 over the inguinal ligament—L1,
over the inguinal ligament—L1,
 lower medial side of the thigh—L3,
lower medial side of the thigh—L3,
 medial side of the great toe (digit I)—L4,
medial side of the great toe (digit I)—L4,
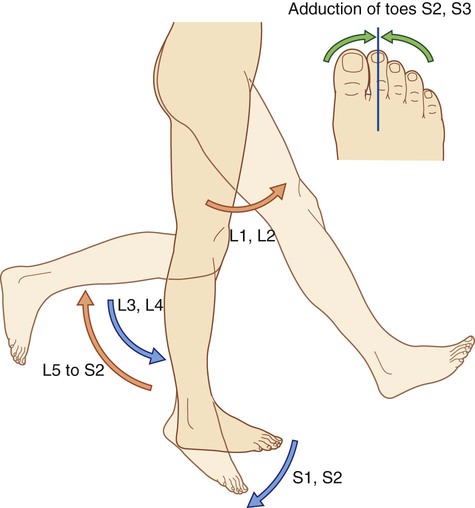
 Flexion of the hip is controlled primarily by L1 and L2.
Flexion of the hip is controlled primarily by L1 and L2.
 Extension of the knee is controlled mainly by L3 and L4.
Extension of the knee is controlled mainly by L3 and L4.
 Knee flexion is controlled mainly by L5 to S2.
Knee flexion is controlled mainly by L5 to S2.
 Plantarflexion of the foot is controlled predominantly by S1 and S2.
Plantarflexion of the foot is controlled predominantly by S1 and S2.
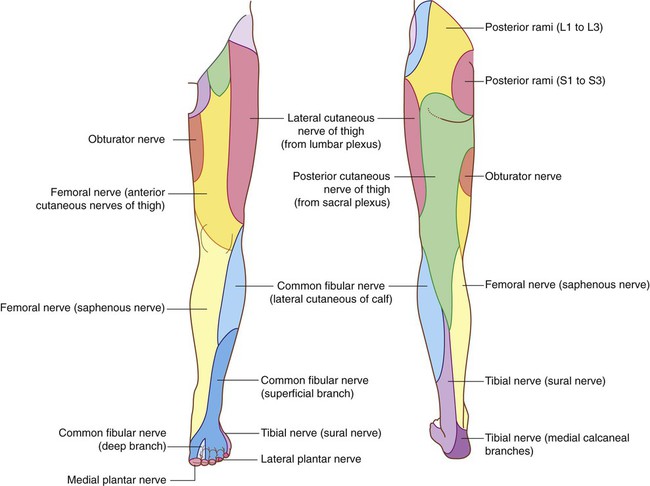
 The femoral nerve innervates skin on the anterior thigh, medial side of the leg, and medial side of the ankle.
The femoral nerve innervates skin on the anterior thigh, medial side of the leg, and medial side of the ankle.
 The obturator nerve innervates the medial side of the thigh.
The obturator nerve innervates the medial side of the thigh.
 The tibial part of the sciatic nerve innervates the lateral side of the ankle and foot.
The tibial part of the sciatic nerve innervates the lateral side of the ankle and foot.
 The common fibular nerve innervates the lateral side of the leg and the dorsum of the foot.
The common fibular nerve innervates the lateral side of the leg and the dorsum of the foot.
Nerves related to bone
Superficial veins
Regional anatomy
Bony pelvis
Ilium
 The inferior gluteal line originates just superior to the anterior inferior iliac spine and curves inferiorly across the bone to end near the posterior margin of the acetabulum—the rectus femoris muscle attaches to the anterior inferior iliac spine and to a roughened patch of bone between the superior margin of the acetabulum and the inferior gluteal line.
The inferior gluteal line originates just superior to the anterior inferior iliac spine and curves inferiorly across the bone to end near the posterior margin of the acetabulum—the rectus femoris muscle attaches to the anterior inferior iliac spine and to a roughened patch of bone between the superior margin of the acetabulum and the inferior gluteal line.
Ischial tuberosity
 The more medial part of the upper area is for the attachment of the combined origin of the semitendinosus muscle and the long head of the biceps femoris muscle.
The more medial part of the upper area is for the attachment of the combined origin of the semitendinosus muscle and the long head of the biceps femoris muscle.
 The lateral part is for the attachment of the semimembranosus muscle.
The lateral part is for the attachment of the semimembranosus muscle.
 The lateral region provides attachment for part of the adductor magnus muscle.
The lateral region provides attachment for part of the adductor magnus muscle.
 The medial part faces inferiorly and is covered by connective tissue and by a bursa.
The medial part faces inferiorly and is covered by connective tissue and by a bursa.
Ischiopubic ramus and pubic bone
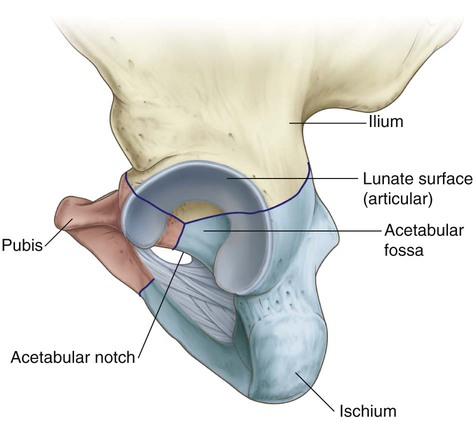
Acetabulum
 The nonarticular part is rough and forms a shallow circular depression (the acetabular fossa) in central and inferior parts of the acetabular floor—the acetabular notch is continuous with the acetabular fossa.
The nonarticular part is rough and forms a shallow circular depression (the acetabular fossa) in central and inferior parts of the acetabular floor—the acetabular notch is continuous with the acetabular fossa.
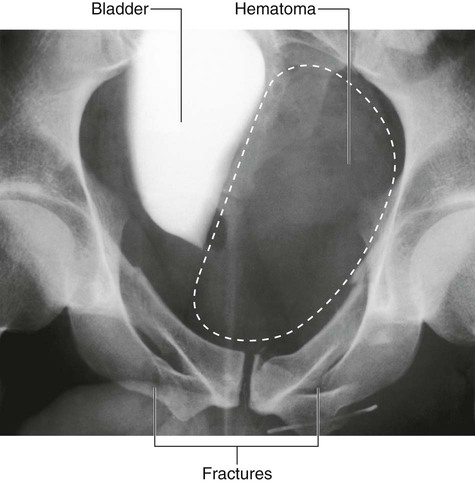
 Type 1 injuries occur without disruption of the bony pelvic ring (e.g., a fracture of the iliac crest). These types of injuries are unlikely to represent significant trauma, though in the case of a fracture of the iliac crest, blood loss needs to be assessed.
Type 1 injuries occur without disruption of the bony pelvic ring (e.g., a fracture of the iliac crest). These types of injuries are unlikely to represent significant trauma, though in the case of a fracture of the iliac crest, blood loss needs to be assessed.
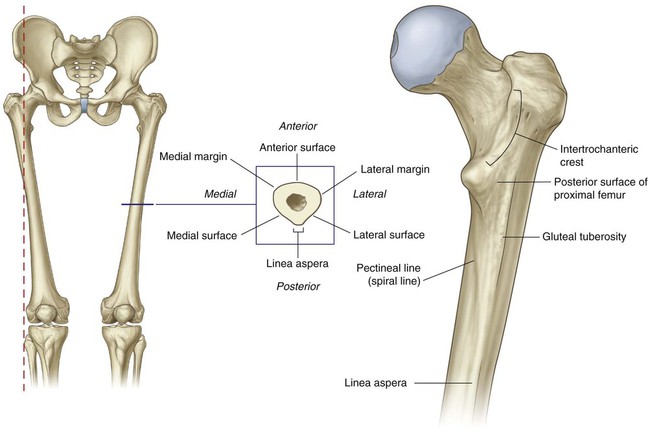
Proximal femur
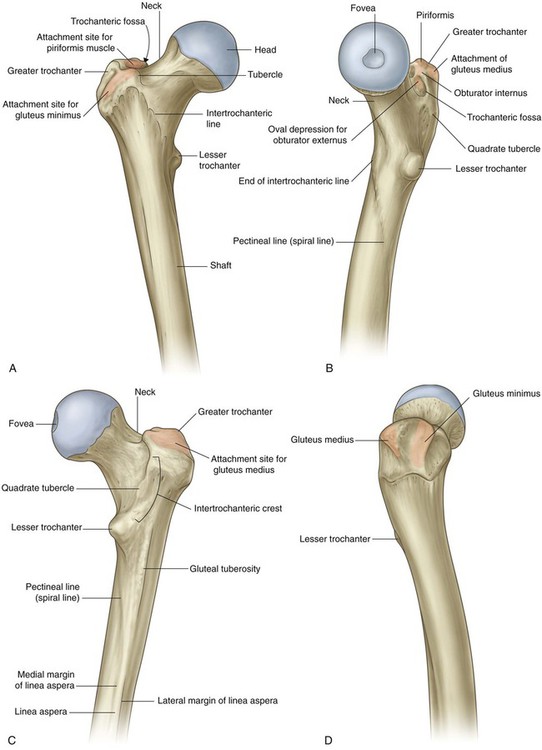
Greater and lesser trochanters
Intertrochanteric line
Intertrochanteric crest
Shaft of the femur
 The pectineal line curves anteriorly under the lesser trochanter and joins the intertrochanteric line.
The pectineal line curves anteriorly under the lesser trochanter and joins the intertrochanteric line.
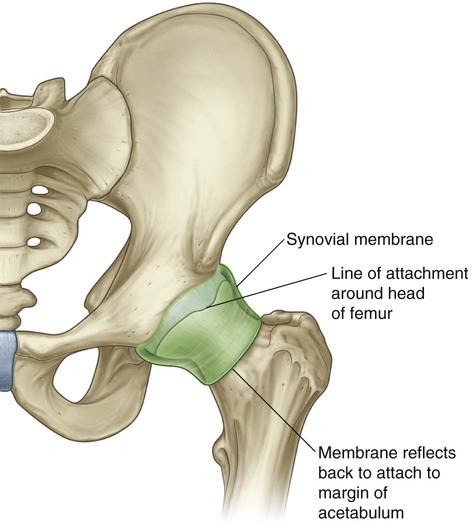
Hip joint
Ligaments
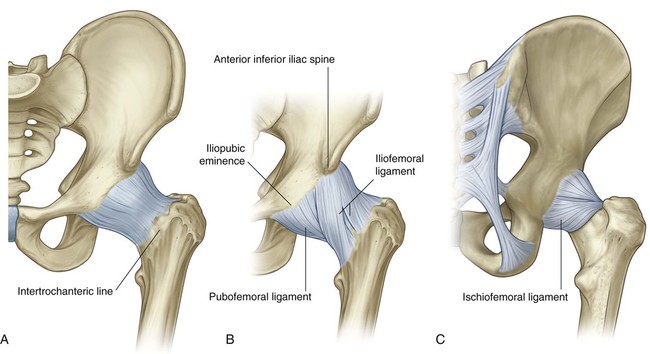
 The iliofemoral ligament is anterior to the hip joint and is triangular shaped (Fig. 6.32B). Its apex is attached to the ilium between the anterior inferior iliac spine and the margin of the acetabulum and its base is attached along the intertrochanteric line of the femur. Parts of the ligament attached above and below the intertrochanteric line are thicker than the part attached to the central part of the line. This results in the ligament having a Y appearance.
The iliofemoral ligament is anterior to the hip joint and is triangular shaped (Fig. 6.32B). Its apex is attached to the ilium between the anterior inferior iliac spine and the margin of the acetabulum and its base is attached along the intertrochanteric line of the femur. Parts of the ligament attached above and below the intertrochanteric line are thicker than the part attached to the central part of the line. This results in the ligament having a Y appearance.
 The pubofemoral ligament is anteroinferior to the hip joint (Fig. 6.32B). It is also triangular in shape, with its base attached medially to the iliopubic eminence, adjacent bone, and obturator membrane. Laterally, it blends with the fibrous membrane and with the deep surface of the iliofemoral ligament.
The pubofemoral ligament is anteroinferior to the hip joint (Fig. 6.32B). It is also triangular in shape, with its base attached medially to the iliopubic eminence, adjacent bone, and obturator membrane. Laterally, it blends with the fibrous membrane and with the deep surface of the iliofemoral ligament.
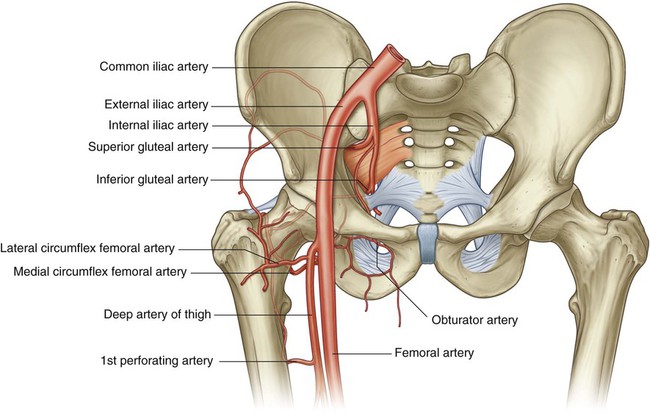
 The ischiofemoral ligament reinforces the posterior aspect of the fibrous membrane (Fig. 6.32C). It is attached medially to the ischium, just posteroinferior to the acetabulum, and laterally to the greater trochanter deep to the iliofemoral ligament.
The ischiofemoral ligament reinforces the posterior aspect of the fibrous membrane (Fig. 6.32C). It is attached medially to the ischium, just posteroinferior to the acetabulum, and laterally to the greater trochanter deep to the iliofemoral ligament.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree