The incidence of marrow involvement, variety of organisms, and frequency of multiple infections have greatly increased in recent years because of the fast-growing population of immunosuppressed patients. International travel has also brought diseases to new countries in significant numbers.
The range of reactive responses in the peripheral blood and bone marrow is limited, and morphologic findings are often nonspecific. Positive identification of the organism, specific serologic reactions, and’or molecular methods are typically required for definitive diagnosis. Following are brief descriptions of the peripheral blood and bone marrow findings in response to various infectious agents (Table 13.1).
BACTERIA
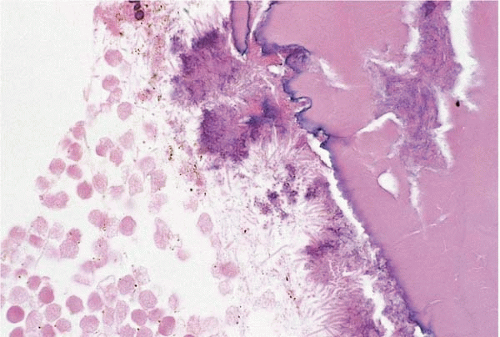
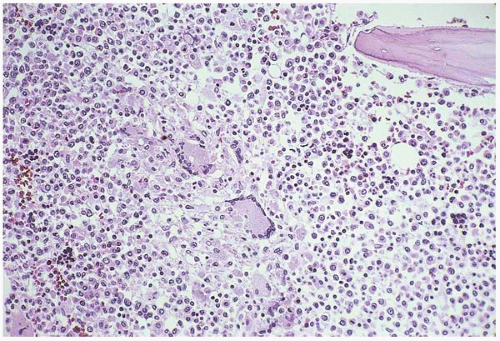
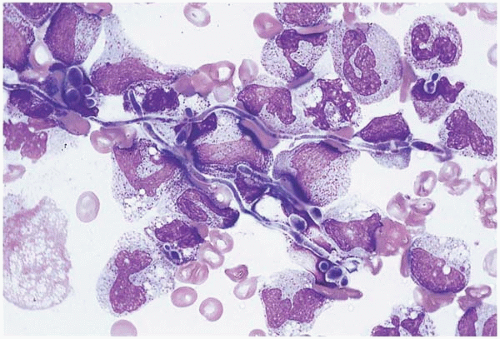
Actinomyces spp. may invade the bone marrow, especially marrow contained within the facial bones. Bone marrow necrosis and clusters of organisms may be found (Fig. 13.1).
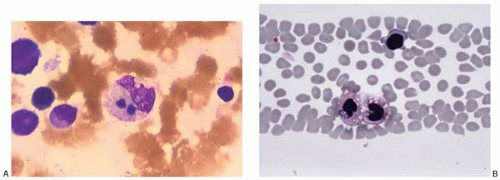
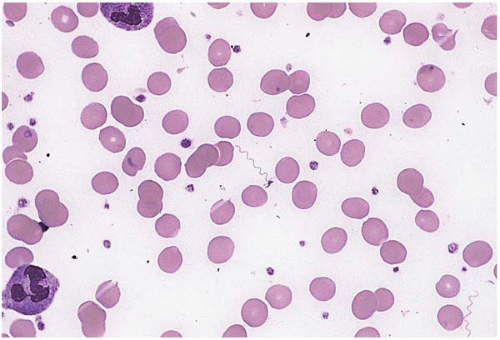
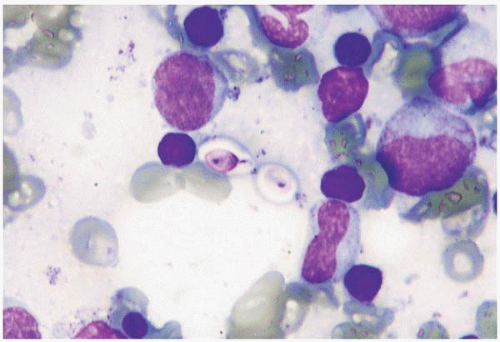
Anaplasma phagocytophilum, a tick-borne rickettsial pathogen, is an obligate intracellular bacterium and the agent of human granulocytic anaplasmosis (formerly human granulocytic ehrlichiosis) (Fig. 13.2) (1,2). Patients present with fever and nonspecific systemic symptoms. Laboratory studies usually show lymphopenia and thrombocytopenia. Peripheral blood and bone marrow aspirate smears may show cytoplasmic inclusions in mature granulocytes. The inclusions are aggregates (morulae) of intracellular organisms. Histologic sections of the bone marrow show myeloid and megakaryocytic hyperplasia or, less often, trilineal hypoplasia. Other findings include reactive histiocytosis, perivascular lymphohistiocytic aggregates, and granulomas, with or without fibrin-ring morphology. Hemophagocytic syndrome has been reported.
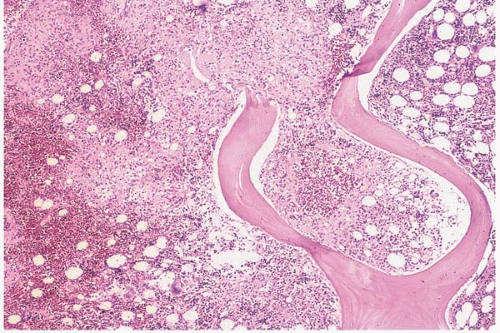
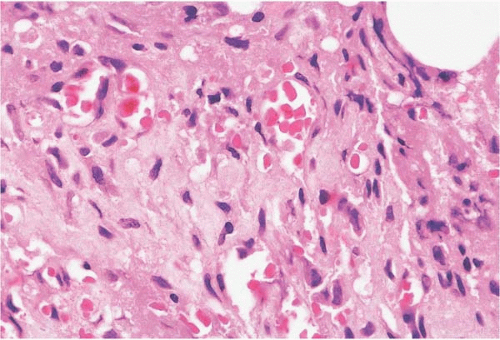
Bartonella spp. are the infectious agents of cat-scratch disease in the immunocompetent host and systemic bartonellosis in the immunosuppressed patient (Figs. 13.3 and 13.4) (3, 4, 5, 6). Marrow sections may show bacillary angiomatosis or granulomas and lymphohistiocytic aggregates without vascular proliferation. Hemophagocytic syndrome has been reported. The diagnosis is made by detection of small, intracellular, gram-negative, and silver-positive bacilli and identification of Bartonella spp. by immunohistochemical and molecular studies. The differential diagnosis of bacillary angiomatosis includes Kaposi sarcoma.
Bordetella spp. cause whooping cough and marked lymphocytosis, primarily in infants and children (7, 8, 9, 10, 11). The white blood cell count may increase to more than 100 × 109‘L, consisting predominantly of lymphocytes. Neutrophils, monocytes, T-cells, B-cells, and natural killer (NK) cell counts are all increased. L-selectin is a surface molecule mediating extravasation of lymphocytes into tissues and homing of lymphocytes to lymph nodes. In Bordetella pertussis infection, L-selectin expression is decreased in all leukocyte groups. This appears to account for the presence of leukocytosis, especially lymphocytosis. The lymphocytes often show convoluted and cleaved nuclear membranes and may resemble blasts. Flow cytometry shows a predominant population of CD3-positive T cells, with a normal CD4:CD8 ratio and no immunophenotypic abnormalities. The differential diagnosis includes acute lymphoblastic leukemia.
Borrelia spp. cause Lyme disease, relapsing fever, and other clinical syndromes (Fig. 13.5) (12, 13, 14, 15, 16). Clinically, borreliosis may mimic malaria. In acute disease, the peripheral blood may show eosinophilia and free-floating spirochetes. The bone marrow may show T-lymphocytosis and epithelioid granulomas, the latter sometimes showing fibrin-ring morphology. The lymphoid infiltrates may resemble malignant lymphoma.
Brucella spp., the agents of brucellosis, may cause disseminated infections with severe microangiopathic hemolytic anemia, especially in children and in immunocompromised patients (17, 18, 19, 20, 21, 22). The peripheral blood often shows thrombocytopenia or pancytopenia. The bone marrow shows erythroid and megakaryocytic hyperplasia, eosinophilia, reactive plasmacytosis, granulomas, and reactive histiocytosis. Hemophagocytic syndrome has been reported.
Burkholderia spp. cause infection in patients with chronic granulomatous disease and immunosuppressed states. No specific peripheral blood or bone marrow findings have been reported, with the exception of hemophagocytic syndrome (23).
TABLE 13.1 Infectious Agents Causing Peripheral Blood and Bone Marrow Changes
Bacteria
Fungi
Viruses
Protozoa
Helminths
Actinomyces spp.
Candida spp.
Adenovirus
Babesia spp.
Brugia spp.
Anaplasma phagocytophilum
Cryptococcus neoformans
BK virus
Leishmania spp.
Mansonella perstans
Coxsackievirus
Microsporidia spp.
Wuchereria bancrofti
Bordetella spp.
Histoplasma capsulatum
Cytomegalovirus
Plasmodium spp.
Bartonella spp.
Dengue virus
Toxocara canis
Borrelia spp.
Paracoccidioides brasiliensis
Echovirus
Toxoplasma gondii
Brucella spp.
Enterovirus
Trypanosoma spp.
Burkholderia spp.
Penicillium marneffei
Epstein-Barr virus
Coxiella burnetii
Pneumocystis jirovecii
Hantavirus
Ehrlichia spp.
Trichosporon spp.
Hepatitis A virus
Escherichia coli
Hepatitis B virus
Klebsiella rhinoscleromatis
Hepatitis C virus
Hepatitis E virus
Leptospira spp.
Herpes simplex virus
Listeria monocytogenes
Human herpesvirus 6
Human herpesvirus 7
Micrococcus spp.
Human herpesvirus 8
Mycobacterium spp.
Human immunodeficiency virus type 1
Neisseria spp.
Orientia tsutsugamushi
Human immunodeficiency virus type 2
Rickettsia conorii
Salmonella typhi
Human T lymphotropic virus I
Shigella spp.
Staphylococcus aureus
Human T lymphotropic virus II
Treponema pallidum
Influenza virus
Tropheryma whippelii
Measles virus
Mumps virus
Parvovirus B19
Rubella virus
SARS virus
Varicella-zoster virus
Figure 13.1Actinomycesinfection, bone marrow biopsy. The bone and hematopoietic tissue are necrotic; clouds (sulfur granules) of bacteria are seen along the bone surface.
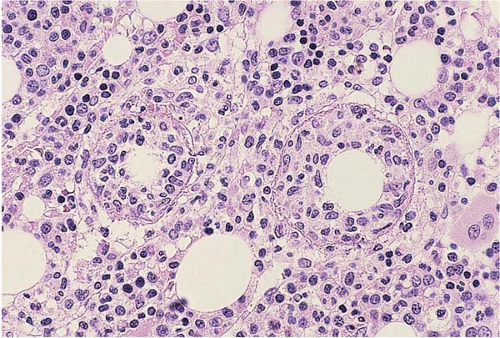
Coxiella burnetii, the agent of Q fever, may be accompanied by cytopenias, hematopoietic hypoplasia, and bone marrow granulomas (Fig. 13.6) (24, 25, 26, 27, 28). The granulomas are composed of a clear central space or vacuole rimmed by fibrin and neutrophils and surrounded by a collar of histiocytes (fibrin-ring granuloma); however, this histologic appearance is not specific for Q fever. Hemophagocytic syndrome has been reported.
Ehrlichia spp. are tick-borne rickettsial pathogens and obligate intracellular bacteria. E. chaffeensis is the agent of human monocytic ehrlichiosis (HME), a more clinically severe disease than human granulocytic anaplasmosis (29, 30, 31, 32, 33, 34, 35, 36). Patients with HME pesent with fever, organ dysfunction, and coagulopathy, and may have a fatal outcome, particularly in immunosuppressed patients. Laboratory studies show lymphopenia and thrombocytopenia. The peripheral blood shows atypical lymphocytes. Peripheral blood and bone marrow aspirate may show cytoplasmic inclusions within neutrophils and histiocytes, rarely within lymphocytes. The inclusions are aggregates (morulae) of intracellular organisms. Histologic sections of the bone marrow may show (in descending order) myeloid and megakaryocytic hyperplasia; granulomas, which may show fibrin-ring morphology; reactive histiocytosis; myeloid hypoplasia; and’or trilineal hypoplasia. E. ewingii is the agent of human ewingii ehrlichiosis, a less severe disease than HME (37). The peripheral blood may show morulae in granulocytes, indistinguishable from those caused by Anaplasma phagocytophilum. E. canis causes a similar nonspecific febrile illness with cytoplasmic inclusions in monocytes (38,39). Bone marrow hypoplasia and hemophagocytic syndrome have been reported.
Figure 13.2Anaplasma phagocytophilum(human granulocytic anaplasmosis), peripheral blood. A morula is present within a neutrophil.
Figure 13.3Bartonellainfection (bacillary angiomatosis) spleen, bone marrow biopsy. The hematopoietic tissue is focally replaced by fibrovascular connective tissue. The differential diagnosis includes Kaposi Sarcoma.
Figure 13.4Bartonellainfection (bacillary angiomatosis) spleen, bone marrow biopsy. The lesion is composed of multiple thin-walled blood vessels separated by connective tissue.
Figure 13.5Borreliainfection (relapsing fever), peripheral blood smear. A spirochete is present, floating in the plasma between red blood cells.
Figure 13.6Coxiellainfection (Q fever), bone marrow biopsy. Fibrin-ring granulomas are present.
Escherichia coli causes infection in patients with a wide variety of underlying pathology. Hemophagocytic syndrome and bone marrow necrosis with gas accumulation have been described in E. coli sepsis (40,41).
Klebsiella rhinoscleromatis is the agent of rhinoscleroma. In disseminated disease, the bone marrow shows proliferation of large histiocytes with bacillus-filled cytoplasm (Mikulicz cells) (42).
Leptospira spp. are spirochetes and the agents of leptospirosis, a disease acquired from rats (43, 44, 45, 46, 47, 48, 49). Patients may be affected at any age and usually present with fever, jaundice, renal failure, and other signs of systemic illness. Laboratory studies usually show anemia and thrombocytopenia, sometimes pancytopenia, and may also show neutrophilia, neutropenia, and immature neutrophils. Leptospirosis has been reported to cause a leukemoid reaction resembling acute myeloid leukemia. The bone marrow may show myeloid hyperplasia, erythroid hypoplasia, reactive plasmacytosis, reactive histiocytosis, and in some cases, trilineal hypoplasia (aplastic anemia). The organisms can be demonstrated within bone marrow histiocytes by silver staining and immunofluorescence. Hemophagocytic syndrome has been reported.
Listeria monocytogenes is an opportunistic pathogen causing listeriosis in patients with constitutional immunodefiency and other immunosuppressed states, monocytopenia, or malignancy (50, 51, 52, 53, 54). Other susceptible populations include neonates, pregnant women, and those older than 65 years of age. The peripheral blood may show lymphopenia. Hemophagocytic syndrome has been reported.
Micrococcus spp. cause no specific peripheral blood or bone marrow findings, but have been reported to cause hemophagocytic syndrome (55).
Mycobacterium bovis (bacille Calmette-Guérin, BCG) may cause disseminated disease in susceptible individuals following either routine vaccination or therapeutic BCG administration (54,56, 57, 58, 59, 60, 61, 62, 63). It has been reported as a presenting sign of severe combined immunodeficiency and other congenital immunodeficiency syndromes, and may also occur after such patients have undergone bone marrow transplantation. Disseminated disease has also been reported in patients with acquired immunodeficiency syndrome, in infants and children without known congenital immunodeficiency, and in patients treated with BCG for bladder carcinoma and malignant melanoma. The peripheral blood may show monocytes filled with micro-organisms, visible with Wright-Giemsa stains as nonstaining, rod-like spaces. Aspirate smears may show Gaucher-like storage histiocytes filled with bacilli. Histologic sections of the bone marrow show well-formed granulomas, loose lymphohistiocytic aggregates, sheets of bacillus-laden histiocytes, or bone marrow necrosis, depending on the degree of antecedent immunosuppression.
Mycobacterium leprae, the agent of leprosy, may become disseminated and involve the bone marrow (64, 65, 66, 67, 68). The peripheral blood often shows anemia of chronic disease. The bone marrow may show megaloblastic erythropoiesis, reactive plasmacytosis, granulomas, and histiocytosis. Acid-fast bacilli may be found both within cells and lying free in the interstitial space. Depending on the stage of disease and level of immunocompetence, bacilli may be scant or numerous. The bone marrow often shows as least a few bacillus-filled histiocytes (known as lepra cells or Virchow cells), plasmacytosis, and sea-blue histiocytosis. In overwhelming disease, numerous bacillus-filled histiocytes are seen, with little or no granulomatous reaction.
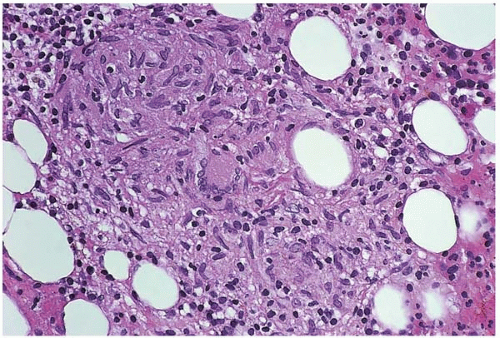
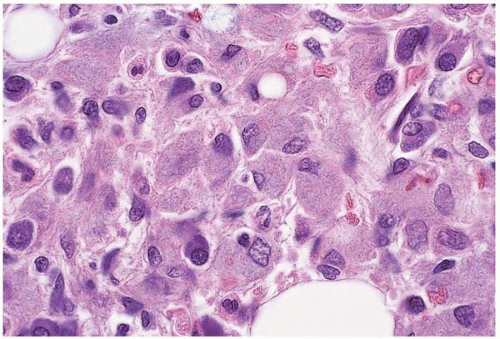
Mycobacterium tuberculosis is an important pathogen, especially in immunosuppressed patients (Fig. 13.7) (4,69, 70, 71, 72). Patients may present with fever of unknown origin and other nonspecific signs and symptoms. The peripheral blood may show a wide variety of findings, with increases or decreases in neutrophils, lymphocytes, monocytes, and platelets. Disseminated disease is accompanied by cytopenias. Depending on the level of immunity, histologic sections of the bone marrow may show granulomas with rare acid-fast bacilli, lymphohistiocytic aggregates with more numerous bacilli, or sheets of bacillus-laden histiocytes. Granulomas may show caseous necrosis. Reactive plasmacytosis may be present. Pure red cell aplasia and hemophagocytic syndrome have been reported.
Figure 13.7Mycobacterium tuberculosisinfection, bone marrow biopsy. A large, well-formed granuloma is present and composed of histiocytes and giant cells.
Figure 13.8Mycobacterium avium-intracellulare complexinfection (atypical tuberculosis), bone marrow aspirate. A histiocyte is present and its cytoplasm is filled and distended by organisms, which are seen as negative (nonstaining) rods.
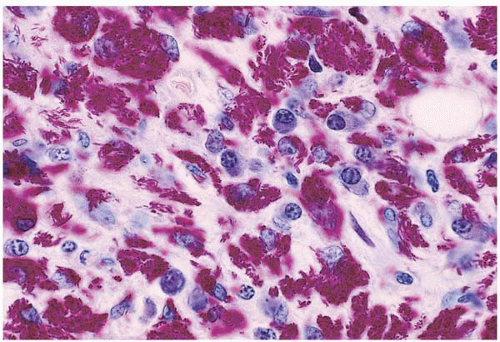
Atypical mycobacteria (those of species other than those discussed above) can cause disseminated infection, usually in immunosuppressed patients (Figs. 13.8, 13.9, 13.10and 13.11) (73, 74, 75, 76). The peripheral blood often shows cytopenias. As in tuberculosis, the degree of tissue reaction in the bone marrow depends on the level of immunosuppression. With relatively intact immunity, well-formed granulomas with few acid-fast bacilli are found. With profound immunosuppression, indistinct lymphohistiocytic aggregates or sheets of bacillusladen histiocytes are found. Hemophagocytic syndrome has been reported.
Mycoplasma pneumoniae is usually considered as a cause of pulmonary disease; however, hematologic complications of infection may occur in the absence of pulmonary findings (77, 78, 79, 80). These include neutrophilia, cold agglutinin-related hemolytic anemia, thrombocytosis, thrombocytopenia, and thrombotic thrombocytopenic purpura. The anemia may be life-threatening. Hemophagocytic syndrome has been described.
Figure 13.9Mycobacterium avium-intracellulare complexinfection (atypical tuberculosis), bone marrow biopsy. A very large, poorly circumscribed granuloma is present that is composed of histiocytes, lymphocytes, and giant cells.
Figure 13.10Mycobacterium avium-intracellulare complexinfection (atypical tuberculosis), bone marrow biopsy. A sheet of bacillus-filled histiocytes is present, without evidence of granuloma formation, in this specimen from a patient infected with human immunodeficiency virus.
Neisseria spp. cause systemic infection, especially in asplenic, hyposplenic, and immunocompromised patients (81,82). The peripheral blood and bone marrow show no specific findings; however, hemophagocytic syndrome has been reported.
Orientia tsutsugamushi (formerly Rickettsia tsutsugamushi), the agent of scrub typhus or tsutsugamushi fever, is acquired from mites (83, 84, 85). Patients present with fever, eschar at the site of the infection, hepatomegaly, cough, and other evidence of systemic infection. The peripheral blood usually shows leukocytosis, lymphocytosis with atypical lymphocytes, and thrombocytopenia. Immunohistochemical evidence of the organisms has been demonstrated in circulating mononuclear cells. CD8-positive T cells are increased, and CD4-positive T cell are reduced, producing a reversed CD4:CD8 ratio. Hemophagocytic syndrome has been reported.
Figure 13.11Mycobacterium avium-intracellulare complexinfection (atypical tuberculosis), bone marrow biopsy. A sheet histiocytes shows massive infection with acid-fast bacilli in this specimen from a patient infected with human immunodeficiency virus.
Rickettsia conorii is the tick-borne agent of Mediterranean spotted fever (boutonneuse fever) (86, 87, 88, 89). Patients present with an eschar at the site of the tick bite, fever, and rash. The peripheral blood shows leukocytosis or leukopenia, thrombocytopenia, and’or pancytopenia. A reversed ratio of CD4 to CD8 T cells has been described. Infection may induce hemolysis in patients deficient for glucose-6-phosphate dehydrogenase. In one case, the bone marrow was hypercellular and contained granulomas. Fibin-ring granulomas have been described in hepatic biopsies, and it is likely that these also occur in the bone marrow, although they have not been specifically reported.
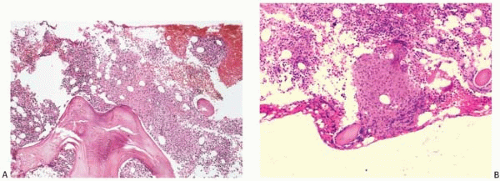
Salmonella typhi is the agent of typhoid fever (Fig. 13.12) (90, 91, 92, 93, 94, 95). Peripheral blood findings in typhoid fever include anemia, neutropenia, eosinopenia, lymphopenia, monocytopenia, and thrombocytopenia. Pancytopenia may be present. In acute disease, the bone marrow may show granulocytic hyperplasia, myeloid maturation arrest, decreased erythroid precursors and megakaryocytes, reactive histiocytosis with increased hemophagocytic activity, and focal necrosis. Frank hemophagocytic syndrome has been reported. Chronic disease is characterized by bone marrow granulomas. Granulomas have also been reported with S. paratyphi.
Shigella spp. cause dysentery. The peripheral blood may show pancytopenia, and the bone marrow may show hematopoietic hypoplasia (96,97).
Staphylococcus aureus infection causes no specific peripheral blood findings. It has been reported to cause osteomyelitis following bone marrow aspiration. In systemic infection, it has been reported to cause pancytopenia with bone marrow hypocellularity and hemophagocytic syndrome (98, 99, 100, 101). S. epidermidis infection has been reported to cause focal bone marrow necrosis (102).
Figure 13.12Salmonella typhiinfection (typhoid fever), bone marrow biopsy. A well-formed granuloma is present in this specimen from a patient who had traveled and lived in Mexico. (A) Low power. (B) High power.
Treponema pallidum, the etiologic agent of syphilis, can cause hematopoietic complications in the fetus and infant (103, 104, 105, 106). These include fetal hydrops, anemia, peripheral monocytosis, extramedullary hematopoiesis, and hemophagocytic syndrome.
Tropheryma whippelii, the agent of Whipple disease, may cause disseminated infection and anemia (107, 108, 109, 110, 111). The bone marrow may show granulomas. Monocytes and macrophages may be increased and filled with periodic acid-Schiff-positive bacilli.
FUNGI
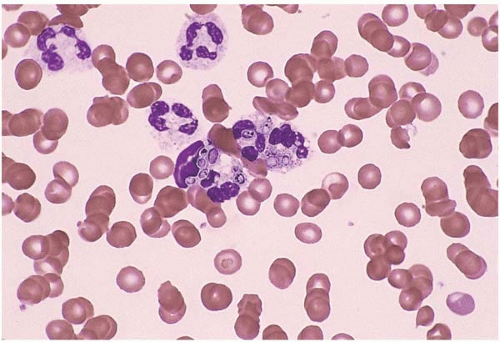
Candida spp. can cause systemic disease, particularly in immunosuppressed patients (Fig. 13.13) (112, 113, 114, 115, 116). The peripheral blood may show intracellular organisms in phagocytic cells and extracellular organisms in the plasma. Both yeast forms and pseudohyphae may be found. A leukemia-like reaction has been reported. Bone marrow granulomas are rarely seen. Leukemoid reaction and hemophagocytic syndrome have been reported.
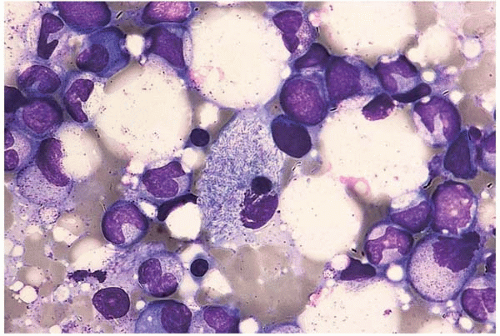
Cryptococcus neoformans may infect the bone marrow in immunosuppressed patients, especially those with reduced T-cell-mediated immunity (Figs. 13.14 and 13.15) (117, 118, 119, 120, 121). Peripheral blood and bone marrow aspirate smears may show ingested organisms in phagocytic cells. Depending on the level of immunosuppression, histologic sections of the bone marrow may show granulomas, lymphohistiocytic aggregates, or diffuse histiocytic infiltrates. Hemophagocytic syndrome has been reported.
Figure 13.13Candida albicansinfection, peripheral blood. Yeast forms and branching pseudohyphae are seen in this specimen from a patient with an indwelling catheter.
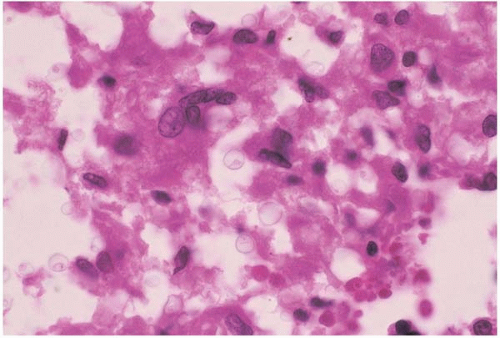
Histoplasma capsulatum may cause disseminated disease, especially in infants and immunosuppressed patients (Figs. 13.16 and 13.17) (122, 123, 124, 125, 126). Peripheral blood and bone marrow aspirate smears show small, intracellular, ovoid yeast forms within phagocytic cells. Depending on the level of immunosuppression, histologic sections of the bone marrow show granulomas, lymphohistiocytic aggregates, or sheets of histiocytes with abundant intracellular and free-lying organisms. Hemophagocytic syndrome has been reported. The differential diagnosis includes disseminated penicilliosis marneffei.
Paracoccidioides brasiliensis, the agent of South American blastomycosis, affects normal individuals and immunocompromised patients in endemic areas (127, 128, 129). The peripheral blood may show anemia, leukocytosis, eosinophilia, and thrombocytopenia. The bone marrow may show eosinophilic hyperplasia, increased histiocytes with phagocytic activity, and granulomas containing yeast forms.
Figure 13.14Cryptococcus neoformansinfection, bone marrow aspirate. Encapsulated, free-floating yeast forms are present in this specimen from a patient infected with human immunodeficiency virus.
Figure 13.15Cryptococcus neoformansinfection, bone marrow biopsy. Encapsulated free-floating yeast forms appear among histiocytes in this specimen from a patient infected with human immunodeficiency virus.
Penicillium marneffei is an important opportunistic pathogen of immunosuppressed patients residing or traveling in Southeast Asia (130, 131, 132, 133). Cytopenias may be present. The peripheral blood and bone marrow aspirate may show intracellular yeast within phagocytes. Depending on the degree of immunosuppression, the bone marrow may show granulomas, lymphohistiocytic aggregates, or sheets of yeast-laden histiocytes. Hemophagocytic syndrome has been reported. The morphologic appearance of the organism may be mistaken for Histoplasma capsulatum; a differential point is that Histoplasma organisms divide by budding and Penicillium organisms by fission.
Pneumocystis jirovecii (formerly Pneumocystis carinii) may disseminate to involve the bone marrow in immunosuppressed patients (134, 135, 136). Bone marrow aspirate smears and histologic sections show a foamy exudate containing rare unicellular organisms. Hemophagocytic syndrome has been reported.
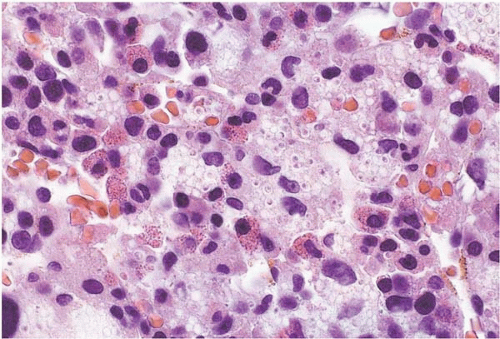
Figure 13.16Histoplasma capsulatuminfection, peripheral blood smear. Neutrophils containing ingested yeast forms are present in this specimen from a patient infected with human immunodeficiency virus.
Figure 13.17Histoplasma capsulatuminfection, bone marrow biopsy. Histiocytes filled with yeast forms are present in this specimen from a patient infected with human immunodeficiency virus.
Trichosporon spp. may cause disseminated disease in an immunocompromised host (137, 138, 139). The bone marrow may show budding yeast forms and hyphae. Hemophagocytic syndrome has been reported.
Only gold members can continue reading. Log In or Register to continue