Chapter 8 Lower Limb
Chapter 8 Lower Limb
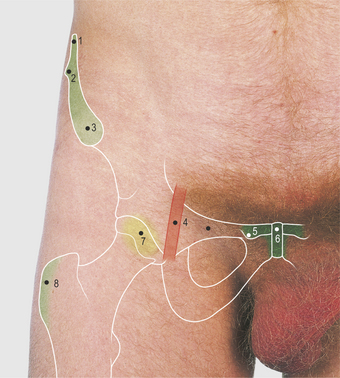
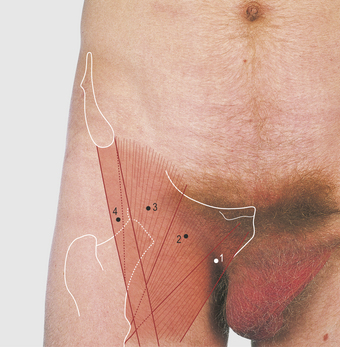
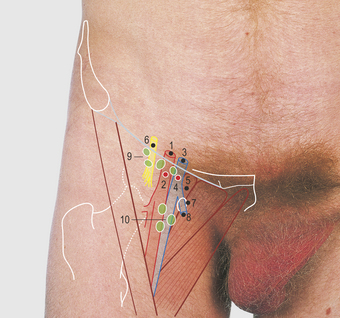
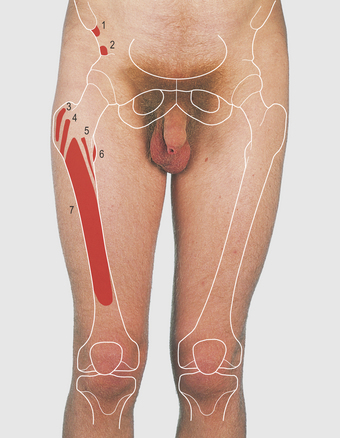
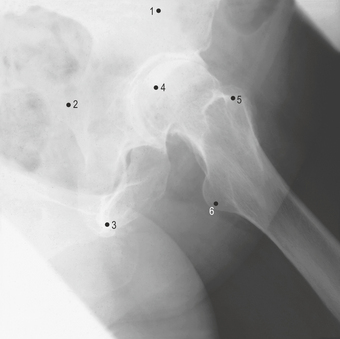
Femoral triangle (Figs 8.1—8.8)
The symphysis, body, crest and tubercle of the pubis, and the anterior superior iliac spine of the pelvis are palpable anteriorly (Fig. 8.3). The inguinal ligament passes between the anterior superior iliac spine and the pubic tubercle, and forms about three-quarters of the base of the femoral triangle (the rest continues across the body of the pubis — Figs 8.6, 8.8). The lateral border of the triangle is formed by the sartorius muscle. This muscle passes from the anterior superior iliac spine distally, across the thigh, to be attached to the medial subcutaneous surface of the upper tibia. Its function is best described as producing the crossed-leg position and it is known as the tailor’s muscle; it is supplied by the femoral nerve.




Anterior and medial aspect of the hip, thigh and knee (Figs 8.9—8.15)
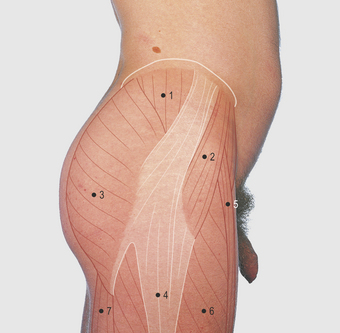
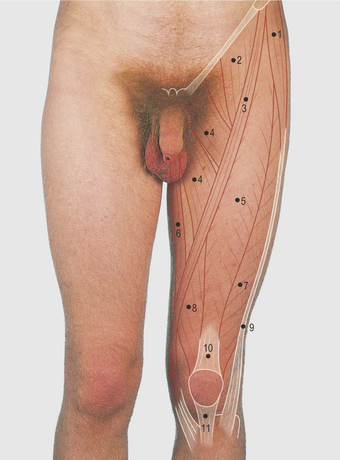
Anterior and medial aspect of the thigh
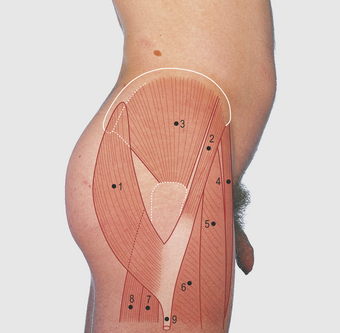
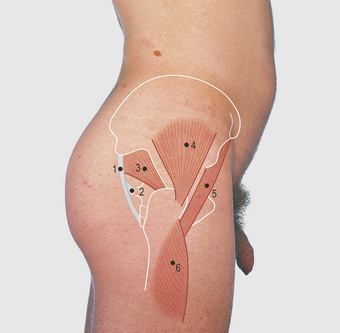
The anterior aspect of the thigh is formed mainly of the large quadriceps muscle mass (Fig. 8.13). The quadriceps has four proximal attachments: the rectus femoris is attached by a straight head to the anterior inferior iliac spine, and by an oblique head to just above the acetabulum. The vastus lateralis and medialis take their attachment from their respective sides of the intertrochanteric line, encircle the subtrochanteric femur, then converge to their respective sides of the linea aspera of the femur and the vastus intermedialis from the anterior aspect of the femoral shaft. The quadriceps muscle is attached inferiorly to the patella and is extended beyond it to form a strong tendon, the patellar ‘ligament’, attached to the tibial tuberosity. The patella is subcutaneous and easily palpable, as is the tibial tuberosity.

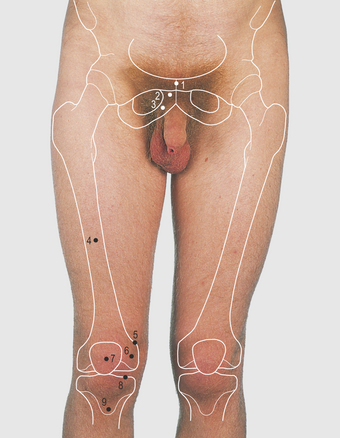
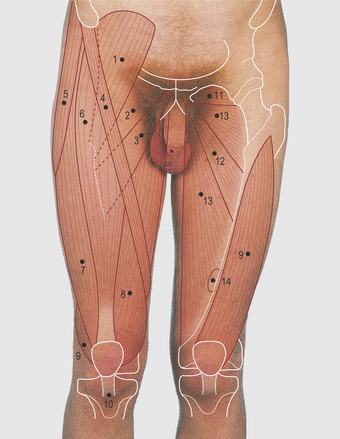
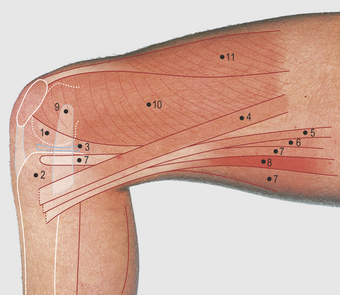
8.13 Anterior and medial aspect of the thigh: superficial (right limb) and deep (left limb) muscles
(Items 6–10 make up the quadriceps muscle)
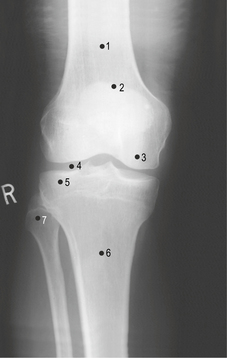
On each side of the patellar ligament, the capsule of the joint is formed largely of downward fibrous expansions of the quadriceps tendon known as retinacula, through which the muscle gains attachment to the tibial condyles. The muscle is supplied by the femoral nerve. The proximal components of the quadriceps are not easily demonstrated when recumbent, or during easy standing, but are clearly seen when the whole leg, with extended knee, is raised against gravity; the patellar ligament and the lower horizontal fibres of the vastus medialis, passing to the medial aspect of the patella, are visible. The latter fibres quickly waste away with inactivity. The medial and lateral femoral condyles and the upper margin of the tibia can be palpated over most of the anterior, medial and lateral aspects of the knee joint (Figs 8.15, 8.30, pp. 105, 109).
The medial side of the thigh contains the adductor group of muscles. The first layer, the pectineus and the adductor longus, has been described in the femoral triangle; the adductor brevis passes from the inferior pubic ramus to the linea aspera between these muscles and the more deeply placed powerful adductor magnus (Fig. 8.13). The latter is attached medially along the ischiopubic ramus and ischial tuberosity and, laterally, to the length of the linea aspera and the medial supracondylar ridge and by a strong tendon to the adductor tubercle on the femur. The tubercle is palpable. The femoral vessels pass through a defect (the adductor hiatus) in this asperal attachment close to the femur; at this point they become the popliteal vessels. The opening is approximately 10 cm above the knee joint. The adductor muscles are overlain by the gracilis muscle, a thin flat (gracile) muscle passing from the inferior pubic ramus to the upper medial aspect of the tibia. The gracilis and the adductor muscles adduct the hip joint and are supplied by the obturator nerve. The adductor magnus also has a sciatic nerve supply to that part arising from the ischial tuberosity; this is functionally and developmentally a part of the hamstring muscle group extending the hip joint.
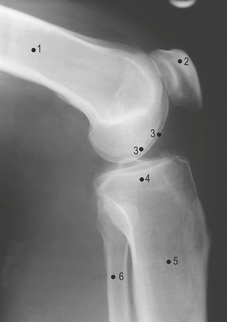
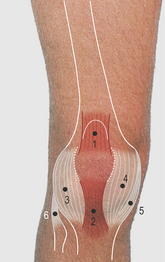
Medial aspect of the knee
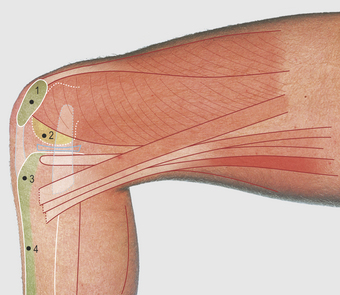
The medial collateral ligament of the knee joint is a wide, flat, strong sheet blending with the capsule of the joint, passing from the medial epicondyle of the femur to the upper surface of the tibial shaft (Fig. 8.17). The medial edge of the medial meniscus is between the femoral and tibial condyles; although it is normally impalpable, if damaged, tenderness can be noted along the joint line and there may be a protrusion over the site of a tear. The tendons of the sartorius, gracilis and semitendinosus are attached to the subcutaneous upper surface of the tibia, from anterior to posterior; they are more easily defined with the knee flexed to a right angle.
Medical aspect of the flexed knee (Figs 8.16—8.18)

Lateral aspect of the hip, thigh and knee (Figs 8.19—8.25)
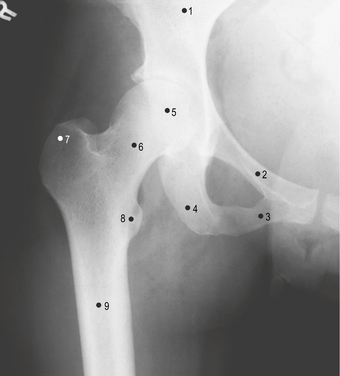
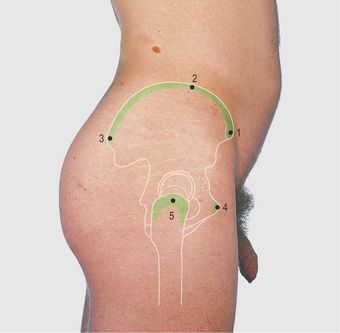
Lateral aspect of the hip

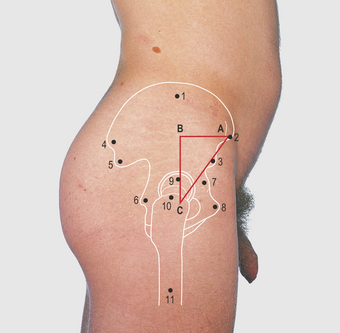

In fractures of the neck of the femur the distance BC in the triangle shown in Figure 8.20 (Bryant’s triangle) is shortened and this can be demonstrated by comparing the normal and fractured sides.
Lateral aspect of the knee
The biceps tendon can be clearly defined over the lateral aspect of the knee when the knee is flexed to a right angle; the tendon can be followed to its attachment to the upper end of the fibula (Figs 8.29, 8.30 and 8.62, pp. 109, 120). The bony margin of the lateral aspect of the tibial condyle can be palpated and the fibular (lateral collateral) ligament felt as a firm cord, separate from the joint capsule, passing from the lateral aspect of the femoral condyle to the head of the fibula. The lateral meniscus lies adjacent to the tibial margin and becomes tender and sometimes palpable when damaged. The common peroneal nerve is overlapped by the tendon of the biceps and then passes subcutaneously over the neck of the fibula, where it can be palpated, before it divides into deep and superficial branches that enter the anterior and lateral compartments of the leg, respectively.