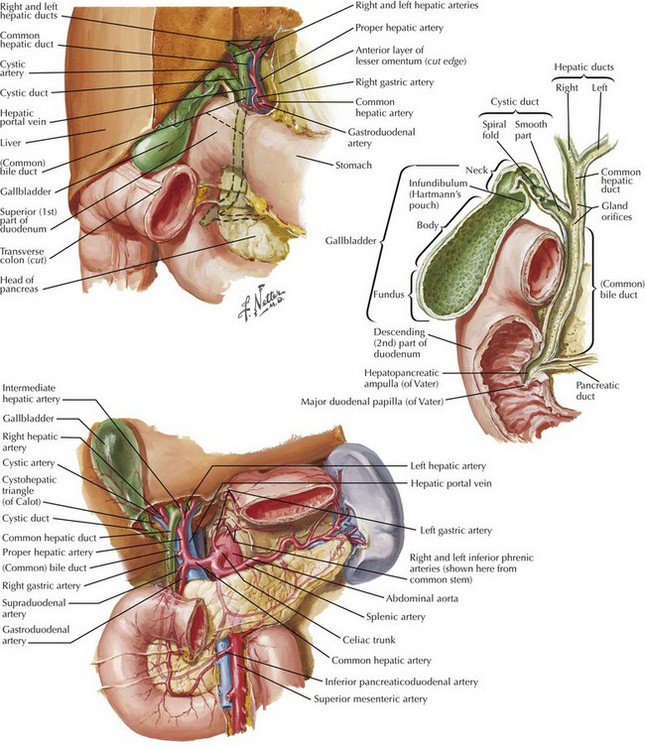
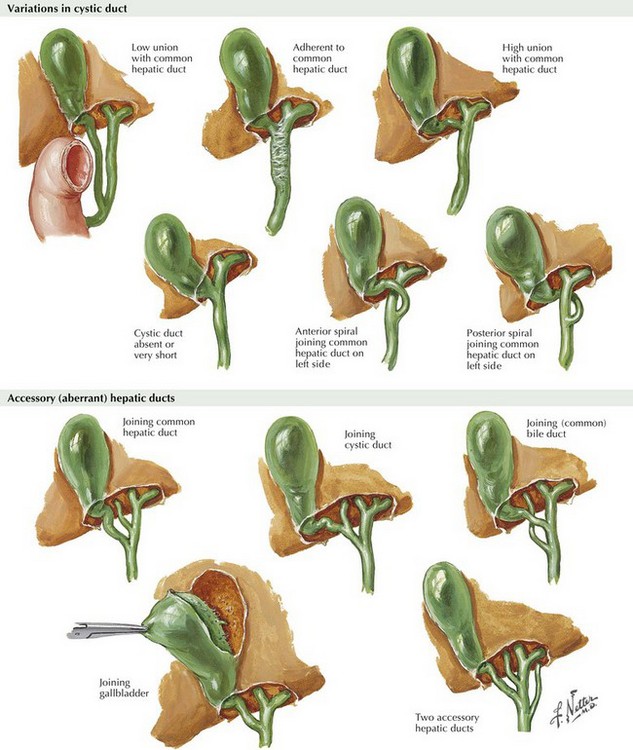
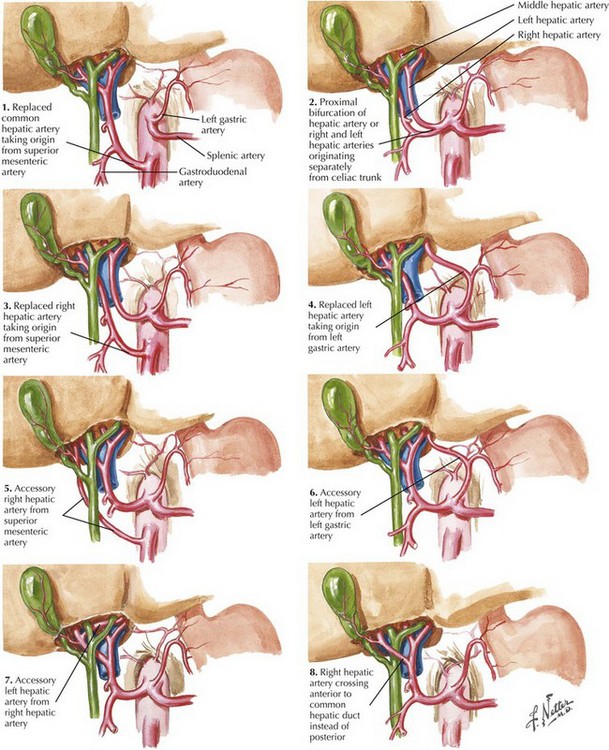
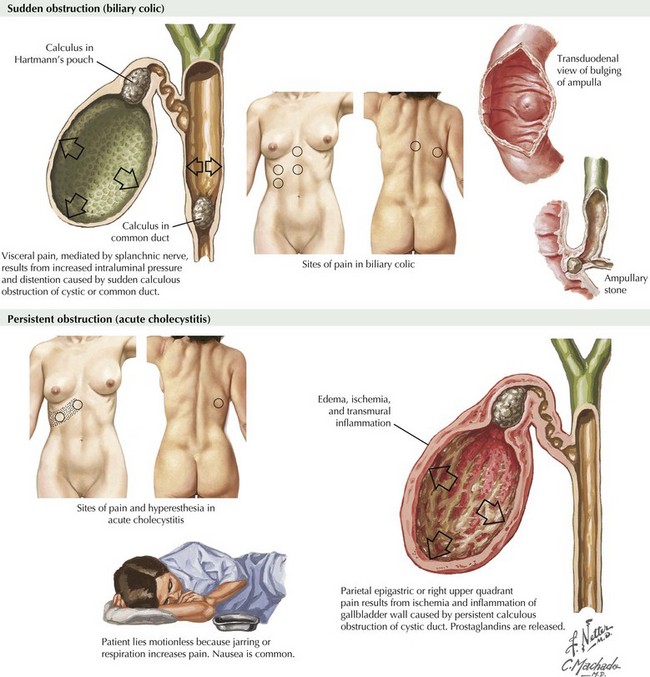
Chapter 12 The gallbladder is an ovoid bag located in the gallbladder fossae of the liver capable of storing up to 50 mL of bile. The gallbladder has a fundus, body, and infundibulum, and it continues by the cystic duct to join the common hepatic duct (CHD) and form the common bile duct (CBD) (Fig. 12-1). The right hepatic artery passes behind the CHD, where the cystic artery originates, and reaches the gallbladder at the cystic node level. This represents the most common anatomic variation but is present in only 50% to 70% of patients. The surgeon must be aware of all anatomic variations of the biliary tree and hepatic artery to avoid injury to the CBD and vascular structures (Figs. 12-2 and 12-3). Although more than 60% of adults older than 60 have gallstones in Western countries, only 20% become symptomatic. The hallmark of symptomatic gallstone disease is abdominal pain, usually in the right upper quadrant (RUQ), with radiation to the back, right shoulder, or epigastrium (Fig. 12-4). Pain classically occurs 30 minutes to 2 hours after the ingestion of a fatty meal and varies in severity. Pain typically is not constant and may be associated with nausea and vomiting. This presentation as biliary colic could progress to an acute inflammatory state promoted by the impaction of a stone in the neck of the gallbladder (see Fig. 12-1). Patients with acute cholecystitis have constant RUQ pain, tenderness at deep palpation (a surrogate of Murphy sign), hyperthermia, and elevated white blood cell count (Fig. 12-4). The stone may pass to the CBD, causing obstruction and development of jaundice. A patient with RUQ pain, fever, leukocytosis, and jaundice, with or without mental changes and hemodynamic compromise, has cholangitis, a true surgical emergency. Other stones produce distal obstruction of the CBD and pancreatic duct, causing an acute episode of pancreatitis. However, most stones that reach the CBD pass into the duodenum, to be passed without consequence.
Laparoscopic and Open Cholecystectomy

Gallbladder Anatomy
Symptomatic Gallstones: Clinical Manifestations
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


