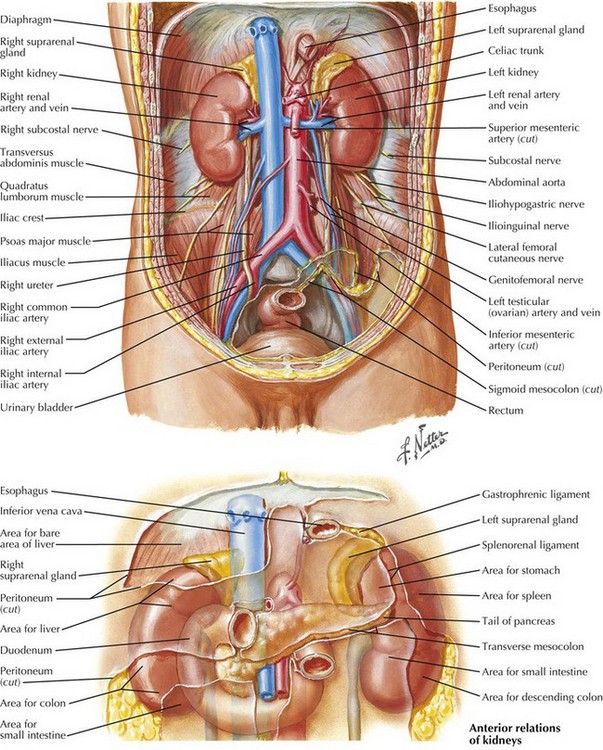
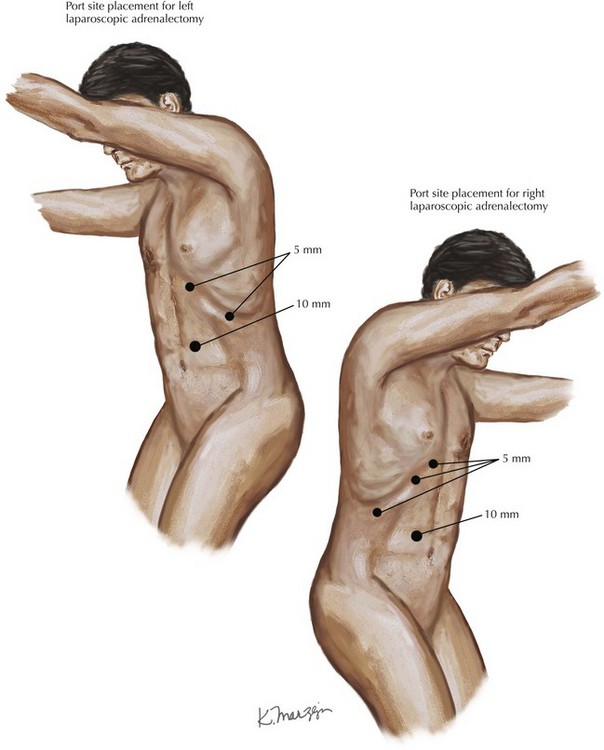
Chapter 4 The adrenal glands reside in the retroperitoneum just above the kidneys (Fig. 4-1). Histologically, the adrenal glands are divided into an outer cortex comprising three layers—zona glomerulosa, zona fasciculata, and zona reticularis—and an inner medulla (Fig. 4-2). These histologic layers correspond to various hormones produced by the adrenal glands. FIGURE 4–2 Histology of adrenal glands. 1. Functional tumors based on excessive hormone production: hyperaldosteronism or Conn syndrome, hypercortisolism or Cushing syndrome, sex hormone–producing tumors, or pheochromocytomas, which lead to excess catecholamine production. 2. Tumors suspicious for malignancy: primary adrenocortical cancer (ACC) or adrenal metastases. 3. Tumors that initially do not meet criteria for categories 1 or 2 but continue to increase in size and volume on interval radiographic follow-up at a rate concerning for a malignant process, or become hypersecretory on repeat laboratory testing. To begin the transabdominal laparoscopic approach, the patient is positioned in the lateral decubitus position to allow gravity to assist with the dissection. A patient requiring right adrenalectomy is placed into a left lateral decubitus position in a jackknife position. Four laparoscopic ports are used, with a 10- to 12-mm port along the lateral border of the right rectus muscle at approximately the level of the umbilicus for the camera and three 5-mm ports along the costal margin. The port closest to the xiphoid process is used for a liver retractor, and two working ports are used for the operative dissection. For left adrenalectomy, the patient is reversed into the right lateral decubitus position, and because there is no need for retraction of the liver, three ports can be triangulated for the operative procedure (Fig. 4-3).
Laparoscopic Adrenalectomy
Introduction
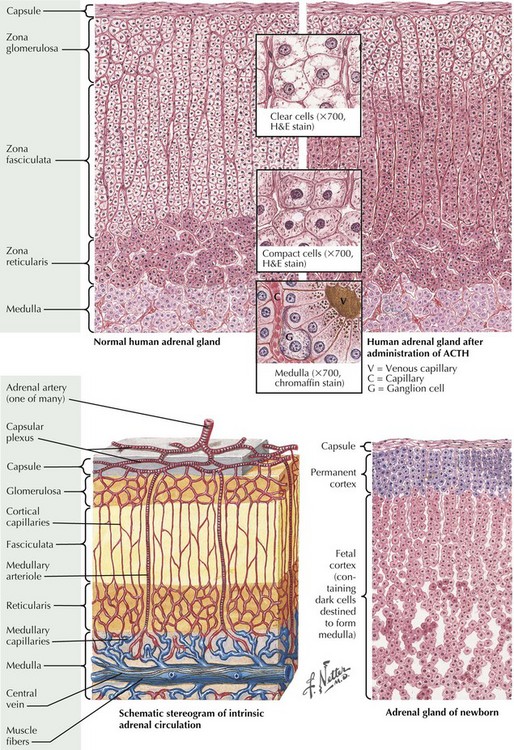
ACTH, Adrenocorticotropic hormone; H&E, hematoxylin and eosin.
Surgical Principles
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine