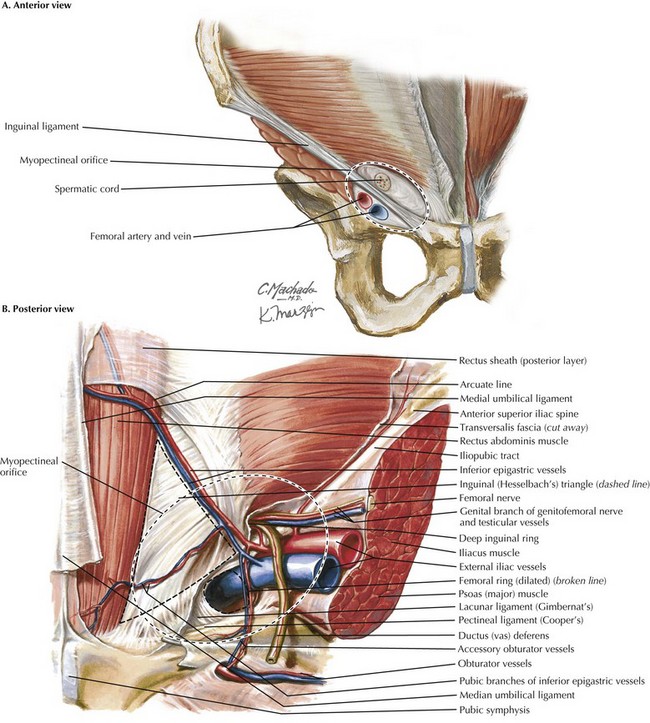
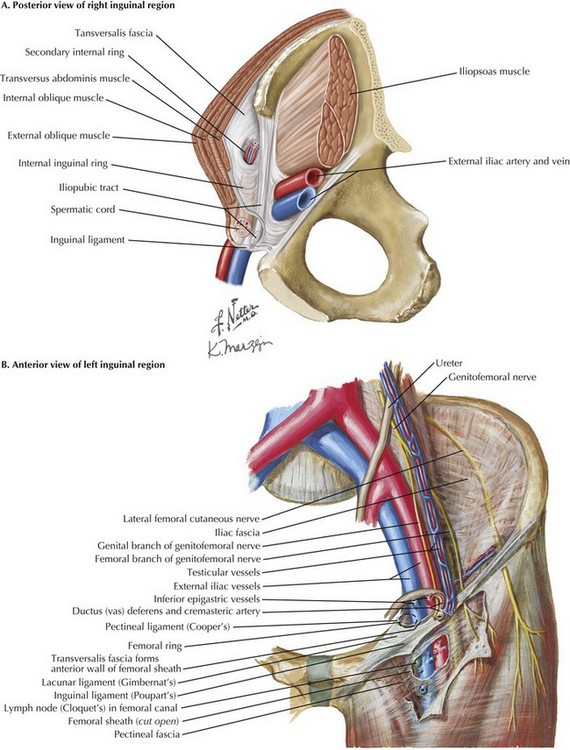
Chapter 29 The myopectineal orifice is one of the most important anatomic features of the groin anatomy (Fig. 29-1, dashed ovals). All hernias of the groin originate from this single zone of weakness, which is covered only by transversalis fascia and peritoneum. Bisected by the inguinal ligament, the myopectineal orifice comprises the inguinal canal superiorly and the femoral canal inferiorly. The inferior border consists of the superior pubic ramus and the pectineal (Cooper’s) ligament. Medially, the myopectineal orifice is bordered by the rectus abdominis muscle and the inguinal falx (conjoined tendon). The conjoined (conjoint) tendon (fusion of internal oblique muscle and transversalis fascia) is also the superior border of the orifice. Laterally, the boundaries consist of the iliopsoas muscle and lateral border of the femoral sheath. Although a key anatomic landmark for open (anterior) inguinal hernia repair, the inguinal ligament is not seen in the laparoscopic (posterior) repair because it is an anterior lamina structure (Fig, 29-2, A). The inguinal (Poupart’s) ligament is the inferior edge of the external oblique aponeurosis, extending from the ASIS to the pubic tubercle, turning posteriorly to form the “shelving edge.” This shelving edge is used to secure the inferior border of the mesh in an open inguinal hernia repair (see Chapter 28). The iliopubic tract is the continuation of the transversus abdominis aponeurosis and fascia. It is located posterior to the inguinal ligament, extends from the pubic tubercle medially, and passes over the femoral vessels to insert on the ASIS laterally. This posterior lamina structure is an important landmark in laparoscopic inguinal hernia repair; lateral to the internal ring, no tacks should be placed below the iliopubic track because of the risk of injury to the lateral femoral cutaneous, genitofemoral, and femoral nerves. The pectineal (Cooper’s) ligament refers to the periosteum found along the superior ramus of the pubic bone, posterior to the iliopubic tract (Fig. 29-2, B). The pectineal ligament is an extension of the lacunar (Gimbernat’s) ligament, which connects the inguinal ligament to Cooper’s ligament near their insertion site at the pubic tubercle. Cooper’s ligament is frequently used for medial fixation of the mesh in a laparoscopic hernia repair.
Laparoscopic Inguinal Hernia Repair
Key Anatomic Concepts for Laparoscopic Repair
Inguinal Ligament versus Ileopubic Tract
Pectineal Ligament
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine