Leiomyoma (Pilar)
Cyril Fisher, MD, DSc, FRCPath
Key Facts
Terminology
Benign cutaneous smooth muscle neoplasm arising from arrector pili muscles
Etiology/Pathogenesis
Many are shown to have germline fumarate hydratase gene mutations
May be associated with uterine leiomyomas and renal cell carcinoma
Clinical Issues
Most develop in adolescence or early adulthood
Predilection for extensor surfaces of extremities as well as trunk
Most often present with multiple painful pink or brown papules
Microscopic Pathology
Bundles and fascicles of differentiated smooth muscle cells
Proliferation is unencapsulated, haphazardly arranged, with irregular borders, and confined to dermis
Degenerative atypia and occasional mitotic figures (up to 1 per 10 HPF) are acceptable
Top Differential Diagnoses
Genital leiomyoma
Angioleiomyoma (vascular leiomyoma)
Smooth muscle hamartoma
Dermatomyofibroma
Myofibroma
Superficial leiomyosarcoma
 Multiple cutaneous leiomyomas are seen involving the chest, lower neck, shoulder, and upper arm. Typical of superficial leiomyomas, these lesions tend to involve more than 1 body site and extensor surfaces. |
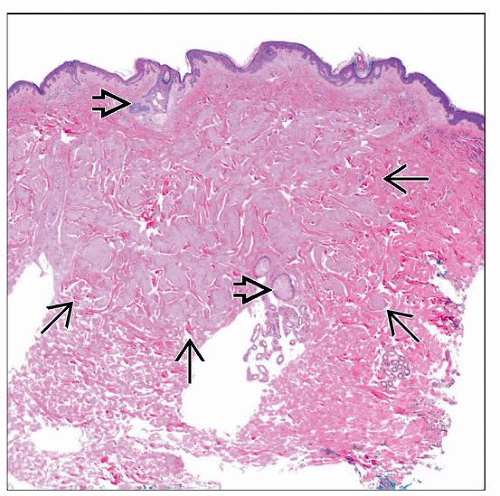 Low-power image shows superficial (pilar) leiomyoma involving most of the dermis. The lesion is unencapsulated and has an irregular border  with displacement of dermal appendages with displacement of dermal appendages  . . |
TERMINOLOGY
Synonyms
Cutaneous leiomyoma, pilar leiomyoma, piloleiomyoma, leiomyoma cutis
Definitions
Uncommon benign cutaneous smooth muscle neoplasm originating from arrector pili muscles
ETIOLOGY/PATHOGENESIS
Genetics
Some cases are familial
Autosomal dominant inheritance pattern with incomplete penetrance
Most patients are shown to have germline fumarate hydratase gene mutations
Gene on 1q43 and enzyme involved with tricarboxylic acid (Krebs) cycle
May be associated with uterine leiomyomas (98%) and renal cell carcinoma (10-15%)
Syndrome known as hereditary leiomyomatosis and renal cell cancer, multiple cutaneous and uterine leiomyomatosis syndrome, or Reed syndrome
Renal cell carcinomas are usually papillary, tubulopapillary, or collecting duct type
CLINICAL ISSUES
Epidemiology
Age
Most develop in adolescence or early adulthood
Some are congenital or develop in childhood
Site
Predilection for extensor surfaces of extremities, trunk, and head & neck
2 or more body sites are often affected
Presentation
Most often multiple painful pink or brown papules
Papules may coalesce into nodules
Lesions tend to follow dermatomal distribution
Pain can be induced by cold exposure, pressure, or states of emotion
Rare cases are solitary and painless
Treatment
Options, risks, complications
Depends on number of lesions and symptomatology
Medical management with follow-up is option for those with extensive lesions
Imaging to rule out renal mass or large atypical uterine lesions is warranted
Cryotherapy and laser ablation have been used with mixed results
Surgical approaches
For localized and symptomatic lesions
Prognosis
Does not undergo malignant change
Surgically treated lesions often develop recurrence (more likely representing new lesions)
MACROSCOPIC FEATURES
Size
Most < 2 cm
MICROSCOPIC PATHOLOGY
Histologic Features
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


