33
CHAPTER OUTLINE
■ WORLDWIDE PREVALENCE OF PSYCHOACTIVE SUBSTANCE USE
■ HISTORICAL SYNOPSIS OF INTERNATIONAL DRUG TREATIES
■ SELECTED ACTIVITIES OF THE UNITED NATIONS OFFICE ON DRUGS AND CRIME
■ SELECTED ACTIVITIES OF THE WORLD HEALTH ORGANIZATION RELATED TO ADDICTION MEDICINE
■ THE EVOLVING ROLE OF INTERNATIONAL MEDICAL ASSOCIATIONS
Historically, international efforts to control use of psychoactive substances have focused on reducing the worldwide supply. International efforts to decrease the demand for drugs are more recent and are gaining momentum. This chapter will focus on major international endeavors: The first two sections will describe the relevant activities under the umbrella of the United Nations: the World Health Organization (WHO) and the United Nations Office of Drug Control (UNODC). The third part describes the mostly volunteer efforts of physicians to develop international networks to address the public health aspects of the use of drugs. These collaborations have resulted in a number of international medical organizations committed to demand reduction, including the World Medical Association, the World Psychiatric Association (WPA), and the International Society of Addiction Medicine (ISAM).
WORLDWIDE PREVALENCE OF PSYCHOACTIVE SUBSTANCE USE
Worldwide psychoactive substance use is highly prevalent, and large segments of the world population are exposed to the effects of dependence-producing substances. Alcohol is the most widely used psychoactive substance worldwide, and about 2.5 billion people use alcohol beverages around the world or approximately 55% of the world’s adult population (1). Currently, more than 1 billion people in the world, or 22% of the world’s adult population (aged 15 years and over) are estimated to be current tobacco smokers (2), and around 230 million people, or 5% of the world’s adult population, are estimated to have used illicit drugs at least once in 2010 (3). Significant proportions of populations repeatedly exposed to such dependence-producing substances as alcohol, tobacco, or drugs develop substance use disorders. According to the WHO estimates, in 2000, the number of people with alcohol dependence or harmful use of alcohol worldwide reached 76.4 million, and the number of people with drug use disorders was 15.3 million (4).
The UNODC’s World Drug Report 2012 estimates the total number of drug users as 230 million people. Cannabis represents the first, and amphetamine-type stimulants, or ATS, the second most widely used classes of substances, followed by “ecstasy,” opioids, and cocaine. UNODC estimates indicate that 27 million people, equivalent to 0.6% of the world population aged 15 to 64, are “problem” drug users (3) (Fig. 33-1).
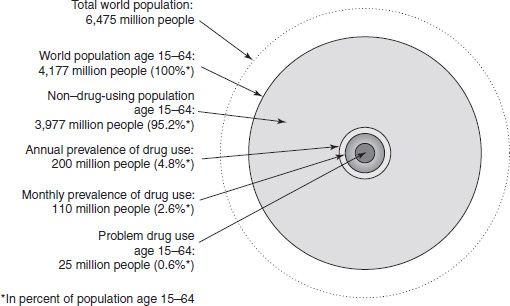
FIGURE 33-1 Illegal drug use at the global level (2005/2006). (Reprinted from World Drug Report, UNODC, 2007.)
The reports to the Commission on Narcotic Drugs on the world situation with regard to drug abuse (5) are based on the opinion of national experts as reported by the member states in the Annual Reports Questionnaire (6). The 2008 report provided an overview of trends in consumption of the main types of illicit drugs from 1998 to 2006 and contributed to the global evaluation of progress toward the achievement of the United Nations General Assembly Special Session (UNGASS) goals set in 1998 (5). The available information suggests that the consumption of opioids and cocaine is stabilizing or decreasing particularly in high-consumption countries (cocaine in North America and heroin in Western and Central Europe, in particular), and the prevalence of heroin injection remains highest in Central Asian and Eastern European countries. Increases in the use of ATS are reported to be tapering off as consumption tends to stabilize or even decrease in Western and Central Europe, East and Southeast Asia, North America, and Oceania. In contrast, cannabis consumption remains globally widespread, as experimentation among youth continues to increase.
In the last 25 years, one of the most visible negative consequences of drug dependence has been human immunodeficiency virus and acquired immunodeficiency syndrome (HIV/AIDS), and it is estimated that more than 10% of all HIV infections worldwide are due to the use of contaminated drug-injecting equipment. If sub-Saharan Africa and the Caribbean are excluded, this rate of injecting drug users rises even to 30% to 40% among those with HIV infection. Data on the size of the injection drug user (IDU) population from 130 countries indicate that there are 13.1 million IDUs worldwide. It also indicates that sharing of contaminated injection equipment is a major route of HIV transmission in many regions, including Eastern Europe; Central, South, and South East Asia; and some countries in Latin America (7).
HISTORICAL SYNOPSIS OF INTERNATIONAL DRUG TREATIES
International drug treaties concluded between 1912 and 1988 provide the legal basis for the present international drug control system aimed at reducing the supply of and demand for illicit narcotic drugs and psychotropic substances. The three major international drug control treaties are complementary and aim at ensuring the availability of narcotic and psychotropic substances for medical and scientific purposes while preventing their diversion into illicit channels, with a view of reducing human suffering and protecting the public health and welfare (8–10).
Particularly relevant to addiction medicine, the conventions specify that signatory countries take all practicable measures for the prevention of abuse of drugs and for the early identification, treatment, education, aftercare, rehabilitation, and social reintegration of the persons involved, including interventions to counteract the social and health consequences of drug abuse. They also require parties to promote the training of personnel involved in delivering such interventions and to facilitate an understanding of the problems of drug abuse among professionals and the general public.
Further clarifying such provisions in the conventions, the International Narcotics Control Board (INCB), in its 2003 report, noted that “Governments needed to adopt measures that may decrease the sharing of hypodermic needles among injecting drug abusers in order to limit the spread of HIV/AIDS.” At the same time, the INCB stressed that such measures should not promote and/or facilitate drug abuse. The same report also observes that “many Governments have opted in favour of drug substitution and maintenance treatment” and that “the implementation of this treatment does not constitute any breach of treaty provisions, whatever substance may be used for such treatment in line with established national sound medical practice” (6).
The conventions further state that when drug abusers have committed drug offences, countries may provide drug treatment, education, aftercare, rehabilitation, and social reintegration either as an alternative or as an addition to conviction or punishment. Such bridges between the criminal justice system and the treatment system may be established at different stages of the criminal process, including the prosecution stage or at the stage of enforcement of a prison sentence.
SELECTED ACTIVITIES OF THE UNITED NATIONS OFFICE ON DRUGS AND CRIME
The United Nations has had drug control functions since its inception, having inherited them from the League of Nations to provide leadership for international drug control efforts. In response to the various mandates reflected under the three major international drug control treaties, work on demand reduction is an integral part of the activities of the UNODC. This important area of work was given further impetus by the special United Nations session in 1998 and thereafter through the adoption of the Political Declaration, the Declaration on the Guiding Principles of Demand Reduction, and the Action Plan for its implementation, which provide focus for the UNODC’s work in providing assistance to member states toward the goal of achieving significant and measurable results in the field of demand reduction by the year 2008. The UNODC’s program of work aims specifically at improving national and global information systems for reporting on activities for the reduction of demand for illicit drugs, sharing of information on best practices, and supporting member states seeking expertise in developing their own strategies and activities for the reduction of demand for illicit drugs (11).
Progress toward Reaching a Balance between Supply and Demand Reduction
As reported by member states to the UNODC through the Biennial Reports Questionnaire, despite the size of the problem and the enormous costs related to drug abuse, in many countries, specialized services are not available or, if present, are not accessible. Although treatment and rehabilitation interventions are being expanded, they are still well below the amount and quality that is needed. For instance, opioid dependence detoxification remains the most common reported approach despite evidence of its lack of effectiveness as a stand-alone intervention, while the intervention with the most solid evidence base—pharmacologic maintenance—remains rather infrequently used in most regions. Interventions for reducing the negative health and social consequences of drug abuse have registered a strong increase at the global level and have overtaken treatment and rehabilitation interventions in terms of reported coverage of activities. In some regions, this trend appears to be associated with efforts to prevent the spread of HIV and other infections among IDUs.
UNODC advocates a comprehensive approach including prevention, treatment, and prevention of health and social consequences in line with the evidence base and has recently released a paper highlighting the complementarities of all those measures and calling for a continuum of care in services for drug users (12). In such a continuum, steps are taken to reach out to and engage drug users in prevention, treatment, and care strategies that protect them, their partners, and their families from infectious disease, other health problems, and negative social consequences. Within this model, a wide range of community-based services offer easy access to different target groups, responding to diverse age, gender, and other needs, and encourage entry to social and health care, substance dependence treatment, and rehabilitation. The UNODC-WHO discussion paper on principles of drug dependence treatment (13) notes that interventions and investments in treatment within such a model would be guided by human rights and evidence-based good practice and the high-quality standards that are required to approve pharmacologic or psychosocial interventions in all the other medical disciplines. Community- and prison-based treatment and rehabilitation programs can form part of the same overall treatment system and guarantee the same level of quality. In an international context, such interventions and strategies need to be adapted to the diverse regional, national, and local circumstances, taking into account cultural and economic factors.
Unfortunately, underutilization of such approaches represents a long-standing problem for the field, and those who would most benefit from research advances (community treatment agencies and the clients they serve) have historically been the least likely to be exposed to innovative evidence-based methods. Training of prevention and treatment professionals from early on in their careers and evaluation and feedback on service performance are essential to improve knowledge and disseminate evidence-based methodologies worldwide.
Key Initiatives and Tools: Youthnet and Treatnet—Knowledge Transfer Initiatives
With the aim of supporting countries in achieving significant results in reducing demand for drugs by 2008, the UNODC supports the Global Youth Network (www.unodc.org/youthnet) for the prevention of drug abuse. Regional networks reach with information, resources, and training more than 500 youth groups around the world and provide grants to some 125 organizations to implement comprehensive drug abuse prevention activities. Unfortunately, many prevention programs around the world, while well intentioned, implement activities that do not have the backing of scientific evidence (e.g., life skills education and family skills training programs) (14–17).
The UNODC aims at positioning drug dependence treatment as a key public health and development intervention. Its work, therefore, will increasingly focus on raising awareness about addiction as a treatable, multifactorial disease and about the need to improve the quality and coverage of drug treatment services around the world. Treatnet, the “International Network of Drug Dependence Treatment and Rehabilitation Resource Centres” (www.unodc.org/treatnet), aims to improve the provision of diversified and effective drug treatment and rehabilitation services, including the support to HIV/AIDS prevention and care, in all regions. The Network’s members included, in its first stage from 2005 to 2007, 20 drug dependence treatment and rehabilitation resource centers, a training consortium led by University of California, Los Angeles Integrated Substance Abuse Programs and other partners. In its second phase, starting in 2008, it evolved into regional networks and involved in addition to treatment centers universities and governmental institutions in charge of treatment and rehabilitation. The work of the network has focused on and developed good-practice documents on four key topics: community-based treatment (18), treatment in prison settings (19), treatment and HIV/AIDS prevention and care (20), and sustained recovery management (21). Through Treatnet, the UNODC has developed a comprehensive training package on treatment and rehabilitation (22) and training of trainers in 14 countries who in turn have trained more than 1,000 physicians, psychologists, counselors, social workers, nurses, and other professionals. The trainers have assessed very positively the comprehensive training package and, in many cases, have continued to disseminate the training well beyond the UNODC’s supported program.
The UNODC’s Global Assessment Programme (GAP) on Drug Abuse aims at improving the local and global knowledge of the drug abuse situation and at building the capacity to design and implement effective responses to the drug abuse problem through establishing drug epidemio-logic surveillance and monitoring and evaluation systems for drug demand reduction. The GAP has been operational since 2000 in several regions of the world and is currently providing training and technical assistance in the Russian Federation, Central Asia, West and Central Africa, and the Middle East and North Africa.
The UNODC is a cosponsor of the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the lead agency for HIV/AIDS prevention and care among IDUs and in prison settings. The UNODC is also responsible for assisting countries in implementing large-scale and wide-ranging interventions to prevent HIV infections and providing care and support to people living with HIV/AIDS. The UNODC advocates that evidence-informed, comprehensive, and large-scale interventions for IDUs be an integral part of national HIV/AIDS framework.
SELECTED ACTIVITIES OF THE WORLD HEALTH ORGANIZATION RELATED TO ADDICTION MEDICINE
The WHO, as the UN specialized agency on health, is concerned with all psychoactive substances irrespective of their legal status in the international treaties and advocates for a public health approach to problems related to tobacco, alcohol, illicit drugs, and other psychoactive substance use.
Global Burden of Disease Attributable to Psychoactive Substance Use
Better understanding of the impact of psychoactive substance use on the population health resulted from the influential Global Burden of Disease (GBD) study, a groundbreaking international effort to quantify the disease burden of different diseases and health conditions using mortality estimates and the estimates of disease burden expressed in disability-adjusted life years (DALYs) lost (23). In 2000, the WHO published its World Health Report with figures of comparative contribution of different risk factors to the disease burden in different parts of the world (24). Tobacco, alcohol, and illicit drug use were among the top leading preventable risk factors to health, responsible for 8.9% of the total disease burden if taken together (25).
The public health impact of psychoactive substance use is not limited to substance use disorders, and significant harm comes from acute intoxication, risks associated with the form of administration, or toxic effects of a substance (25). The proportion of the burden attributable to substance use disorders in the overall burden attributable to psychoactive substances is at least moderate. For example, according to the WHO estimates for 2002, alcohol use disorders are responsible for 1.4% of the total global disease burden, whereas drug use disorders account for 0.5%, compared to a much higher contribution of alcohol and drug use as risk factors to the global disease burden (illustrated in Table 33-1). At the same time, alcohol and drug use disorders (harmful use/ abuse and dependence) are the second largest contributor— after unipolar depressive disorders—to the global disease burden among “neuropsychiatric disorders,” which are responsible for 13% of the total global disease burden in 2002 (26). These data have important policy implications: From a public health perspective, effective reduction of the disease burden attributable to psychoactive substance use cannot be achieved just by treatment of substance dependence and implies a broader spectrum of effective policies. These include reducing exposure to psychoactive substances, limiting their availability in populations, and specific targeted interventions aimed at reducing the harm associated with continued use of psychoactive substances.
TABLE 33-1 PERCENTAGE OF TOTAL GLOBAL MORTALITY AND DALYs ATTRIBUTABLE TO TOBACCO, ALCOHOL, AND ILLICIT DRUGS, 2000
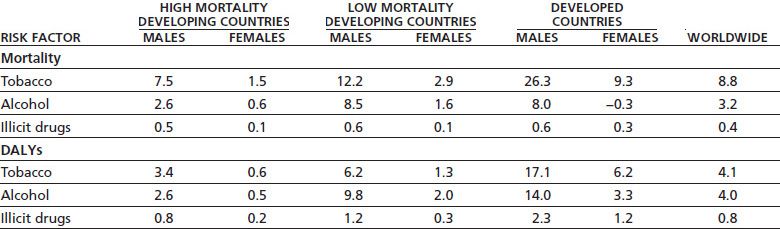
From World Health Organization. Neuroscience of psychoactive substance use and dependence. Geneva, Switzerland: World Health Organization, 2004.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


