Patient Story
A 55-year-old woman presents with severe pain in the right flank. The pain began suddenly after supper and increased dramatically over the next hour. Urinalysis shows blood but no signs of infection. Abdominal x-ray reveals bilateral renal stones (Figure 68-1). A noncontrast CT scan confirms multiple bilateral renal stones, with an obstructing right distal ureteral stone and enlargement of the right kidney (Figure 68-2). She is subsequently found to have hyperparathyroidism, which is the cause of her multiple stones.
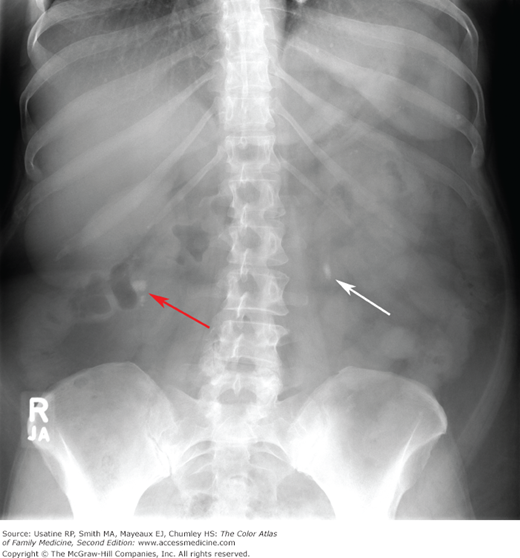
Figure 68-2
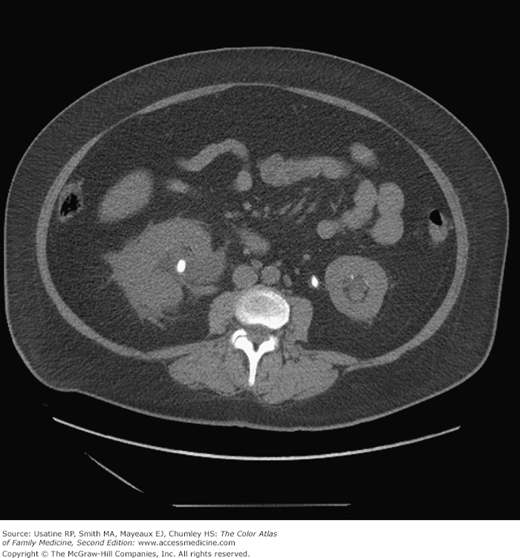
Noncontrast CT of the abdomen and pelvis of the same woman showing several of the stones seen in Figure 68-1, including a nonobstructing stone in the interpolar region of the right kidney. Because the right ureter is obstructed by a distal stone (not visible on this image), the right kidney is enlarged, with collecting system dilation and perinephric stranding. The large left proximal ureteral stone seen in this image is only partially obstructing, causing mild dilation in the left kidney collecting system. Several small stones are visible in the left kidney, and the left kidney is somewhat atrophied from chronic obstruction. (Courtesy of Karl T. Rew, MD)
Introduction
Synonyms
Epidemiology
- The prevalence of kidney stones is increasing in the United States.1 More than 5% of adults have kidney stone disease, with a lifetime risk of 13% for men and 7% for women.
- Men between the ages of 40 and 60 years have the highest risk of stones; for women, the risk peaks in their 50s.2
- African Americans have a lower rate of kidney stones than white Americans.1
- Calcium oxalate and calcium phosphate stones are the most common, occurring in 75% to 85% of patients. Struvite (magnesium ammonium phosphate) stones occur in 5% of cases. Uric acid stones occur in 5% to 10% of patients and cystine stones occur in 1% of cases. Other types of stones are less common.3
- Calcium stones are more common in men than in women (ratio 2:1), whereas struvite stones are more common in women than in men (ratio 3:1).3
Etiology and Pathophysiology
- Kidney stones form when there is supersaturation of otherwise soluble materials, usually from increased excretion of these compounds or dehydration. Urine pH is a factor in stone formation because urinary phosphate increases in alkaline urine, whereas uric acid predominates in acidic urine (pH <5.5). Higher urine citrate can decrease stone formation.
- Struvite stones are caused by infection with urea-splitting bacteria, mainly Proteus.
- Uric acid stones form in patients with gout or hyperuricemia caused by other causes, including myeloproliferative disorders, chemotherapy, and Lesch-Nyhan syndrome.
- Cystine stones occur in patients with an inherited defect of dibasic amino acid transport.
- Struvite, cystine, and uric acid stones can grow large, filling the renal pelvis and extending into the calyces to form staghorn calculi Figure 68-3.

Risk Factors
Infections, genetic defects, and certain drugs can increase the risk of stones, but most stones are idiopathic. Risk factors vary with type of stone, as follows:
- Calcium stones are more likely in patients who are obese4 and in those with diets higher in animal protein, salt, and oxalate-containing foods. Contrary to popular belief, calcium in the diet does not lead to calcium stones; in fact, calcium supplementation can prevent calcium stones by trapping oxalate in the GI tract.
- Patients with poor urinary drainage or indwelling catheters are at risk for Proteus urinary tract infections and struvite stones.
- Uric acid stones are associated with acidic urine, which is more common in obese patients with metabolic syndrome and insulin resistance, and in patients with chronic diarrhea.
Diagnosis
- Kidney stones are often asymptomatic. Stone passage into the ureter usually causes pain and hematuria. The pain of renal colic typically begins suddenly in the ipsilateral flank or abdomen and progresses in waves, gradually increasing in intensity over the next 20 to 60 minutes. As the stone moves downward, pain may be felt in the ipsilateral groin, testis, or vulva.
- Obstructing stones cause hydronephrosis, with an associated constant dull flank pain. Stones in the bladder may cause frequency, urgency, dysuria, or recurrent urinary tract infections.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


