Chapter 13 Local Anesthetics
| Abbreviations | |
|---|---|
| CNS | Central nervous system |
| Epi | Epinephrine |
| IV | Intravenous |
| VGSC | Voltage-gated sodium channels |
Therapeutic Overview
Local anesthetics reversibly block the generation and conduction of action potentials in all excitable cells. These drugs have many uses in medicine ranging from dental to obstetric procedures, because they prevent painful stimuli from being perceived in a specific part of the body into which they have been locally administered. Local anesthetics can also affect an entire region of the body when injected (e.g., when injected into the spinal cord). The first known local anesthetic, cocaine, is a natural product, but its abuse liability (see Chapter 37) precludes most of its clinical uses except in ophthalmology. These anesthetics may be applied locally by subcutaneous infiltration for the removal of a superficial skin lesion or may be applied to the spinal cord as a regional anesthetic for a hip replacement procedure or for the management of postoperative pain. Thus the selection of a local anesthetic depends on the pharmacokinetic profile required for each specific use and on the side effect profile of the compound, factors summarized in the Therapeutic Overview Box.
| Therapeutic Overview |
|---|
| Factors in drug selection |
| Speed of onset |
| Duration of effect |
| Side effects |
| Seizures |
| Cardiovascular depression |
Mechanisms of Action
and all neurons in the central nervous system (CNS). Thus the actions of these compounds can be restricted by administering them locally. Certain practical pharmacokinetic properties make these agents particularly useful in temporarily blocking the sensory transmission of pain impulses. The greatest advantage of local anesthetics is their reversibility—that is, once the drug is eliminated by metabolism, diffusion from its injection site, or excreted, the nerve resumes normal function. There are generally no long-term consequences from the use of local anesthetics. Thus these drugs are highly effective in providing regional or localized reversible pain relief.
The resultant K+ efflux through these and non–voltage-gated K+ channels returns the membrane potential to its normal resting value. This mechanism is depicted in Figure 13-1.
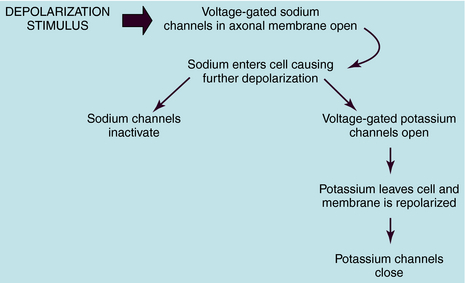
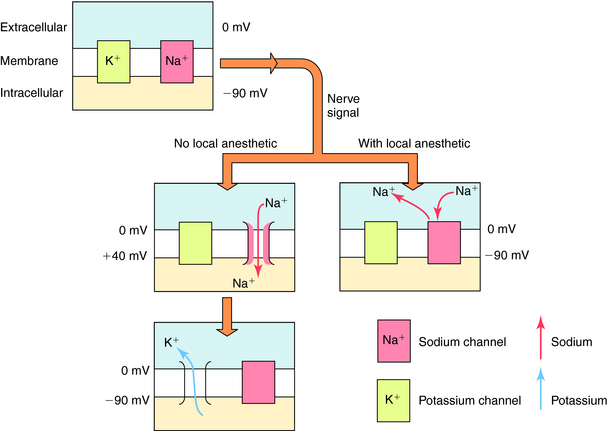
The cellular physiological mechanism by which local anesthetics block the conduction of nerve impulses is well understood. These drugs bind selectively to VGSCs at the intracellular surface of the channel pore near the pore’s vestibule and thereby block the pathway for Na+ and prevent the channels from opening (Fig. 13-2). By blocking Na+ influx, these drugs prevent the depolarization necessary for action potential propagation and, at sufficient concentrations, block impulse conduction. Because local anesthetics dissociate from the VGSC very rapidly, once drug administration is stopped, the drug diffuses away from the nerve and/or is absorbed by the local circulation, and impulse activity is restored.
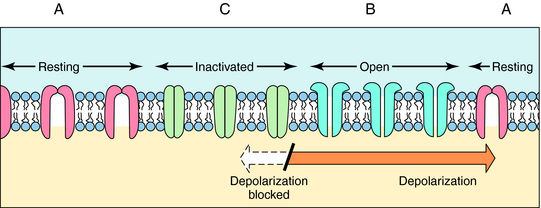
The ability of local anesthetics to block VGSC is highly dependent on the activity (or state) of the channel. Na+ channels exist in three major states (Fig.13-3). In the resting closed state, the channels do not allow Na+ influx and are highly sensitive to depolarization-induced opening. In the open state, the channels allow Na+ influx, whereas in the inactivated closed state, they do not allow Na+ influx and are not opened by depolarization. Local anesthetics have different potencies for binding to these different states. They are much more likely to bind when the channels are active, open, or inactivated and are less likely to bind to the resting state. This modulation of affinity is called activity (or state) dependence and has great practical importance. Because local anesthetics preferentially block nerves in which Na+ channels are open or inactivated (activity-dependent), they are more potent in rapidly firing nerves than in nerves in which action potentials occur less frequently. Because sensory neurons fire at greater frequencies in response to more intense noxious stimuli, the effectiveness of impulse blockade is greater under these conditions.
Pharmacokinetics
The structures of the local anesthetics have a direct bearing on their therapeutic actions (Fig. 13-4). All of these agents contain a hydrophobic group linked by either an ester or an amide bond to a relatively hydrophilic group (usually a tertiary or quaternary amine). This hydrophilic group makes the drug H2O-soluble, enabling the agent to diffuse to the nerve. The hydrophobic group makes the agent lipid soluble and enables the drug to penetrate the lipid membranes (sheath, perineural tissue, and nerve membrane) to reach its binding site on the inner surface of the VGSC. The more hydrophobic local anesthetics bind more tightly to the channel.
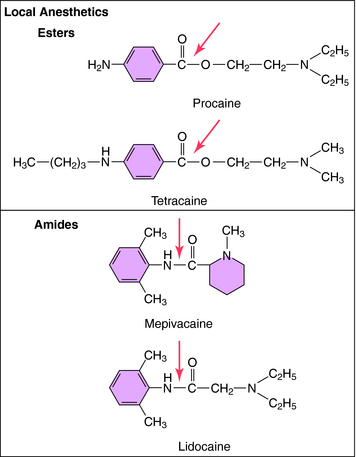
FIGURE 13–4 Structures of the two types of local anesthetics depicting sites of hydrolysis (shown with arrows).
Local anesthetics must cross the neuronal cell membrane to reach the VGSC; therefore sufficient amounts of the drugs must be in the unionized form to gain entry to the cell. However, the charged form of the compound is thought to be most active. Thus an important chemical aspect of local anesthetics is that they are weak bases, with pKa values of 8 to 9. At physiological pH (~7.4), most (80% to 90%) of the drug is in the ionized (charged) form (see Chapter 2). Once inside the cell, the predominant ionized form of the agent binds to the Na+ channel proteins.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


