Inflammatory Pseudotumor
Francisco Vega, MD, PhD
Key Facts
Terminology
Inflammatory reaction with multifactorial pathogenesis
Infectious etiologies account for subset of cases
Clinical Issues
Young adults with fever and constitutional symptoms
Localized or involving several lymph node groups
Excellent prognosis
Microscopic Pathology
Initially centered on hilum, trabeculae, and capsule of lymph nodes
Fascicles and whorls of spindle cells
Vascular proliferation
Polymorphic inflammatory infiltrate
Plasma cells often numerous
Pronounced follicular hyperplasia occurs in syphilitic lymphadenitis
Ancillary Tests
Spindle cells positive for markers of fibroblastic reticulum cells &/or histiocytes
Lack of chromosomal translocations involving ALK or lack of ALK1 protein expression
No evidence of monoclonality
Top Differential Diagnoses
Inflammatory myofibroblastic tumor
Kaposi sarcoma
Mycobacterial spindle cell pseudotumor
Follicular dendritic cell sarcoma
Hemorrhagic spindle cell tumor with amianthoid fibers (palisaded myofibroblastoma)
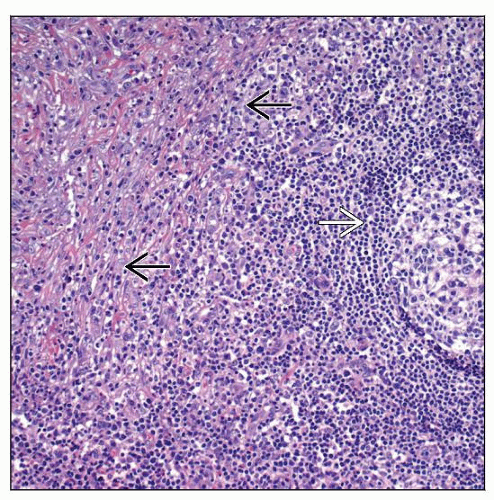 IPT focally involving mediastinal lymph node is characterized by spindle cell proliferation, slight sclerosis, and a polymorphic inflammatory infiltrate  . Note residual lymphoid follicle . Note residual lymphoid follicle  . . |
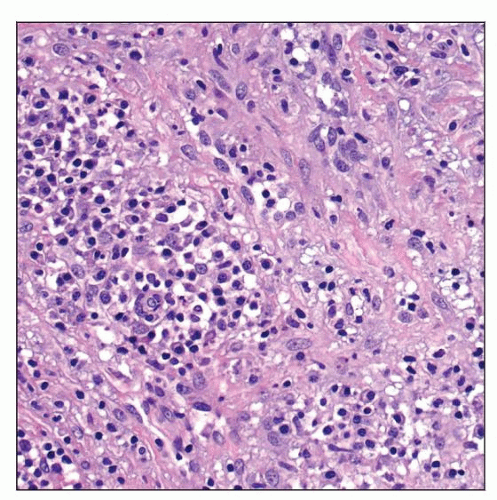 IPT of lymph node is composed of spindle cells, histiocytes, and clusters of plasma cells and small lymphocytes. |
TERMINOLOGY
Abbreviations
Inflammatory pseudotumor (IPT)
Synonyms
Plasma cell granuloma
Definitions
Inflammatory reaction involving lymph node characterized by proliferation of spindled cells associated with small vessels and inflammation
ETIOLOGY/PATHOGENESIS
Infectious Agents
Etiology is most likely multifactorial but subset appears related to infectious agents
Treponema pallidum
Pseudomonas veronii
Pseudomomas psittaci
Subset of IPT cases are associated with rheumatoid arthritis
For many cases etiology is unknown; EBV unlikely to be involved
CLINICAL ISSUES
Presentation
No sex predilection
Broad age range; median: 4th decade
Fever &/or constitutional symptoms
Anemia, elevated erythrocyte sedimentation rate, hypergammaglobulinemia
Localized or involving several lymph node groups
Cervical, axillary, mediastinal, retroperitoneal, and inguinal lymph nodes
Treatment
Surgical excision of lesion is curative
Prognosis
Excellent; usually self limiting
Relapse in some cases
MACROSCOPIC FEATURES
General Features
Enlarged; rubbery, gray-white cut surface
MICROSCOPIC PATHOLOGY
Histologic Features
Cell proliferation initially centered on fibrous network of lymph node
Hilum, trabeculae, and capsule
Different histologic stages
Stage I: Partial involvement; prominent inflammation
Stage II: More diffuse involvement
Stage III: Dense sclerosis; few inflammatory cells
Fascicles and whorls of spindle cells
Vascular proliferation (small vessels)
Polymorphic inflammatory infiltrate
Plasma cells common and can be numerous
Immunoblasts, small lymphocytes, histiocytes, neutrophils, and occasional eosinophils
Histiocytes can be spindled or round
Vasculitis is frequent
Follicular hyperplasia can be prominent
Suspect spirochete infection as cause
Lack of necrosis, karyorrhexis, or infarction
No cytologic atypia or atypical mitotic figures
ANCILLARY TESTS
Immunohistochemistry
Spindle cells can have immunophenotype of fibroblastic reticulum cells (FRC) or histiocytes
FRC are often
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


