Clinical Photograph Photograph shows a medium-sized infantile hemangioma on the face of a female infant. Most of these lesions are located in the head and neck region. (Courtesy J. Hall, MD.)
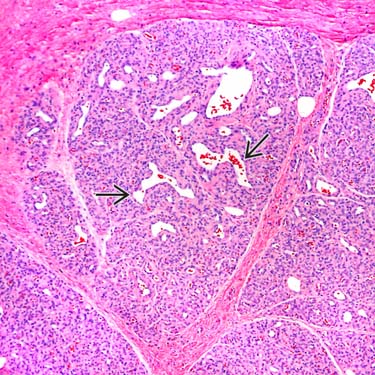
Infantile Hemangioma: Lobular Growth Low-power examination reveals multiple lobules composed of tightly packed capillaries, separated by fibrous septa. Note the scattered, centrally located feeding and draining vessels .
Facial Infantile Hemangioma Facial infantile hemangioma is seen in a patient with PHACES (posterior fossa malformations, hemangiomas, arterial and cardiac anomalies, eye abnormalities, and sternal cleft raphe). (Courtesy S. Yashar, MD.)
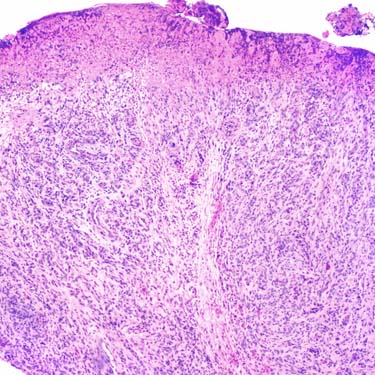
Infantile Hemangioma: Ulcerated The skin overlying infantile hemangioma may ulcerate, resembling an inflamed granulation tissue or pyogenic granulomas. The sharp separation between the 2 nodules of proliferating capillaries is a useful diagnostic clue.
TERMINOLOGY
Synonyms
• Hemangioma of infancy
• Juvenile hemangioma
• Cellular hemangioma of infancy
• Strawberry nevus/hemangioma
Definitions
• Benign proliferations of endothelial tissue; represent most common tumors arising in neonatal period
• Vascular neoplasm of infancy with characteristic onset, rapid growth, and spontaneous involution
• Does not include congenital hemangiomas, as they are clinically, histologically, and immunohistochemically distinct from infantile hemangiomas
Both below are negative for GLUT1 and Lewis-Y antigen
– Rapidly involuting congenital hemangioma
– Noninvoluting congenital hemangioma
CLINICAL ISSUES
Epidemiology
• Incidence
Most common tumor of infancy
Affects ~ 4% of children
• Sex
F > M
• Ethnicity
Caucasians more frequently affected
Site
• Skin and subcutis
Head and neck (60%)
Extremities, trunk, and genitals
• Viscera
Presentation
• Appears within 1st few weeks after birth
Blanched telangiectatic area
Natural History
• Rapidly enlarges over several months
Maximum size usually achieved by 6-12 months
• Hemangiomas typically achieve 80% of their final size by end of early proliferative phase
Occurs at mean age of 3.2 months
• Regresses over several years
75-90% involute by age 7 years
Treatment
• Options, risks, complications
Propranolol
Corticosteroids
Pulsed dye laser
Surgical excision
Watchful waiting
– Small innocuous lesions
Interferon-α
– Restricted to life-threatening lesions
Topical imiquimod
Prognosis
• Excellent; all eventually spontaneously regress
MACROSCOPIC
General Features
• Crimson-colored multinodular mass
• Can start out as flat red or purple patch, frequently less than 5 cm in diameter
• Then gradually enlarges and develops raised surface
MICROSCOPIC
Histologic Features
• Multiple lobules composed of tightly packed small- to medium-sized capillaries
• Early lesions
Plump endothelial cells that line small vascular spaces
Inconspicuous vascular lumina
Distinct lobules separated by normal stroma
Moderate mitotic activity and scattered mast cells
• Mature lesions
Small vessels lined by flattened endothelial cells
Only gold members can continue reading. Log In or Register to continue
 .
.